
Healthcare Quarterly
Integrated Health Systems and Integrated Knowledge: Creating Space for Putting Knowledge into Action
Abstract
The capacity to innovate and share knowledge is not well developed within health systems. In this paper we highlight essential structures, principles and processes for successful implementation of knowledge utilization strategies in complex health systems. We demonstrate essential links between systems that support knowledge utilization and governance, change management, information management and process improvement.
"The multiplicity of terms complicates working in this field … what is needed is not the specific term, but rather the shared understanding"
- Birdsell and Omelchuk 2006
Introduction
A number of articles of this special edition of Healthcare Quarterly highlight the complexity of integrated health care systems. While there is no, "one size fits all" approach to integration, common principles (Suter et al. 2009) and lessons can be learned across these examples. This compilation of practice examples illustrates a point that has been made repeatedly in recent years (Birdsell et. al. 2005; Birdsell and Olmechuk 2006; Scott and Gall 2006; Saskatchewan Health Research Foundation [SHRF] 2007): tremendous work is being undertaken throughout the health system to create environments that support the provision of high-quality care. It is rare, however, that promising practices are spread effectively throughout the system. What is also evident is that the capacity to innovate and share knowledge is not well developed within health systems, and few resources are dedicated to these important activities. When good ideas succeed, it is more often due to the creativity, determination and hard work of the people involved than to explicit strategies for supporting the development and spread of their innovations. Alberta Health Services, through embedding a specific knowledge function within its organizational structure, is clearly communicating that knowledge systems are fundamental to overall health system integration and improvement.
Just as the definition of integration continues to evolve, so too does our understanding of strategies to effectively use knowledge in health systems. Over the past 30 years, an extensive body of evidence has accumulated from a range of disciplines and practice settings to guide evidence-informed planning and practice and to promote knowledge utilization (Hazlett et al. 2008). The application of such evidence to inform clinical practice, policy development and decision-making in health systems remains, however, haphazard, inconsistent and unpredictable (Eccles et al. 2005). Despite this, there are lessons to be learned from a range of innovative practice experiments taking place across Canada.
| Since 2001, Rehabilitation Services within the former Calgary Health Region has offered a Time Grants Program, which recognizes that employees need dedicated, protected time for assessing research evidence and moving evidence into practice. In addition to time away from work to focus on a project, grant recipients are provided with mentoring, particularly at the beginning of a project, to help clarify project goals and methods, and again at the end, to help with data analysis, presentations or writing for publication. |
The program is funded by unused salary dollars to pay relief staff on the days that grantees are working on their projects. For Rehabilitation Services, costs amount to about half a full-time job per year. During the first five years of the program (2001–2006), 34 time grants were awarded to teams involving 57 employees. A little more than half the projects were completed, and a third are in progress. The remaining projects were discontinued due to staff changes. Two thirds of the completed projects were accepted for publication. |
Results of participant interviews indicate that more than eight in 10 participants (83%) reported positive changes in patient care. More than nine in 10 (92%) reported improvement in their ability to employ evidence-based practice. What is particularly interesting about this model, however, is that participants have also reported positive changes in their professional lives. These include more confidence in their skills and knowledge and a greater overall sense of professional competence (CHSRF 2008). |
While the "tools" described in this section are inextricably linked, some might say that they are in need of integration. The focus of this paper is on moving what we know about what works into action – from clinical guidelines to community care processes to policy development. We will draw from current evidence to illustrate a range of principles and strategies for creating knowledge-rich healthcare environments – for integrating knowledge use into practice. This overview will demonstrate essential links between systems that support knowledge utilization and other "tools" such as governance, change management, information management and process improvement.
Evidence and Knowledge: Moving toward a Shared Understanding
Practitioners and decision-makers in health systems increasingly recognize the need for strategies to make better use of evidence to fundamentally improve practice. This reflects an understanding of healthcare as a knowledge-intensive field (Birdsell and Omelchuk 2006; Lomas 2000). Across Canada, there are exemplar programs that focus on building capacity for evidence-informed decision-making (e.g., SEARCH Canada training programs, CHSRF-EXTRA [Canadian Health Services Research Foundation – Executive Training for Research Application] fellowships and regional training programs) (Conrad 2008) and integrating knowledge synthesis and application into ongoing operations (e.g., by creating embedded knowledge transfer, research and evaluation units and functions within the healthcare system). In spite of these initiatives, however, there is little practical guidance for programs on how to make better use of knowledge in complex health systems.
