
Healthcare Quarterly
Transfer of Accountability: Transforming Shift Handover to Enhance Patient Safety
Abstract
Communication of information between healthcare providers is a fundamental component of patient care. The information shared between providers who are changing shifts, referred to as "handover," helps plan patient care, identifies safety concerns and facilitates continuity of information. Absent or inaccurate information can have deleterious effects on patient care. According to the Joint Commission on Accreditation of Healthcare Organizations (JCAHO 2003), almost 70% of all sentinel events are caused by breakdown in communication. Issues and concerns regarding the effectiveness of handover at shift change were raised by nurses throughout Hamilton Health Sciences (HHS), leading to the approval of a hospital-wide project to implement evidenced-based Transfer of Accountability (TOA) Guidelines and a bedside patient safety checklist. This article describes the development of the guidelines, the results of the pilot study and the ongoing implementation of the project. The observed impact on patient safety within HHS is presented.
Background
Reporting mechanisms employed when providers change shifts are an integral component of the communication process used to convey information about patients between healthcare providers. A number of terms are used to describe this exchange of information, such as patient care handover, transfer of accountability, bedside reporting, and shift handover. The information imparted during this exchange is fundamental to the professional activities that follow, and consequently to the care the patient receives (Dowding 2001; Kerr 2002; Miller 1998). Inadequate or incorrect information jeopardizes patient safety and the continuity of care (Anthony and Preuss 2002).
Many Canadian hospitals have no policy or standards for handover. Transfer of accountability (TOA) practices vary across and within healthcare organizations. Typical procedures involve spoken, written and/or taped reports (Dowding 2001; Greaves 1999; Kerr 2002; Pothier et al. 2005; Timonen and Sihvonen 2000; Williams 1998). When the process for this transfer varies between settings or healthcare providers, the risk of missed or incorrect information is elevated. The potential impact of inadequate or erroneous information on patient care is troubling. The Joint Commission International Center for Patient Safety (JCICPS) contends that effective communication is the "hallmark of health care organizations that are successful in providing safe, high-quality care" (JCAHO 2004). The JCICPS goes on to suggest that systems and processes must be established to ensure complete communication of information. The Canadian Council on Health Services Accreditation suggests patient safety can be improved by employing "effective mechanisms for transfer of information at interface points, including shift changes …" (CCHSA 2005). The Canadian Patient Safety Institute (CPSI) has recognized the importance of this issue, designating implementation and evaluation of new mechanisms for communication within and between caregivers as a research priority (2006).
At Hamilton Health Sciences (HHS), prior to the implementation of the TOA project, methods used for transferring patient accountability between care providers differed. Concerns related to the usefulness of the information and congruence between the report and the patient condition were raised. As a result, a team of nurses with expertise in practice, policy and research related to patient care communication was established under the auspices of the HHS Professional Affairs portfolio. Using the best available evidence supporting bedside reporting, and through a process of consensus, TOA guidelines were developed. The guidelines were pilot-tested and subsequently implemented in units with shift handovers across the organization.
Objectives
The objectives of the TOA project were to review the handover processes at HHS, develop TOA practice guidelines, provide an appropriate framework through which nurses can handover patient care, implement a standardized approach to TOA and evaluate the effect of the project on patient safety within HHS.
Setting
Hamilton Health Sciences (HHS) is a 1,000-bed regional tertiary care facility comprising five distinct hospitals and a cancer centre, serving more than 2.2 million residents of Hamilton and Central South and Central West Ontario. The facility employs over 3,400 registered nurses (RNs) and registered practical nurses (RPNs) who are actively involved in communicating patient information between nurses at shift change, and between units and hospitals when transferring patients.
The Transfer of Accountability Project
Development of TOA Guidelines
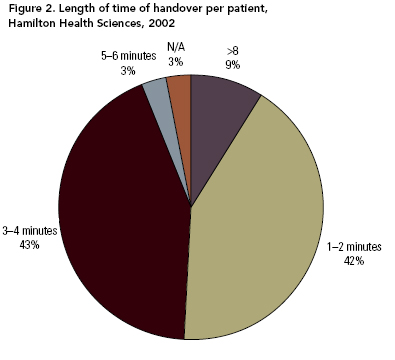
Assessment of current practice. The first phase of the project was to determine the current handover practices within the organization. In 2002, a survey was conducted, the aim of which was to determine both the handover practices of nurses and the length of time involved at shift change. The survey was distributed to the clinical educators for each of the 52 inpatient areas; responses for 36 units (69%) were received. Analysis of the responses revealed that nine different shift-reporting mechanisms were being used, including combinations of verbal, taped and written methods (see Figure 1). Length of handover ranged from as little as one or two minutes per patient on a ward to more than six minutes per patient in critical care areas (see Figure 2).

