
Healthcare Quarterly
Using ISMP Canada's Framework for Failure Mode and Effects Analysis: A Tale of Two FMEAs
Abstract
Patient safety concerns in healthcare are not new or unexpected, and one goal of all healthcare organizations is to provide the safest possible care for patients and their families. With that goal in mind, Annapolis Valley Health, a rural district health authority in Nova Scotia, identified the need to develop expertise in the use of failure mode and effects analysis (FMEA) as a tool to promote quality processes within the organization. Staff members were aware of the value of this type of analysis but also recognized that real learning would best be achieved through completing an FMEA of an existing process or situation, rather than through a simulation or staff training. Annapolis Valley Health identified two high-risk situations requiring attention: transcription of medication orders for in-patients and overcrowding in the emergency department. The Institute for Safe Medication Practices Canada provided training and support to two staff teams and visited the organization eight months later for an update on progress. This article chronicles the journey of Annapolis Valley Health to improve patient safety through the application of FMEA to two high-risk processes for one of its hospital sites.
In fall 2006, Annapolis Valley Health, in conjunction with another rural district health authority in Nova Scotia, engaged the Institute for Safe Medication Practices Canada (ISMP Canada) to provide training and support for a facilitated failure mode and effects analysis (FMEA). Each organization identified two healthcare processes associated with significant risks for patient safety and assembled a team for each process. This article chronicles the Annapolis Valley Health experience with the application of the ISMP Canada framework for FMEA (Institute for Safe Medication Practices Canada 2006) to two high-risk processes for one of its hospital sites.
FMEA is a team-based systematic and proactive approach for identifying ways in which a process or design can fail, why it might fail and how it can be made safer. FMEA is not a new concept, and it has been used for many years in a variety of industries to determine the potential effects of system and equipment failures. The automotive, chemical, aviation, nuclear power and aerospace industries all rely on FMEA as an essential aspect of improving safety and quality (McDermott et al. 1996). Completion of one proactive risk assessment project annually, using FMEA or a similar process, is now a required organizational practice for accreditation by the Canadian Council on Health Services Accreditation (2007).
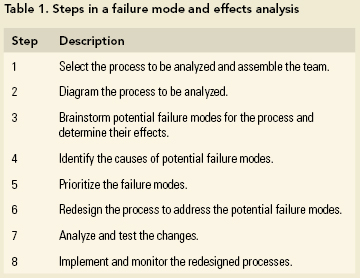
A typical FMEA includes eight steps (Table 1) and is conducted systematically (Joint Commission on Accreditation of Healthcare Organizations 2002).
FMEA requires a multidisciplinary team, including process experts and those with decision-making authority. FMEA is resource intensive and, as such, is most suitable for high-risk processes, that is, those in which failure is likely to jeopardize the safety of those served by the organization.
Topic Selection and Team Development
Selected members of the Annapolis Valley Health Patient Safety Committee met to determine the topics for analysis and to identify team members. Some aspect of the medication-use system was a natural choice for analysis, given that ISMP Canada, the organization that would be providing training and facilitation, has strong expertise in this area. A review of medication incident reports for Annapolis Valley Health showed that the incident type most frequently reported was related to the transcription process; the management of in-patient medication orders was therefore the first process identified for analysis. The group decided to base the analysis on the current processes for the Medical Unit at Valley Regional Hospital (VRH), one of six sites within the District Health Authority. It was hoped that solutions developed within this unit could later be shared across the district.
In the search for a second topic for analysis, it was noted that problems with "at or near capacity" status (also called "Code Purple") in the emergency department (ED) at VRH had been an ongoing concern and, in the opinion of the Patient Safety Committee representatives, presented a significant risk to patient safety across the district. This is a well-recognized problem across Canada (Noseworthy 2004; Physician Hospital Care Committee 2006; Rowe et al. 2006).
