
Healthcare Quarterly
ICES Report: Unintentional Discontinuation of Long-Term Medications for Chronic Diseases after Hospitalization
Abstract
The Issue
Lifelong medication adherence is essential in promoting continued risk reduction from important adverse outcomes in patients with chronic diseases. Patients may stop taking their medications over time for a variety of reasons. One cause for non-adherence is the unintentional discontinuation of medications that can occur during high-risk periods of care transitions, when patient responsibility shifts from one physician to another.
These types of transitions commonly occur in hospitalized patients, particularly when care is transferred from the hospital-based physician to the usual primary care provider or specialist. Patients admitted to the intensive care unit (ICU) may be at an even higher risk of unintentionally discontinuing medications prescribed for chronic conditions since the focus in the ICU is on acute illnesses. As well, patients in the ICU may experience additional transitions of care during their hospital stay. It is during these transitions that failure in both the communication of important information and in the reconciliation of admission and discharge medications may result in medication non-adherence.
Little is known about these so-called errors of omission, whereby failure to provide indicated drug treatment may place individuals at risk for preventable adverse events. By acquiring more knowledge about these issues through focused research, effective strategies could be developed and targeted at closing these gaps in the continuation of patient care.
Study and Findings
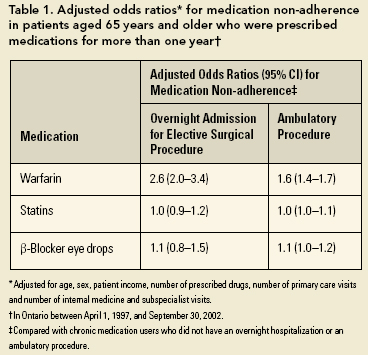
In two separate studies, scientists at the Institute for Clinical Evaluative Sciences (ICES) evaluated the unintended discontinuation of long-term medications in hospitalized patients with chronic diseases. The first study tracked over 233,000 Ontarians aged 65 years and older, with continuous use (one or more years) of warfarin (blood thinner), statins (cholesterol-lowering drugs) or betablocker eye drops between April 1, 1997, and September 30, 2002. Patients were assessed for continuation of the drug after overnight hospitalization for uncomplicated elective surgery. Warfarin is usually discontinued prior to surgery because of an increased risk of bleeding. In contrast, statins and eye drops do not have to be stopped before surgery.Those with an overnight hospitalization for elective surgeries were compared with those who had ambulatory or outpatient procedures, as well as with a control group who had no procedures. Patients prescribed warfarin were more than twice as likely to discontinue their drug after an overnight hospitalization for elective surgery, and more than one and a half times more likely to discontinue their drug after an ambulatory procedure, than those who had no procedures (Table 1). Undergoing a procedure did not affect the risk of unintended discontinuation of statins or eye drops.
The second study reviewed the hospital records of consecutive ICU patients at one academic and two community hospitals in Toronto during 2002. ICU patients who were prescribed at least one of six types of medications to treat chronic conditions before hospitalization were identified to determine the proportion of patients whose medications were unintentionally discontinued at hospital discharge (Table 2).
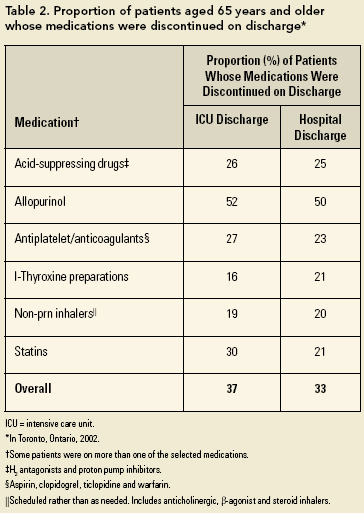
Of the 1,402 ICU patients, 834 had prescriptions for at least one of six types of medications used to treat chronic conditions. Thirty-seven percent of patients had one or more of their medications omitted at ICU discharge. Medications remained discontinued for more than 75% of this group on their subsequent discharge from the hospital. In total, 33% of the patients discharged from the ICU had their medications discontinued on hospital discharge.