 Development of TOA practice guideline. An expert panel of nurses including administrators, educators and clinicians reviewed over 25 relevant research and opinion articles related to patient handover. The literature suggested that typical transfer procedures involve spoken, written and/or taped reports, and that these reports play a pivotal role in the continuity of patient care (Dowding 2001; Kerr 2002; Miller 1998). Young et al. (1988), in a study aimed at improving the communication of patient information at change of shift, found that a hybrid approach - verbal report, coupled with a silent report when patients' notes were read - facilitates the transfer of information necessary for safe and holistic care.
Development of TOA practice guideline. An expert panel of nurses including administrators, educators and clinicians reviewed over 25 relevant research and opinion articles related to patient handover. The literature suggested that typical transfer procedures involve spoken, written and/or taped reports, and that these reports play a pivotal role in the continuity of patient care (Dowding 2001; Kerr 2002; Miller 1998). Young et al. (1988), in a study aimed at improving the communication of patient information at change of shift, found that a hybrid approach - verbal report, coupled with a silent report when patients' notes were read - facilitates the transfer of information necessary for safe and holistic care.
On the basis of this literature, practice guidelines were drafted. The guidelines identify and expand upon the three distinct phases of TOA: pre-handover, inter-shift handover and post-handover. Within the pre-handover phase, a review of patient information is obtained from the chart, team members, patient and family; a written report capturing the key pieces of information about the patient is prepared. The format of this report, including content, can differ for patient care units, according to the information needs of care providers. During inter-shift handover, the off-going and the on-coming nurses engage in a verbal report and complete a patient safety checklist at the bedside. Following this, the on-coming nurse reviews the patient plan of care, medication record and summary work plan, e.g., kardex.
Pilot study. Two clinical inpatient units, a 16-bed general medicine unit and a 34-bed obstetrical unit participated in the pilot study. Orientations were held to familiarize the nurses with the TOA guidelines. Nurses were provided with an information package on each unit, and support was provided through e-mail and telephone contact. Four months following implementation of the TOA guidelines, a questionnaire was developed and structured to determine the frequency and perceived usefulness of completing each component of handover. Responses were obtained from 57 of the 59 (97%) registered nurses and registered practical nurses working on these units. Analysis revealed that, overall, nurses were completing the written and verbal handover as per the new TOA guidelines. At times, they were choosing to conduct the face-to-face component in the hall outside the patient's room. While each unit implemented the three phases of the TOA process, they modified the inter-shift handover. Nurses excluded the bedside safety checklist, because the process had not yet been clearly defined.
Analysis also revealed that nurses on each unit perceived the usefulness of the written tools differently. One unit used a generic computer-based form; the nurses on the other unit developed their own form. Nurses chose to modify the written tools to make them more appropriate for the particular unit. Analysis revealed that the form developed by the staff nurses was perceived as much more useful than the generic form (p = 0.00, 2-tailed t-test).
The conclusion of the study was that nurses were not comfortable communicating nursing information during face-to-face interaction at the bedside. Face-to-face reporting needed to be introduced, along with education to enable nurses to use this component. Nurses were more accepting of the TOA guidelines when they were involved in the development or identification of written tools for the staff nurse and charge nurse. Needed were patient-population-specific components of the TOA standards. The importance of a bedside patient safety check needed to be communicated.
The results and conclusions were disseminated to the HHS executive team, who decided that further development and implementation was warranted. An implementation plan, including guiding principles and a staged implementation, was suggested.
Implementation Plan
A TOA Advisory Committee convened to review the practice guidelines and the pilot study. The Advisory was made up of nurse leaders, a patient safety specialist, a clinical educator, a clinical system professional and staff nurses. They determined that the introduction of a bedside patient safety checklist, face-to-face dialogue and a written tool for both the charge nurse and the staff nurse would help nurses establish and maintain the principles of TOA. The Advisory adapted a one-page document, the "HHS Nursing Standards for Patient Safety during Transfer of Accountability" that had been drafted in response to the TOA guidelines by the HHS ICU Innovation and Learning project in 2004. This document, also known as the "TOA standards," outlined the process for TOA, including a review of patient history and plan of care, review of patient-population-specific information and completion of a bedside patient safety checklist (see Figure 3). Following this, a five-step plan for implementation of TOA was developed to ensure effective engagement of staff and support a sustainable transformation within the organization. A project coordinator was hired to assist nurses with the change in practice.