Once the topics had been selected, identification of the members of the analysis teams proceeded quickly. Individuals were chosen on the basis of their involvement in front-line care and their demonstrated understanding of departmental processes. Most of those who were invited to participate were enthusiastic and readily agreed to become part of the project.
In-patient Medication Process: Team Medication
Team Medication included a physician (general practitioner), registered nurse, licensed practical nurse and ward clerk from the medical unit, as well as the director of pharmacy. The team was led by the interim director of risk management and patient safety. Before the off-site facilitated session (led by an ISMP Canada staff member), the team reviewed background material on FMEA and mapped out the steps of the in-patient medication process at VRH (Figure 1).
[Figure 1]
"Nurse processes medication order," step 2 in the 14-step high-level process, was selected as the starting point for analysis through FMEA as it was deemed to be a key point where failures tended to occur and where existing systems were weak because of difficult-to-control manual processes. Within this step, team members identified seven substeps and 31 sub-substeps. The sub-substeps in the transcription step, along with the identified potential failure modes, are shown in Figure 2. During the off-site facilitated session, the team analyzed the first two sub-substeps in the transcription process, including identification of potential failure modes, the effects and causes of those failure modes, assessment of single-point weaknesses, calculation of criticality scores, development of potential solutions and re-scoring of criticality. The balance of the project was completed during more than 30 hours of meeting time over the subsequent seven months (for a total of 180 person-hours for the project).
[Figure 2]
"At or Near Capacity" Status in the Emergency Department: Team Code Purple
Team Code Purple included a physician (the VRH chief of staff), the ED nurse manager and an ED staff nurse, a clinical leader for the site and the director of quality and system performance. The team was led by the incoming director of risk management and patient safety. The team decided to first consider the issue of capacity assessment in the ED and how the organization responds to this form of crisis, which was step 1 of a nine-step process (Figure 3).
[Figure 3]
During the off-site facilitated session, the team completed the FMEA for all of the substeps related to capacity assessment in the ED, including the calculation of criticality scores and development of solutions. On return to the home institution, Team Code Purple found that there was some duplication and overlap among the nine steps; the team was therefore able to collapse the process into six substeps (Figure 4). The team completed the FMEA over the following seven months using approximately 150 person-hours.
[Figure 4]
Findings
Both Team Medication and Team Code Purple were surprised by the complexity and interrelatedness of the systems under analysis, which hospital staff used automatically and unquestioningly on a daily basis, and by the magnitude of the potential for harm within these complex processes.
Team Medication
Team Medication identified 78 potential failure modes within the various substeps for processing of medication orders. At one point, while considering the magnitude of the identified issues, one team member wondered aloud if anyone had actually designed the current system. A criticality score out of 100 was determined for each potential failure mode. The criticality scores ranged from 2 to 80, with a sum for all identified failure modes of 2,384 and an average of 31. Major themes discovered by Team Medication included communication, policy development, implementation of systems technology and general continuous quality improvement activities, as described below:
- Communication issues were found to be multidimensional. In particular, the FMEA highlighted concerns about communication between individuals as well as between departments.
- Development of and adherence to policies within the context of clinical activity was inconsistent. For example, the FMEA showed that allergy information was collected and documented in several places, but the information for a given patient was often contradictory.
- Investment in information systems technology was seen as key to solving many of the problems. For example, legibility of written orders can be problematic, and transcription of written orders by both nursing and pharmacy staff seems inappropriate in the context of a modern healthcare system.
- General continuous quality improvement activities, such as creating a double-check certification process for nursing staff, would assist in ensuring that double-checks are completed consistently.
Team Code Purple
Team Code Purple identified 31 potential failure modes with criticality scores ranging from 2 to 64 (sum 1,268; average 41). The highest-priority failure modes related to unpredictability of service demand, poor compliance with discharge criteria, inadequate documentation of patient care plans, lack of utilization and workload information systems and poorly understood and defined team roles for responding to a Code Purple. When the team recalculated criticality scores on the basis of full implementation of the recommended solutions, their sum dropped to 133 - a potential improvement of 90%!
