
ElectronicHealthcare
Low-Cost Rapid Usability Engineering: Designing and Customizing Usable Healthcare Information Systems
Abstract
Introduction
Although innovations in e-health have the potential to dramatically improve and streamline healthcare, there are a number of critical problems and issues related to their successful implementation and acceptance. One of the main areas of concern revolves around the following question: How can we ensure the healthcare information systems that we develop are suitable, meet information and workflow needs and are safe? The design of healthcare information systems that are intuitive to use and that support human information processing is essential. This has become increasingly recognized as critical, as more and more complex software and hardware applications appear in healthcare. Usability is a measure of how effective, efficient and enjoyable a system is. Closely related to issues of usability are issues of software safety and workflow, with the need to ensure that new devices and software increase patient safety and that workflow can be carried out in an effective and efficient manner.
This paper presents a case study detailing the development of a low-cost portable usability laboratory at the School of Health Information Science at the University of Victoria. The approach has been used to evaluate a variety of applications and devices ranging from PDA (Personal Digital Assistants) to Web-based information resources designed for both healthcare professionals and laypersons (Kushniruk 2002). In this case study, details are given about the initial setup, the costs associated with the purchase of equipment, the costs involved in conducting a typical usability study and the methods that are employed. Usability approaches to the evaluation of software and health information systems will be discussed, which can include testing of systems deployed in real-world settings such as clinics. In this paper, we will show how inexpensive yet powerful methods can be applied to rapidly testing healthcare information applications (i.e., rapid usability engineering) to build more suitable and safer health information systems.
Background: Usability Engineering in Healthcare
Over the past 15 years, the authors have been involved in adapting methods that are tried and true in the general software industry towards improving healthcare information systems. The methods are generally classified under the term "usability engineering." The main approach to usability engineering is known as usability testing (see Kushniruk and Patel 2004), which is a practical yet scientific approach to evaluating how usable our systems are and can also provide invaluable feedback to designers with ways of improving their usability, safety and workflow. The basic idea involves observing representative end users of a system (e.g., doctors or nurses) as they carry out representative tasks using a system (e.g., entering patient information into a patient record system). Observing users interacting with a system under study typically involves video recording all the user's interactions with the system (including video recording physical behaviour and also recording all the computer screens, as described below). In running such tests, the users of the system may be asked to "think aloud" or verbalize their thoughts as they use the system, while being video and audio recorded. Based on data collected this way from a representative sample of users (often involving as few as 5-10 participants), we have found that the majority of usability problems with a system can be identified and recommendations made for fixing them within a short period of time. We have used this approach to analyzing a wide range of healthcare information systems, ranging from studies of doctors using handheld PDA applications (e.g. prescription writers) to in-depth studies of problems with the user interface of medication order-entry systems. For example, in a recent study of a medication order-entry system, subjects were asked to enter prescriptions as accurately as possible into the system. By recording their activities in doing so, we were able to identify aspects of the user interface, ranging from content issues that needed to be changed to allow for accurate data entry (e.g., changing the default dosages provided to users to match dosages actually given in their hospital) to issues related to lack of consistency in the user interface (e.g., multiple ways to exit a screen, leading to confusion for new users).Setting Up a Portable Usability Laboratory
In the early stages of our work and early experimentation with usability engineering in healthcare, we employed a number of different approaches to conducting usability testing, including setting up a considerably more expensive "fixed" laboratory (where users would interact with systems in a fixed "wired" room with one-way mirrors). However, our experience has indicated that this approach does not allow us to collect data easily or rapidly at the site where the software under study is actually installed, which is often at a location not accessible (due to security restrictions, firewalls, etc.) from a fixed usability laboratory. In addition, for many of our studies, it is essential that we conduct them in the actual environment in which they are being employed (i.e., in order to determine how aspects of the particular environment may be affecting how users interact with a system), which is not realistically possible without employing a portable approach. With the advent of inexpensive screen recording software and high-quality portable digital video cameras, the costs have decreased for conducting such studies, along with an increase in the portability of the equipment that can be taken into any hospital or clinical environment, which also simplifies the entire process. It should be noted that all of the equipment we currently use (described below) can be physically carried in a small suitcase.Laboratory Set-up
To illustrate our approach and to make the point that usability testing methods described can be carried out rapidly in a cost-effective manner, in this section we will describe the set-up of a low-cost portable usability laboratory that has been set up at the School of Health Information Science at the University of Victoria. This laboratory set-up has so far been used for a number of projects, ranging from the study of nurses' information needs to its application in the evaluation of a new medication order-entry system (using bar-coding technology) by the authors.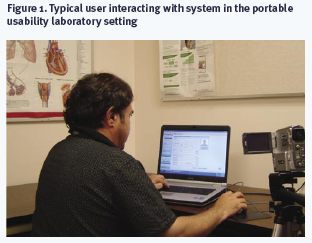
Figure 1 shows an example of a typical user (e.g. a physician) interacting with a system under study during usability testing of an electronic health record system. In this example, the subject interacted with the system to obtain information about a specific patient and was instructed to "think aloud" while doing so. The subject's overt physical activities were recorded using a Camcorder (a $500 Sony mini-DVD camera). In addition to recording physical activities and audio of the subject thinking aloud, the actual computer screens were recorded as a digital movie file, with the audio portion of the movie corresponding to subject's verbalizations. In order to do this, we are currently using a commercial software product called Hypercam© (approximately $60). Hypercam© allows one to record all the computer screens as a user interacts with the system under study, and stores the resultant digital movie for later playback and in-depth analysis of the interaction.