Our understanding of evidence and knowledge is informed by results from recent reviews (Birdsell and Omelchuk 2006; Grimshaw and Graham 2004; SHRF 2007; Scott and Gall 2006) which indicate that, generally, most people prefer the use of basic descriptive terms and encourage a move away from jargon. We conceptualize evidence as being derived from a variety of sources – not only research, but also clinical experience; patient, family and care-provider experience; and local context and environment (Bowen and Zwi 2005; Rycroft-Malone et al. 2004). This expanded notion of evidence to inform decision-making is critical. Knowledge is generated from practical use or application of evidence. It involves personal experience to interpret and apply the evidence and consists of facts, beliefs, perspectives, concepts, judgment and expectations (Seidel et al. 2009). Knowledge is gathered, assessed, adapted and applied over time to manage specific situations and challenges (Rycroft-Malone et al. 2004; Scott and Gall 2006; Seidel et al. 2009). Knowledge may be exchanged either explicitly (e.g., verbally or in written form) or tacitly (e.g., through action). In organizations, it often becomes embedded not only in documents or repositories but also in organizational routines, processes and practices (Knowledge Exchange Centre [KEC] 2005; Scott and Gall 2006). For evidence to be effectively used in practice, people need to process different sources of evidence (i.e., generate knowledge) at different times in the decision-making process, in ways that are meaningful to their context.
Currently, many terms are used to describe using evidence in practice. Knowledge transfer, knowledge translation, knowledge exchange and knowledge utilization are just a few of these terms. Each is defined somewhat differently and implies a particular approach to the application of evidence in practice (Scott and Gall 2006). Knowledge transfer refers specifically to making relevant information accessible and available to end users (KEC 2005). In this case, movement of information is either academically driven (push) or user driven (pull). Definitions of knowledge translation differ, but most emphasize a more active connection between the researchers and users of research findings than is implied by the term knowledge transfer (Canadian Institutes of Health Research 2006; Davis et al. 2003). Knowledge exchange (KE) refers to "collaborative problem-solving between researchers and decision-makers" (Canadian Health Services Research Foundation 2009) and multi-directional learning, whereas knowledge utilization refers to the application of evidence in practice settings. Increasingly, emphasis has shifted from bridging the diverse research and practitioner cultures to a focus on developing effective partnerships that integrate the specific skills and knowledge and of both researchers and practitioners along the entire decision-making continuum (Bowen et al. 2005).
Efforts to embed evidence-informed practice are challenged not only by a lack of understanding of what works well in complex health systems, but also by the many terms that are used. We echo the sentiments of Birdsell and Omelchuk when they stated: "The multiplicity of terms complicates working in this field … what is needed is not the specific term, but rather the shared understanding" (2006: 17–18). There will always be differences in preferred terminology across disciplines, and it is not productive to expend energy in these debates; the field will advance as we look across the wealth of evidence to define common structures, principles and processes for generating and using knowledge in health systems.
Creating "Space" for Knowledge Utilization
While there are few overarching models to guide this work, a great deal is known about what needs to be in place for effective knowledge utilization to occur in complex health systems, and a combination of systems-level and individual-level approaches is required. Findings from a number of studies in a range of contexts have highlighted both high-level and more detailed understanding of the characteristics of the social and physical "spaces" for embedding knowledge utilization in systems to support change. Knowledge must not be seen as a product to be inserted into existing planning and decision-making processes but must be used to inform the way planning and decision-making takes place (Bowen et al. 2009). System- and practice-level changes are influenced not only by individual-level readiness for change but also by:
- The characteristics of the context within which people work (i.e., organizational readiness for change, absorptive capacity and culture) (Greenhalgh et al, 2005; Scott and Gall 2006; Snowden and Boone 2007);
- The attributes of the proposed change (e.g., usefulness of the innovation);
- Organizational structures and processes that facilitate or constrain uptake of evidence; and
- The nature of interpersonal relationships (e.g., trusting relationships that support the introduction of new ideas) (Scott and Gall 2006).