Analysis of the failure modes and potential solutions identified by Team Code Purple revealed four themes: managing information, policy and procedure development, practice issues and communication.
- Managing information was a problem in several areas within the target hospital and across the provincial healthcare system. Specific concerns identified by the FMEA ranged from the lack of an electronic triage and workload measurement system in the local ED to the lack of a provincial bed-management system.
- The development of new policies and procedures is required at the board, executive, facility and unit levels. For example, policies are needed for determining district utilization of beds, creating clear trigger points for initiating certain processes and developing team, unit and individual expectations for responding to a Code Purple crisis.
- Practice-related issues identified by the FMEA included lack of documented care plans, problems with timeliness of physician rounds and response of all care providers to a Code Purple.
- Communication problems were found to affect various levels of the organization. For example, communication processes within the ED team, throughout the site and the district as well as communication of wait times to the public were complex, and varied depending on the time of day and day of the week.
Sharing of Information and Engaging the Organization
Senior leaders within Annapolis Valley Health were kept informed of the teams' progress in general terms throughout the course of the two projects. At the time of this writing, the two teams had completed their respective FMEAs but had not received administrative approval for full implementation of recommendations. The detailed findings will be presented at an upcoming meeting of key stakeholders. In the interim, improvements within the control of department leaders are being implemented.
The team leaders recognized the need to summarize the FMEA findings in a compact and meaningful way to assist the organization's leaders to understand both the findings and the recommendations. A summary sheet was developed to categorize and group related recommendations (Figure 5).
[Figure 5]
Lessons Learned
Team Process
A number of important lessons were learned regarding team dynamics:
- The commitment of team members is fundamental to success. The staff members who were invited to participate were genuinely interested in improving patient safety.
- Direct care staff must be involved in the process. Annapolis Valley Health was fortunate to have two physicians who were willing to participate in an activity that some would view as outside their scope of work.
- The team needs to be supported as it negotiates its own rules and learns the process through experimentation and experience.
- The individual value of each team member must be recognized. Everyone's perspective is different, and the understanding of the process under analysis varied among individuals according to their role within that process. Revelations about how processes worked within and between departments improved the understanding of individual roles within the system.
- Team leaders and facilitators play a crucial role in maximizing the efficiency of the team and ensuring that documentation and background information are completed and available when needed.
- Having a defined "scribe" who records discussion notes that are not part of flow charts and spreadsheets is helpful for dealing with questions that arise later in the analysis.
- Teams need to celebrate small successes and have fun.
Additional Learning
Teams undertaking large-scale FMEA projects such as the ones described here should get early administrative sign-off on the scope of the project and the associated resource requirements. Support by organizational leadership, as evidenced through the serious consideration of recommendations made by FMEA teams, is key to sustaining the efforts of individual staff for future FMEA projects. In retrospect, it would have been helpful to have followed a defined procedure for keeping decision-makers up to date on team activities.
Each team identified multiple opportunities for improvement; however, an unexpected positive benefit was that an enhanced understanding of the work of different team members resulted in a number of immediate quick fixes, some related to the processes under analysis and others for unrelated processes. For example, when nursing and pharmacy staff discussed medication process issues, they discovered that the delivery of narcotics could be improved by a simple change in timing. Some recommendations did not have an associated cost and could be implemented immediately by the charge person in the area. Planning for the implementation of each team's recommendations identified others within the organization who had to concur with recommendations and who could assist with implementation. The FMEA process helped the teams to consider additional solutions; for example, Team Code Purple asked the district's telecommunication and information services department to address the problem of urgently communicating information about ED overcrowding to family practitioners working in the community.