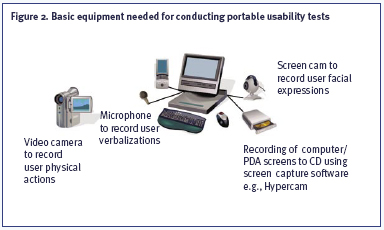
The equipment we currently use for our usability studies is shown in Figure 2. This typically includes (1) a computer to run the software under study (which might be run on a notebook or desktop in a hospital setting), (2) screen recording software (we are currently using Hypercam©), which allows the computer screens to be recorded as movie files (with audio input of the subject thinking aloud captured using a standard microphone plugged into the computer), (3) a digital DVD camcorder on a tripod to video record the user's physical interactions. In studies being conducted remotely, the equipment may also include a Webcam attached to the computer the user is interacting with. The studies we have conducted using this equipment have been carried out in a range of settings.
| Materials | Cost |
| Microphone | $50.00 |
| Mini-DVD or DV Camcorder | $500.00 |
| Standard notebook (for data collection) | $1,500.00 |
|
Software |
|
| Screen recording
software (e.g., Hypercam©) Transana© analysis software available free from www.transana.org |
$60.00 |
|
Total One-Time Equipment Set-Up |
$2,110.00 |
The typical costs we have incurred in conducting rapid portable usability tests of hospital systems (i.e., involving a typical study where 10 users of a healthcare information system are video recorded as they use the system, with basic analysis of the resulting data) is given below:
| Subjects and Personnel | Cost |
| Subject
Pay (assuming $50 for each subject for a one-hour session) |
$500.00 |
| Assistant - for data collection and analysis | $2,000.00 |
|
Materials |
|
| Tapes (digital and audio) | $250.00 |
|
Total Cost |
$2,750.00 |
The one-time cost of equipment needed is in the range of $2,000, with the costs of running a full usability study only slightly more (including the cost of an assistant for data collection and analysis), making usability engineering accessible to nearly all healthcare organizations.
