




Nursing Leadership, 26(Special Issue) May 2013: 52-60.doi:10.12927/cjnl.2013.23361
The Effectiveness of Superficial Subcutaneous Lidocaine Administration Prior to Femoral Artery Sheath Removal
Laura Davison, Anne McVety and Tara Oke



Abstract
The dynamic world of healthcare requires continuous review of practice to ensure that patient care aligns with current evidence and best practice. Superficial subcutaneous lidocaine injection has been an order option at London Health Sciences Centre – University Hospital (LHSC-UH) for use in post-percutaneous coronary intervention (PCI) prior to femoral artery sheath removal (FASR). The purpose of administering lidocaine is to reduce pain during FASR, subsequently enhancing the patient's experience. A critical appraisal was performed by the Continuous Quality Improvement – Cardiac Care Council (CQI-CCC) at LHSC-UH, evaluating the effectiveness of superficial subcutaneous lidocaine for use in patients undergoing FASR. This paper details the process followed to evaluate this practice and reports on the subsequent findings and recommendations. A literature review, a retrospective chart audit, a blinded online survey and peer hospital polling were compiled, and a summary of findings was shared with the cardiac interventionists, with subsequent polling. No significant evidence for pain reduction was identified when lidocaine injections were administered prior to FASR. As such, a unanimous decision was reached to remove lidocaine from the LHSC Coronary Angioplasty Clinical Pathway order form.
Introduction
In order to perform a post-percutaneous coronary intervention (PCI), access to an artery is required. A percutaneous sheath is used to gain access to the radial or femoral artery, thus allowing therapeutic instruments to be inserted into the artery and guided towards the stenosed area. This is necessary in order to conduct the required lifesaving intervention. After the procedure is completed, the sheath remains in situ until it is safe to remove without risking complications related to bleeding. Depending on the medications administered during the procedure, the removal criteria may vary. The criteria include either (a) achieving a specified time frame (i.e., two hours post-procedure) or (b) results of blood work indicating an activated clotting time (ACT) value within prescribed limits. If either of the criteria for sheath removal has been achieved, the most qualified healthcare professional will perform the procedure. At LHSC-UH interventionists are responsible for removing radial artery sheaths, while qualified registered nurses remove the femoral artery sheaths. FASR is an added nursing skill; the registered nurse performing the procedure must have completed additional education and clinical training.
At LHSC-UH, FASR is accomplished by applying manual pressure or using a C-clamp to the groin region. During removal, sufficient pressure is applied proximal to the puncture site to promote hemostasis of the arterial puncture. This pressure is gradually eased, on average taking between 20–40 minutes, dictated by ongoing patient assessment. This procedure is slightly uncomfortable for most patients; however, it can be painful for others related to patient-specific factors and the diminished effect of local anesthaesia by the time removal is initiated.
Background
One option listed on the pre-printed LHSC Coronary Angioplasty Clinical Pathway order sheets is to administer superficial subcutaneous lidocaine prior to FASR. However, this practice was not routinely ordered and was seldom administered by the registered nursing staff. This finding raised questions among the members of the CQI-CCC, including: Was superficial subcutaneous lidocaine effective in pain management during FASR? Was a localized pain regimen beneficial versus a systemic pain regimen? Why were the registered nurses not administering lidocaine when it was ordered? Would further education on superficial subcutaneous lidocaine injection change medication administration rates and thus improve patients' experience? To answer these questions and to determine current best practice, the CQI-CCC initiated an investigative review of current literature regarding this practice.
Literature reviews were compiled by an LHSC clinical librarian using the search words "(femoral [ti] OR femoral artery [mh]) AND (lidocaine [mh] OR lidocaine [ti] OR lignocaine [ti] OR anesthetics, local [mh]) AND (pain [mh] OR device removal [mh])" in the National Center for Biotechnology Information PubMed and "MH sheath removal+ and (MH treatment related pain+ or MH lidocaine OR TI lidocaine or MH anesthetics, local+)" in Ebsco Publishing CINAHL. This search identified studies with involvement of superficial subcutaneous lidocaine administration and its effectiveness prior to FASR.