Similarly, Rycroft-Malone et al. (2002) suggest that successful uptake of evidence in practice (successful implementation [SI]) is a function of the complex interplay between the nature of the evidence being used (E), the quality of the context (C), and the types of facilitation (F) needed to ensure a successful change process (i.e., SI = f[E,C,F]). To be effective and sustainable, strategies designed to support utilization of evidence and practice change must take this complexity into account. Success is contingent on organizational capacity to engage in and use evidence, emphasizing the need for collaboration and participatory processes, stewardship and supportive environments (Scott and Gall 2006).
At a more detailed level, the following points highlight essential structures, principles and processes for successful implementation of knowledge-utilization strategies (Estabrooks et al. 2008; Scott and Gall 2006; Seidel et al. 2009):
Supporting strong leaders and leadership approaches that reflect understanding of, and support for, knowledge integration and reflective practice as an essential part of providing excellent care:
- In this sense, leadership is equated not only with people in senior executive position but is also distributed with people throughout the organizational structure who are actively engaged in, and accountable for, knowledge generation and use.
- Leaders who facilitate knowledge work within organizations are those who model and actively demonstrate their commitment to reflection on practice.
- Supports for such work include explicit mechanisms for recognizing and rewarding such leadership in organizational recruitment and evaluation activities.
Creating environments in which people are encouraged and supported to challenge and change practice based on evidence that they trust:
- Systems-level supports are essential for enabling individual-level change. In creating systems that support knowledge use, there is a tendency to gravitate toward the quick fixes – changing structures, putting information on a website and ensuring people have access to electronic communication devices – but these tools may hinder or support change, depending on how well they function and how they are used. Sustained systems change requires people who see and feel the need for change and then act upon those feelings.
- Supporting change also requires finding mechanisms to give voice to people who are traditionally silent within the system (e.g., patients, staff who continue to work in hierarchical and/or punitive working environments).
- Celebrating learning and change is an explicit way of demonstrating the value placed on the work being done.
- Support also involves placing value on time in ways that permit reflection within practice (CHSRF 2008).
Creating the reflective space needed to integrate knowledge with practice:
- Time is set aside in regularly scheduled meetings to review evidence and evaluate progress. While not all staff will necessarily be actively engaged in research and evaluation, these activities can be integrated into operational activities.
- The strategy of promoting collaborative approaches builds capacity for evaluative thinking while at the same time developing a shared understanding of issues and potential solutions.
Investing in relationships:
- Collaborative and positive working relationships among clinicians, administrators, researchers, patients and families fundamentally enhance evidence generation and use.
- People who generate and use evidence to inform practice (e.g., in planning, policy development, research and evaluation processes) are involved early and genuinely in projects.
Comprehensive communication strategies that support interpersonal interaction, which may include but are not limited to:
- Communities of practice
- Deliberative processes
- Web-based technologies
- Video-teleconferencing
(Cautionary notes about the use of email are emerging from recent studies. These results suggest that email may actually be a disabler rather than an enabler of knowledge flow when it is seen as a substitute for face-to-face communication [Bowen et al. 2009; Hazlett et al. 2008]).
Matching the strategy to the context (contextualizing strategies):
- Strategies that work well in acute care settings may be ineffective in community contexts. Similarly, strategies that work in acute care in urban areas need to be assessed for applicability in rural and remote areas.
- Research evidence is rarely sufficient to support decisions made for health system policy and planning. It is essential that we begin to articulate explicit criteria for valuing a range of evidence sources, criteria that consider not only the quality of evidence but also its relevance for different contexts, at different times and for different kinds of decisions.
Embedding research and evaluation in practice settings and strengthening linkages with universities:
- Investing in internal capacity for evaluation, research and use of evidence;
- Establishing dedicated positions or, in larger organizations, creation of specific units providing "real time" synthesis, evaluation, and research services in response to priority issues identified by the organization;
- Implementing mechanisms for sharing research findings;
- Undertaking collaborative research on topics relevant to practitioners and decision-makers; and
- Developing explicit linkage between health and research systems.
These connections are described as fundamental to strengthening health systems. In part, this is accomplished by strengthening applied research to improve population health outcomes and by focusing on systems-level initiatives (Seidel et al. 2009; World Health Organization 2004).