Data Analysis
The analysis of the data collected (e.g., screens of user interactions, video recordings of users' problems) varies from informal analysis, which consists of simply playing back the movies of user interactions to identifying particular usability problems (e.g., where a user is unable to carry out a requested task) in the presence of designers, hospital staff, managers, etc. The analysis can also involve video annotation of the movie file using software such as Transana©(a freeware video annotation program that allows analysts to "mark up" and time stamp movies of user interactions with a system). The typical result of carrying out a usability test includes identification of specific usability problems (often in a meeting setting with system developers, customizers and hospital or management staff present). The intent of our work is typically to provide feedback about system usability to provide useful information to improve system design, deployment or customization in an efficient and rapid manner. Our most recent projects have involved applying usability engineering methods (including our low-cost portable approach) to identifying potential errors that may be caused by a system (e.g., inappropriate medication defaults in an order-entry system), or "induced" by poor design of a user interface (see Borycki and Kushniruk 2005; Kushniruk et al. 2005).Experiences to Date
We have carried out a number of studies of healthcare information system usability at varied locations with a number of organizations including Mt. Sinai Medical Center in New York, Columbia-Presbyterian Hospital and numerous commercial organizations. Some of the earliest work involved usability testing of a patient record system at Columbia-Presbyterian Hospital, where the methods described in this paper resulted in a tenfold decrease in the number of problems encountered by users of the system. The data collection and analysis was conducted in a cost-effective and efficient manner, with specific recommendations for system improvement being programmed and incorporated in an improved system within several hours to weeks from the time of data collection (Kushniruk et al. 1996). Usability problems related to issues such as lack of interface consistency, problems in representing time sequences and issues in matching user- specified terms to computer terms were identified. We have also employed a similar approach to detecting and correcting potential user problems and preventing medical error in a range of systems, including a handheld prescription writing program (Kushniruk et al. 2005), and more recently we have employed the method to determine how medical workflow may be inadvertently affected by introduction of a medication order-entry system (Borycki et al. 2006).Based on our experiences, this approach to setting up a portable usability lab typically involves several steps: (1) familiarizing oneself with the techniques and approaches that are possible (see Kushniruk and Patel 2004 for details) in healthcare, (2) setting up a low-cost portable usability laboratory, (3) choosing a project area that might of significance (e.g., to identify the major usability problems that users of a patient record system may be encountering), (4) working closely with clinical informatics staff, designers and management to show how system usability can be improved in an effective and cost-beneficial manner and (5) making alternations based on feedback.
Discussion
Usability analyses of healthcare systems may be carried out at various points within the development life cycle of healthcare information systems, ranging from selection of systems to design and later testing and/or customization of emerging IT solutions (Kushniruk 2002). It is currently recognized that there is a critical need for support and methods for creating more effective and practical systems from the perspective of end users of our systems. In this paper, we have presented an approach that is both cost-effective and can be rapidly deployed in a range of real-world settings (e.g., hospitals, clinics, etc.) to collect immediately beneficial data from users of systems. The approach described has successfully been employed for improving healthcare information systems in Canada, the US and internationally. It is essential for dissemination of these approaches that we strive to develop innovative methods that are both practical and cost-effective. Indeed, we fully expect the cost of the equipment to decrease and do not recommend expensive equipment investments. The argument for the need for such analyses extends not only to providing input to improve and refine usability of healthcare systems but also to ensure patient safety. Indeed, based on studies indicating that poorly designed healthcare systems may actually facilitate medical error (Koppel et al. 2005), organizations such as the Agency for Healthcare Research and Quality (AHRQ) have recently begun to promote the specific techniques described in this paper to ensure not only the usability, but also equally as important, to ensure the safety of our healthcare information systems.About the Author(s)
Andre W. Kushniruk is Associate Professor and Director, School of Health Information Science, University of Victoria. Email: andrek@uvic.ca
Elizabeth M. Borycki is Assistant Professor, School of Health Information Science, Adjunct Assistant Professor, School of Nursing, University of Victoria. Email: emb@uvic.ca
References
Borycki, E. 2005. "Identifying and Preventing Technology-Induced Error Using Simulations: Application of Usability Engineering Techniques." Healthcare Quarterly (8): 99-105.
Borycki, E., A. Kushniruk, S. Kuwata and J. Kannry. 2006. "Use of Simulation Approaches to the Study of User Needs and Error in Biomedical Informatics." Proceedings of the 2006 Annual AMIA Conference.
Koppel, R., J.P. Metlay, J. Cohen, B. Abaluck, R. Localio, S.E. Kimmel and B. Strom. 2005. "Role of Computerized Physician Order Entry System in Facilitating Medication Error." Journal of the American Medical Association 293: 1197-03.
Kushniruk, A. 2002. "Evaluation in the Design of Health Information Systems: Application of Approaches Emerging from Usability Engineering." Computers in Biology and Medicine 141-49.
Kushniruk, A. and V. Patel. 2004. "Cognitive and Usability Engineering Methods for the Evaluation of Clinical Information Systems." Journal of Biomedical Informatics 37: 56-76.
Kushniruk, A., V. Patel, J. Cimino and R. Barrows. 1996. "Cognitive Evaluation of the User Interface and Vocabulary of an Outpatient Information System." Proceedings of the 1996 Annual AMIA Conference, 22-26.
Kushniruk, A., M. Triola, E. Borycki, B. Stein and L. Kannry. 2005. "Technology Induced Error and Usability: The Relationship Between Usability Problems and Prescription Errors when Using a Handheld Application." International Journal of Medical Informatics 74: 519-26.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Note: Please enter a display name. Your email address will not be publically displayed