Within the literature, an applicable Cochrane Database review was found titled, "Pain Relief for the Removal of Femoral Artery Sheath After Percutaneous Coronary Intervention" (Wensley et al. 2011). Four studies involving a total of 971 participants were included in the review. Of the 971 participants, 498 were involved in studies that analyzed pain scores of patients given subcutaneous lidocaine injections versus control (null) treatment. The review concluded there was no statistically significant change in pain scores between patients given subcutaneous lidocaine injections prior to FASR versus the control group; mean difference (MD), 0.12 (95% confidence interval [CI] –0.46 to 0.69) (Wensley et al. 2011). The report stated that "in all groups the pain intensity was relatively mild with mean pain scores ranging from 1.88 to 4.10 in the [lidocaine] groups and 2.67 to 3.67 in the control group" (Wensley et al. 2011: 9). The reviewers went on to suggest that significant pain reduction scores were discovered with other regimens, including intravenous pain regimens, that were not observed in the lidocaine trials. Moreover, the reviewers acknowledged the need for further studies as not all treatment arms were properly blinded and study sizes were small. Overall, the literature review did not support the current administration practice of superficial subcutaneous lidocaine injections to reduce patient pain and improve the patient experience during FASR. Further investigation was necessary to determine best practice and thus alter current practice accordingly.
Design and Implementation
Several methods of evaluation were used to determine current best practice associated with superficial subcutaneous lidocaine injections prior to FASR. A survey was conducted with nurses working within the Cardiac Program, including Inpatient Cardiology, the Cardiac Day/Night Unit (CDNU) and Coronary Care Unit (CCU) on the fifth floor of LHSC-UH. The questionnaire explored nurses' comfort with administering superficial subcutaneous lidocaine and rates of administration. This was a blinded online survey that was distributed to the nurses' confidential intranet email accounts on the LHSC GroupWise server. The nurses were notified of the survey via emails and were provided written instructions and information regarding the study objectives. The survey data were accumulated and subsequently displayed in a table format. Retrospective patient chart audits were completed to determine rates of ordering and administration. The chart audits were blinded and randomized, with data collected on analgaesia orders and/or administration of analgaesia prior to FASR. Patient chart audit analysis was configured into graph format. Three peer hospitals were polled to inquire about their current practice. Hamilton Health Sciences, Ottawa Heart Institute and St. Michael's Toronto were contacted through email or telephone. Two educators and an interventionist were questioned on FASR practices in their respective hospitals. A summary of findings was shared with the cardiac interventionists at LHSC-UH, with subsequent polling to determine future action based on current research and accumulated data. Practice changes were then initiated with regard to patients' receiving FASR at LHSC-UH, supported by current practice and evidence identified through these methods of evaluation.