What Do These Findings Mean?
Potentially unintended discontinuation of long-term medication for chronic diseases commonly occurs when patients are hospitalized. Indeed, it is increasingly recognized that transitions between healthcare settings represent vulnerable periods for medical error. Yet these types of medical errors are a distinct subset of "errors of omission" because these patients were already identified and treated for a disease with evidence-based therapies. Moreover, they were adherent to this treatment. The misfortune is that although these patients represented successful treatments from a hospital perspective - they survived ICU admission or elective surgery - these positive outcomes did not translate into additional success in the long-term management of their chronic diseases when they left hospital.Where Do We Go from Here?
These studies are among the first to underscore the notion that failure to restart long-term medications on transition of care may place patients at a greater risk of unintentional medication discontinuation on discharge from hospital. Our findings call attention to the need to develop a framework that focuses on reducing the unintended discontinuation of medications during healthcare transitions. Specifically, there should be an emphasis on better communication for the reconciliation of pre-admission and discharge medications at every transition of care.This goal can be achieved through the implementation of methods ranging in complexity from instituting standard medication lists upon admission to the ICU (which get transferred to relevant care units in the hospital) through to customized computerized systems. Hospital-based programs (e.g., the Safer Healthcare Now! medication reconciliation program) have been developed, but these interventions are only one part of an integrated model of communication and coordination for medication continuity. The success of all these initiatives relies on the involvement of hospital and community pharmacists, specialty and primary care physicians, nurses and the patients themselves.
Summary
Our present efforts are focused on identifying particularly high-risk individuals and medications that would be the best targets for intervention. As well, we will be working with stakeholders to devise evidence-based strategies to effectively promote and ensure medication continuity. In this way, hospitalization could provide an opportunity to encouragemedication adherence rather than be a contributor to its breakdown.About the Author(s)
Chaim M. Bell, MD, PhD, is an adjunct scientist at the Institute for Clinical Evaluative Sciences; a general internist and scientist at St. Michael's Hospital in Toronto; and an assistant professor of Medicine and Health Policy, Management and Evaluation at the University of Toronto. One of his main research interests is the continuity of patient care between the hospital and the community. Dr. Bell holds a Canadian Institutes of Health Research (CIHR) New Investigator Award. This work was partially funded by an operating grant from the CIHR. For more information, contact Chaim Bell at chaim.bell@ices.on.ca.
References
Bell, C.M., J. Bajcar, A.S. Bierman, P. Li, M.M. Mamdani and D.R. Urbach. 2006. "Potentially Unintended Discontinuation of Long-Term Medication Use after Elective Surgical Procedures." Archives of Internal Medicine 166: 2525-31.
Bell, C.M, P. Rahimi-Darabad and A.I. Orner. 2006. "Discontinuity of Chronic Medications in Patients Discharged from the Intensive Care Unit." Journal of General Internal Medicine 21: 937-41.
Coleman, E.A. and R.A. Berenson. 2004. "Lost in Transition: Challenges and Opportunities for Improving the Quality of Transitional Care." Annals of Internal Medicine 141: 533-36.
Cook, R.I., M. Render and D.D. Woods. 2000. "Gaps in the Continuity of Care and Progress on Patient Safety." British Medical Journal 320: 791-94.
Moore, C., J. Wisnivesky, S. Williams and T. McGinn. 2003. "Medical Errors Related to Discontinuity of Care from an Inpatient to an Outpatient Setting." Journal of General Internal Medicine 18: 646-51.
Safer Healthcare Now! Med Rec Intervention. Retrieved January 14, 2007. http://www.saferhealthcarenow.ca/
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Note: Please enter a display name. Your email address will not be publically displayed