Guiding principles. The TOA Advisory Committee identified four guiding principles for the transfer of accountability process:
- A mechanism (safety checklist) to review key patient safety issues, identify errors and limit patient harm must be introduced.
- An opportunity to clarify information (face-to-face dialogue) must be included.
- Reliance on memory should be minimized through the use of a staff nurse written tool.
- One person must have a total picture of the unit through the use of a charge nurse written tool.
[Figure 3]
Five-step plan for implementation. The implementation plan was divided into five steps: (1) development of a patient-population-specific component of the TOA standards; (2) development or identification of written tools for the staff nurse and charge nurse; (3) introduction and implementation of the bedside patient safety checklist; (4) introduction of face-to-face reporting; and (5) evaluation. A two-hour, facilitated workshop was prepared for each step. Implementation teams consisting of a manager, an educator and a staff nurse were identified for each area that had shift handovers. Implementation team members attended the series of five workshops, during which they planned for implementation on their wards, developed a communication plan, drafted TOA standards and drafted written tools for the staff and charge nurses.
The TOA workshops were scheduled every two weeks, to allow members time to work with the nurses on the units to develop, review, test and revise their TOA standards, written tools and face-to-face reporting methods. This process helped to ensure the tools met the needs of the unit while remaining consistent with the guiding principles. Each workshop opened with storytelling from the members to foster collaboration and mutual problem-solving. The project coordinator followed up with members between meetings, offering to meet with staff and to assist with testing out the new tools and methods. The teams reconvened three months after the workshops to review progress and to celebrate successes.
Ongoing evaluation. A communication book was kept on the clinical units, in which nurses wrote questions and comments as TOA was implemented. One book exemplified the evolution in feelings and beliefs of the nurses as they implemented the practice change. Its first nine entries expressed frustration. A nurse stated she was "too busy" to report. Another suggested that using paper for the written report "was a waste of money." As the communication continued, the manner shifted. One nurse stated, "the checking of armbands is good, I had an incident where I was going off nights and checking an armband. The ID number did not match the patient armband and this patient was going to the OR that day." Another stated, "I feel doing TOA is helping everyone … we can get on with our jobs. Teamwork!" And another commented, "patients have been very positive regarding armband check and face-to-face reporting."
Observational audits are currently being conducted to evaluate the handover process. Unusual findings identified by the nurse at shift change are documented. Nurses are reporting improvements in the congruency of information received in handover and their patient assessment. Patients have expressed their satisfaction with the process, particularly the bedside check. They are reassured by knowing information about their care requirements has been communicated between nurses. Incorrect patient armbands and IV solutions have been identified and rectified during the bedside patient safety check. These early "catches" help limit patient harm, identify system issues to prevent future errors and help the organization reach its patient safety goals.
Plans to extend this project to explore TOA within and between other disciplines and facilities are under way. In addition, McMaster University School of Nursing is exploring ways to introduce TOA education into the undergraduate curriculum.
Implications for Patient Safety
The intent of this project was to develop handover practices to support patient safety. Prior to the TOA project, a lack of consistency in practice about appropriate nursing change of shift handover resulted in confusion about the appropriate information to communicate. Lack of communication of significant patient information among nurses sometimes led to an inappropriate plan of care and ultimately a negative outcome. The use of TOA guidelines, a relatively standardized approach, can decrease the chance of negative outcomes, because of the limits placed on the variety of methods used to perform a task (Porto 2001). Use of a structured tool can also stimulate recall for nurses, ensuring that assessment about key issues is conducted and the reporting of significant findings enhanced.
Conclusion
The purpose of the TOA project was to provide an evidence-based framework to support nurses' handover of patient care, and to implement a standardized approach to TOA to promote patient safety. TOA guidelines were developed, pilot-tested and evaluated. Results of the pilot study were used to inform clinical practice. This was achieved by developing nursing standards for patient safety during transfer of accountability and introducing written tools, a bedside patient safety checklist and face-to-face reporting. The standardized approach to TOA improves the effectiveness and coordination of communication among nurses at shift change, and fosters complete communication of information related to patient needs during provision of care. The next step of this project is to understand and enhance handover practices within and between other care providers and facilities.