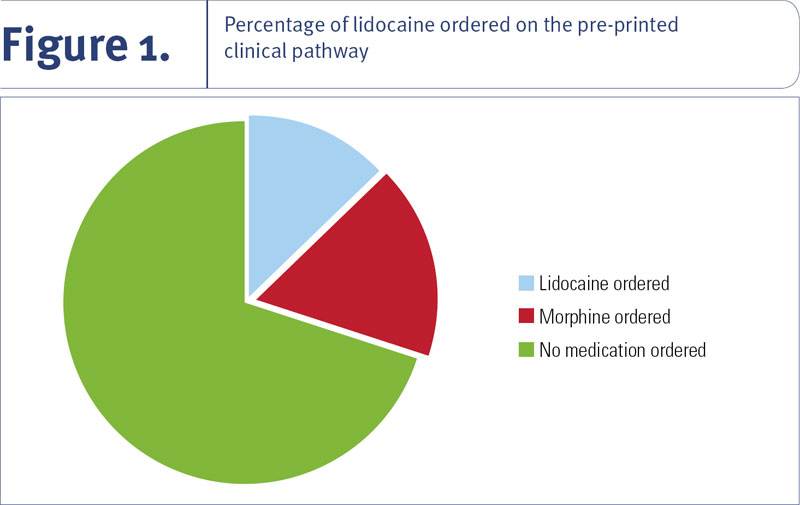
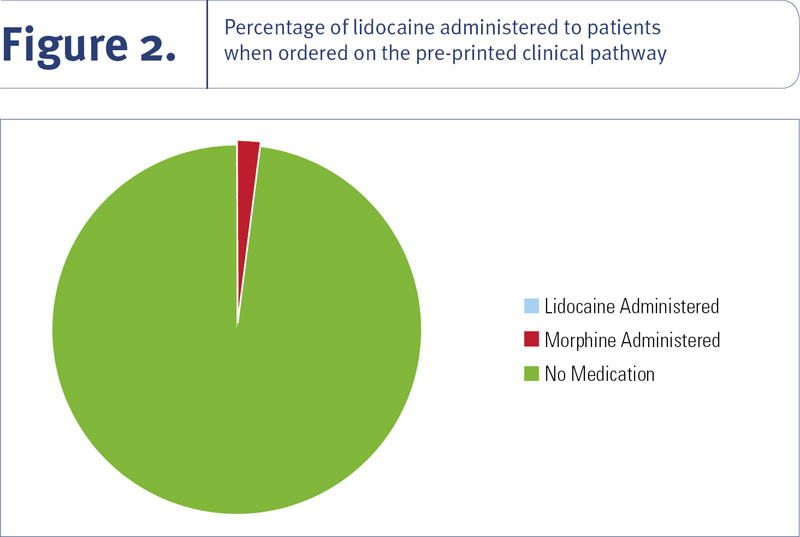
In the randomized retrospective chart audit, 24 charts from the Cardiac Day/Night Unit and the Cardiac Care Unit at LHSC-UH were reviewed for the number of times superficial subcutaneous lidocaine injection and morphine intravenous injection were selected on the pre-printed order sheet (see Figure 1). Included in this review was the number of medication administration records (MARs) that demonstrated the administration of lidocaine or morphine prior to FASR. The chart audits revealed that 17% ordered superficial subcutaneous lidocaine, yet out of those 17%, no lidocaine injections were administered to the patients (see Figure 2). Morphine intravenous injections were ordered in 25% of the time, yet out of those 25% only one injection was administered. These findings confirmed the limited use of lidocaine for FASR at LHSC-UH and also highlighted the limited use of morphine for this procedure. The findings identified the need for further research into the practice of administering superficial subcutaneous lidocaine prior to FASR. They also suggested that the use of morphine injection be investigated for efficacy of patient analgaesia post-FASR, as it is infrequently ordered and seldom administered.
In search of a rationale to explain why superficial subcutaneous lidocaine injections were not being administered, a blinded online survey was sent to all registered nurses working in the cardiac care units where nurses were trained and qualified to perform FASR. Forty-three surveys were completed by the closing date. Three questions were listed on the yes/no blinded survey:
- Do you feel proficient in using subcutaneous (SC) lidocaine for femoral artery sheath removal (FASR)?
- Do you feel you need more education to use SC lidocaine for FASR?
- If you were to be provided with additional education re SC lidocaine, would you be more willing to use it?
Of the 43 respondents, 74% stated they did not feel proficient in SC lidocaine administration, 52% stated they did not require further education on the skill and 65% stated they would not use lidocaine if given additional education (see Table 1). With these results, the members of the CQI-CCC concluded that staff nurses in the areas performing FASR did not feel proficient in the skills required to administer lidocaine. However, with additional education, which 48% determined would be required prior to performing the skill of administering lidocaine, the majority (65%) indicated they still would not change their practice and administer lidocaine. This finding may indicate that staff nurses do not observe a significant benefit to patients. This interpretation was validated when the additional comments section at the end of each survey was reviewed. Therefore, the survey revealed that the primary reasoning behind the limited use of lidocaine injection was that nurses did not find lidocaine injection to have enough of a therapeutic effect on patients' experience of pain to warrant its use prior to FASR.