Making decision-support tools and resources available (e.g., practice guidelines, databases, information systems, communications technology, library services):
- The use of technology must never be considered the solution to the knowledge utilization puzzle. Decision-support tools and resources are a valuable adjunct to this work but must always be combined with strategies that support interpersonal interaction, dialogue and collaborative processes (Johnson et al. 2007).
Implementing strategies to ensure the sustainability of initiatives when warranted:
- Critical review of current practice to ensure that what is being done continues to meet the needs it was designed for. When warranted, the potential for sustaining programs and practices is supported if the knowledge gained through their application is synthesized and shared in other contexts.
Embedding knowledge utilization in health systems requires explicit strategies for linking people with evidence in ways that reflect the structures, principles and processes illustrated above. There are differing approaches to knowledge translation/transfer/exchange; unfortunately, these have remained limited to focus on the use of research evidence typically generated by university-based researchers (Birdsell et al. 2005; Graham and Logan 2004). Different models are required when we begin to think of strategies for knowledge utilization that are embedded in health systems and where the research is responsive to issues of concern to the healthcare system. In these contexts, ongoing investment in capacity, relationships and reflection becomes paramount.
The model illustrated in Figure 1 was developed based on a review of practice and research evidence. It provided the foundation for the development of the Knowledge into Action department within the Calgary Health Region in 2006. Using evidence in decision-making for health services planning, policy development, management, delivery and use (that is, by patients and families) involves an iterative process of:
- Clearly articulating the problems we are dealing with in order to ask good questions;
- Acquiring and assessing the various sources of evidence that are relevant to the questions asked and to the context;
- Adapting evidence as needed to apply it in context; and
- Evaluating the strategies that are developed based on the best available evidence.
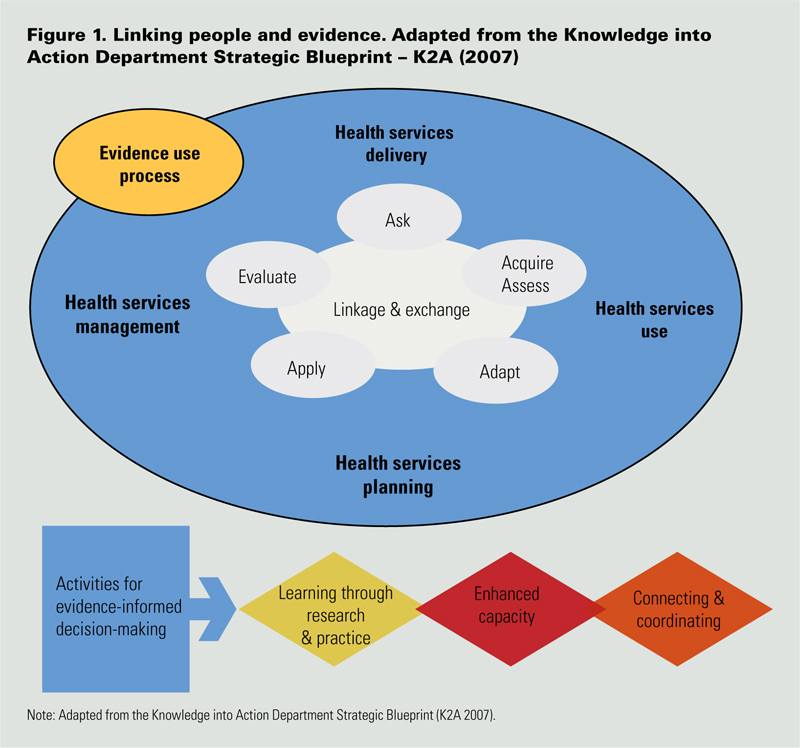
Within this model, activities required to support evidence-informed decision-making include:
- Enhancing capacity for creating and using evidence;
- Developing mechanisms for learning through research and practice; and
- Connecting and coordinating people and activities in order to build on what is learned.
So What Does This Mean in Practical Terms?