Use of Tools and Technology
The teams used technology as much as possible to minimize administrative activity. ISMP Canada provided electronic versions of spreadsheet tools. In addition, Visio software was used for electronic brainstorming of failure modes and for documenting related information. Some team members had the technical skills to use various types of software and to develop spreadsheets (e.g., the summary document shown in Figure 5), which was helpful. Use of colour for the complex summary documents improved readability and enhanced understanding. The summary document developed by the team also provided a visual representation of the amount of work completed.
Conclusions
To say that conducting an FMEA is time-consuming is an understatement; however, the value of this type of analysis lies in the fact that processes are deconstructed to a level of detail that allows full analysis of the potential opportunities for failure. This experience has convinced team members that attempting to shortcut the process through a less robust analysis would allow significant opportunities for harm to go undetected.
The findings of FMEA teams need to be widely shared within and outside individual organizations. This will help to sustain the momentum of the organization's quality improvement and risk management initiatives and will encourage action to implement recommendations. Furthermore, other facilities can learn not only from the specific process analysis and action plans but also from the personal experiences of other teams.
About the Author(s)
Tim Nickerson, BA(Hon), is Manager of Human Resources at Annapolis Valley Health (and was formerly director of Risk Management and Patient Safety), Kentville, Nova Scotia, and an MPA(M) student at Dalhousie University, Halifax, Nova Scotia.
Margie Jenkins, RN, BN, MN, is director of Risk Management and Patient Safety at Annapolis Valley Health.
Julie Greenall, RPh, BScPhm, MHSc, FISMPC, is project leader for Analysis and Consultation Projects at the Institute for Safe Medication Practices Canada, Toronto, Ontario. You can reach Ms. Greenall at jgreenall@ismp-canada.org.
Acknowledgment
The authors would like to acknowledge the tireless efforts of Team Medication: Anne Barry, MD; Elaine Lightfoot, LPN; Satch Currie, ward clerk; Dylana Arsenault, PharmD; and Joanne Marshall, RN; and Team Code Purple: Lynne Harrigan, MD; Lynn Fudge, RN; Kim Hutchison, RN; Kathie Swindell, RN; and Sue Hayes, Director of Quality. Thanks also to Ethel Gunn and Jacinta Archibald of the Guysborough Antigonish Strait Health Authority for proposing and coordinating the initial joint FMEA project and to Peggy Robinson for manuscript editing assistance.References
Canadian Council on Health Services Accreditation. 2007. Patient Safety Goals and ROPs. Ottawa: Author. Retrieved September 5, 2007. < http://www.cchsa.ca/default.aspx?page=139 >.
Institute for Safe Medication Practices Canada. 2006. Failure Mode and Effects Analysis Framework: A Tool for Proactively Identifying Risk in Health Care. Toronto, ON: Author.
Joint Commission on Accreditation of Healthcare Organizations. 2002. Failure Mode and Effects Analysis: Proactive Risk Reduction. Oakbrook Terrace, IL: Joint Commission Resources.
McDermott, R., R. Mikulak and M. Beauregard. 1996. The Basics of FMEA. Portland, OR: Productivity, Inc.
Noseworthy, S.B. 2004. "Emergency Department Overcrowding: Waiting for Disaster." Outlook Spring 27-1, p. 12-17.
Physician Hospital Care Committee, a tripartite committee of the Ontario Hospital Association, Ontario Ministry of Health, Ontario Medical Association. 2006. Improving Access to Emergency Care: Addressing Systems Issues. Toronto: Ontario Medical Association.
Rowe, B.H., K. Bond, M.B. Ospina, S. Blitz, M. Schull, G. Innes, M. Afilalo, M. Bullard, S.G. Campbell, G. Curry, B. Holroyd, P. Toon and D. Sinclair. 2006. Emergency Department Overcrowding in Canada: What Are the Issues and What Can Be Done? (Technology Overview No. 21). Ottawa: Canadian Agency for Drugs and Technologies in Health.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Note: Please enter a display name. Your email address will not be publically displayed