| Table 1. Blinded online nursing survey. This table illustrates the proficiency and need for lidocaine administration education among the nursing staff in the Cardiac Care Program at LHSC-UH. | ||
| Blinded Survey Questions | Response 'Yes' | Response 'No' |
| Proficiency in administering lidocaine subcutaneous (SC) for femoral artery sheath removal (FASR) | 11 | 32 |
| Further education required to adminster lidocaine SC | 21 | 23 |
| Willingness to utilize lidocaine if education provided | 15 | 28 |
To further investigate current best practice regarding the use of superficial subcutaneous lidocaine, three peer hospitals providing tertiary cardiac care were polled. These hospitals were Hamilton Health Sciences, Ottawa Heart Institute and St. Michael's Toronto. Clinical educators at the first two hospitals and an interventional Cardiologist at the latter were contacted through emails and telephone.
Hamilton Health Sciences' clinical nurse educators completed a study, "To Freeze or Not to Freeze? A Randomized Controlled Pilot Trial" (Cook et al. 2008), assessing the efficacy of administering subcutaneous lidocaine to decrease pain and reduce the vasovagal response prior to FASR. Analysis of the data showed that the pain scores among the control and intervention arms were low. Based on the study findings, and Hamilton Health Sciences' own literature review, lidocaine injections were removed from their post-PCI order sets (Cook et al. 2008).
Telephone contact with the clinical nurse educator from Ottawa Heart Institute provided the information that lidocaine was replaced with the administration of intravenous fentanyl (25 μg) and intravenous midazolam (1–2 mg) to enhance the patient experience and alleviate discomfort and pain (personal communication, October 12, 2012).
A cardiac interventionist from St. Michael's Hospital in Toronto was also contacted by phone. The cardiac catheterization lab at St. Michael's Hospital prepares patients for cardiac procedures and sees them through recovery after these procedures are performed. Patients who undergo a PCI require intravenous medications to prevent clot formation during the procedure. Following their PCI, patients are recovered in this unit, receiving a dose of intravenous protamine sulphate to reverse the anticoagulant effect of the medications given during the PCI. Trained staff are then able to perform FASR immediately following the PCI using a technique employed at LHSC-UH that restores haemostasis to the insertion site using pressure (personal communication, October 12, 2012). This approach obviates the need for lidocaine injection as the sheaths are pulled while the effects of the local anaesthesia are still intact.
With the evidence gathered and summarized, the interventional cardiologists were polled to determine whether superficial subcutaneous lidocaine should continue as an order option on the pre-printed order sheet, LHSC Coronary Angioplasty Clinical Pathway, for administration prior to FASR. The votes were unanimous in the decision to remove this practice from the order sheet.
The research process carried out by the CQI-CCC – including a literature review, a blinded online nursing survey, a retrospective randomized chart audit and peer hospital polling – identified many different factors affecting the limited use of superficial subcutaneous lidocaine, including lack of proficiency and confidence among the nursing staff regarding its administration, clinical perception of minimal benefit to the patient and ultimately, limited use of the order option by the interventional cardiologists' at LHSC-UH. Furthermore, the literature reported only a small increase in pain scores during the FASR procedure and supportive evidence that peer hospitals within Ontario had removed lidocaine injections for this reason. Therefore, this study confirmed the need to change practice based on the identified current evidence and best practice, in order to continue to provide high-quality patient care within the PCI program at LHSC-UH.
Objectives
Although the purpose of this study was to gain an understanding of why superficial subcutaneous lidocaine was not routinely ordered and administered prior to FASR, the overriding objective was to incorporate current evidence-based research into best practice, ensuring a safe, comfortable and positive patient experience.
Positive Outcomes
The definitive decision was made to eliminate the practice of superficial subcutaneous lidocaine injections post-percutaneous coronary intervention and prior to FASR at LHSC-UH based on the listed evidence. Cessation of superficial subcutaneous lidocaine injections is expected to reduce patient risk of pain and complications related to receiving the lidocaine injection, consequently improving patient safety, outcomes and satisfaction. Moreover, removing this additional nursing procedure means a reduction of time allotted for these interventions, therefore improving service efficiencies.