About the Author(s)
Kim Alvarado, RN, BScN, Doctoral Student, is Chief of Nursing Practice at the Henderson and Chedoke Hospitals, Hamilton Health Sciences, Hamilton, ON.
Ruth Lee, RN, PhD, is Chief of Nursing Practice at the McMaster University Medical Centre, Hamilton Health Sciences, Hamilton, ON.
Emily Christoffersen, RN, BScN, is a Patient Safety Specialist, Hamilton Health Sciences, Hamilton, ON.
Nancy Fram, RN, BScN, MEd, is the Vice-President Professional Affairs and Chief Nursing Executive, Hamilton Health Sciences, Hamilton, ON.
Sheryl Boblin, RN, PhD, is an Associate Professor, McMaster University, Hamilton, ON.
Nancy Poole, RN, BScN, is an Education and Development Clinician and was the Coordinator for the Transfer of Accountability project, Hamilton Health Sciences, Hamilton, ON.
Janie Lucas, RN, BScN, MSc, is a Quality Improvement Specialist, Hamilton Health Sciences, Hamilton, ON.
Shirley Forsyth, MBA, is an Organizational Development Specialist, Hamilton Health Sciences, Hamilton, ON.
Please direct correspondence to: Kim Alvarado, Hamilton Health Sciences, Henderson Hospital, 711 Concession Street, Hamilton, ON, Canada, L8V 1C3. Tel: (905) 521-2100, ext. 43810; Fax: (905) 577-1409. E-mail: alvarkim@hhsc.ca.
References
The authors of the paper would like to acknowledge the dedication and commitment of the clinical managers and staff nurses at Hamilton Health Sciences. They supported and implemented the Transfer of Accountability initiative to improve communication and safety related to patient care.
References
Anthony, M.K. and G. Preuss. 2002. "Models of Care: The Influence of Nurse Communication on Patient Safety." Nursing Economics 20(5): 209-15.
CCHSA. 2005. "Patient Safety Goals: Required Organizational Practices and Evidence of Compliance" [announcement]. Canadian Council on Health Services Accreditation site. Retrieved August 7, 2006. http://www.cchsa.ca/pdf/PS GoalsandEvidenceJan05.pdf
Dowding, D. 2001. "Examining the Effects That Manipulating Information Given in the Change of Shift Report Has on Nurses' Care Planning Ability." Journal of Advanced Nursing 33(6): 836-46.
Greaves, C. 1999. "Patients' Perceptions of Bedside Handover." Nursing Standard 14(12): 32-35.
JCAHO. 2003. "Sentinel Event Statistics" [announcement]. March 31. Joint Commission on Accreditation of Healthcare Organizations site 16-5-2005. Retrieved August 7, 2006. http://www.jointcommission.org/SentinelEvents/Statistics
JCAHO. 2004. "Focus on Five: Strategies for Enhancing Physician-to-Physician and Staff-to-Physician Communication." Joint Commission Perspectives on Patient Safety 11(4). Available at Joint Commission on Accreditation of Healthcare Organizations site. Retrieved August 7, 2006. http://www.jcipatientsafety.org/show.asp?durki=9993
Kerr, M.P. 2002. "A Qualitative Study of Shift Handover Practice and Function from a Socio-Technical Perspective." Journal of Advanced Nursing 37(2): 125-34.
Miller, C. 1998. "Ensuring Continuing Care: Styles and Efficiency of the Handover Process." Australian Journal of Advanced Nursing 16(1): 23-27.
Porto, G.G. 2001. "Safety by Design: Ten Lessons from Human Factors Research." Journal of Healthcare Risk Management 21(3): 43-50.
Pothier, D., P. Monteiro, M. Mooktiar and A. Shaw. 2005. "Handover: Pilot Study to Show the Loss of Important Data in Nursing Handover." British Journal of Nursing 14(20): 1090-93.
Timonen, L. and M. Sihvonen. 2000. "Patient Participation in Bedside Reporting on Surgical Wards." Journal of Clinical Nursing 9(4): 542-48.
Williams, A.J. 1998. "Managing Change in the Nursing Handover." Nursing Standard 12(18): 39-42.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Note: Please enter a display name. Your email address will not be publically displayed