Challenges and Recommendations
Upon study review, the CQI-CCC identified areas that could have been enhanced. Owing to staff's limited research experience, a research proposal was not presented to the Western University Office of Research Ethics committee and therefore, chart audits could be performed only retrospectively. The limited number of chart audits (24) and number of peer hospitals polled (3) by the CQI-CCC provided a very small sample size. Increasing the size of the study would have provided greater confidence in the findings. In hindsight, the added collection of patient pain scores during the chart-auditing phase would have complemented the results. The treatment arms listed in the Cochrane Database of Systematic Reviews had notably small study sizes and limited blinding procedures, suggesting that additional studies are required (Wensley et al. 2011). In addition, these studies compared administration of subcutaneous lidocaine with intravenous interventions, which may have influenced the identified outcomes (Wensley et al. 2011). A further recommendation would be to investigate patient benefits related to the administration of intravenous morphine prior to FASR: the literature suggests significant pain score reductions with intravenous interventions (Wensley et al. 2011), yet IV morphine is infrequently ordered or administered at LHSC-UH.
Conclusion
This paper demonstrates how the CQI-CCC at LHSC-UH effectively identified an area for inquiry and completed a critical appraisal resulting in a practice change to improve patient care outcomes and experience. Overall, the study concluded that superficial subcutaneous lidocaine injections were not found to reduce patient pain scores significantly (Wensley et al. 2011), were not consistently ordered or administered at LHSC-UH and have been removed from practice at peer hospitals in the same region. Presentation of the data resulted in the interventional cardiologists' unanimous agreement to remove superficial subcutaneous lidocaine injection from the pre-printed order sheet LHSC Coronary Angioplasty Clinical Pathway, and subsequently from practice. Members of the CQI-CCC remain dedicated to identifying areas of practice that require change based on current research and best practice.
About the Author
Laura Davison, RN, BScN, Acute Care Nurse, Cardiac Care Program & Chair, CQI Council, 2012–2014
Anne McVety, RN, BHSN, CCN(C), Professional Scholarly Practice Clinical Educator, Cardiac Care Program, London Health Sciences Centre – University Hospital
Tara Oke, RN, CCN(C), Professional Scholarly Practice Clinical Educator, Cardiac Care Program, London Health Sciences Centre – University Hospital
Correspondence may be directed to: Anne McVety, Cardiac Clinical Educator, Nursing Professional Scholarly Practice, London Health Sciences Centre, University Hospital, 339 Windermere Road, PO Box 5339, London, Ontario, N6A 5A5; e-mail: Anne.mcvety@lhsc.on.ca
Acknowledgment
We would like to thank everyone who contributed to this project, demonstrating their dedication to providing high-quality patient care, aligning with current evidence and best practice in the Cardiac Care Program at LHSC-UH. Special thanks to the CQI-CCC 2011/2012 membership, specifically Tina Dyck, RN, BScN, Tina Davidson, RN, BScN and JoAnn Richardson, RN, for their significant commitment and direction in this project.
We would also like to thank Sylvia Katzer, BA, MLS, Clinical Librarian at LHSC for her expertise in conducting our literature searches; Michèle Nelson, RN, BScN, Nurse Educator at University of Ottawa Heart Institute; Tammy Cosman, RN(EC), PhD, Hamilton Health Sciences Centre; and our peer hospitals, Hamilton Health Sciences, Ottawa Heart Institute and St. Michael's Hospital, Toronto, for supporting us in our search for current evidence and best practice.
References
Cook, A., T. Cosman, L. Gauthier and M. Quirk. 2008. "To Freeze or Not to Freeze? A Randomized Controlled Pilot Trial." Hamilton, ON: Hamilton Health Sciences.
Wensley, C., B. Kent, M.B. McAleer, S.M. Savage and J.T. Stewart. 2008. "Pain Relief for the Removal of Femoral Sheath After Percutaneous Coronary Intervention (Review)." Cochrane Database of Systematic Reviews 4(9). doi: 10.1002/14651858.CD006043.pub2.
Comments
Be the first to comment on this!
You must sign in to comment Sign In or Create an Account to add comments
Related Content
HealthcarePapers
HealthcarePapers
Reform, Rather than Discard the WHO
Nursing Leadership