Given that we know all of this, why do health systems continue to struggle with moving knowledge into practice? Certainly, the complexity of our current system, the many competing demands on staff and managers and the need for strategies to be appropriate to the specific context are all contributing factors. If, however, there is commitment to fundamentally changing health systems to better meet the needs of the population within resource constraints, there is no question that the ways in which we organize ourselves and work with one another have to change. The creation of social (i.e., organizational structures, principles and processes) and physical spaces that promote the generation and use of knowledge through collaborative processes is fundamental to systems change, so that we are able to build on what is known about what works and what does not work in different contexts. We must move beyond a focus on individual professional development and focus instead on strategies designed to engage staff and patients in process and system improvements. Such strategies will contribute not only to staff recruitment and retention but ultimately to improvements in patient and staff experience, safety and quality. The structures, principles and processes highlighted above are congruent with those identified as key elements of integration, for example:
- An organizational culture with strong leadership and shared vision;
- Supportive social and physical environments, including governance models and appropriate use of tools such as practice guidelines, information technology and communication mechanisms;
- Active participation of key stakeholders in sharing what they know to inform decision-making, implementation and evaluation; and
- Coordination of efforts within and across different contexts (Suter et al. 2007).
Our discussion of knowledge utilization in healthcare adds to the list of key elements critical for evidence-informed decision-making:
- Developing capacity for generating and making better use of contextually relevant evidence;
- Investing in time and relationships that support reflection on practice;
- Developing embedded research and evaluation infrastructure;
- Tailoring the strategies used to the contexts in which decisions are being made;
- Celebrating learning and success;
- Explicitly reviewing relevant evidence to determine when and when not to sustain current practice;
- Dedicating resources (e.g., time, staff) to knowledge-utilization activities;
- Focusing on developing evidence-informed change processes; and
- Collaborative implementation and evaluation processes.
Change of this extent requires a level of readiness for fundamental systems transformation. Change is no longer an option; it is a necessity. Moving forward with new ways of working and relating to others involves risks. There is no clear research evidence to support all that we do, but there is an enormous body of experiential evidence that we can draw upon locally and around the world. We must build an evidence base through embedded research and evaluation processes and use this to inform our next steps. Finally, we must also ensure that people who work in the system have the capacity to access the evidence they need to make decisions – the right information, in the right place, at the right time.
Such change will not be straightforward and will not always go as we had planned, but it is essential to begin to take steps in this direction if we are to achieve the goals of designing a patient- and family-centred health system that is accessible and sustainable for all Albertans, while ensuring quality supports and services through the application of best practices (Alberta Health Services 2008; Seidel et al. 2009).
About the Author(s)
Cathie Scott, PhD, is currently employed within Alberta Health Services - Calgary, leading research, evaluation and knowledge utilization initiatives. She is also a Faculty member with SEARCH Canada (www.searchca.net), and holds adjunct appointments with the Departments of Community Health Sciences and Sociology, University of Calgary.
Judy Seidel, PhD, is an epidemiologist and health services researcher in Alberta Health Services - Calgary. Her work involves leading embedded research and decision support initiatives in the areas of health system access and quality.
Sarah Bowen, PhD, holds a position as Associate Professor, School of Public Health, University of Alberta, and is currently Academic Co-Director, SEARCH Canada. As founding Director of Research and Evaluation within the Winnipeg Regional Health Authority, she led a unit with the purpose of promoting and facilitating evidence-informed planning and decision-making.
Nadine Ball, MSc, currently holds a position in applied health research and knowledge exchange within Alberta Health Services - Calgary. She is also a member of the SEARCH Canada Faculty - providing research and evaluation support for health professionals to facilitate use of evidence in practice and policy.
References
Alberta Health Services. About Us. Retrieved December 22, 2008. <http://www.albertahealthservices.ca/about/index.html>.
Alberta Heritage Foundation for Medical Research (2000). "Using Research to Improve Health: Five Years of Activity at AHFMR (1995-2000)." Foundation report, Department of Applied Health Research Programs (AHRP). Edmonton, AB: Alberta Heritage Foundation for Medical Research.
Birdsell, J. and K. Omelchuk. 2006. Using Health Research in Western Canada: A Scan and Assessment of Capacity. Edmonton, AB: Alberta Heritage Foundation for Medical Research.
Birdsell, J., R. Thornley, R Landry, C. Estabrooks and M. Mayan. 2005. The Utilization of Health Research Results in Alberta. Edmonton, AB: Alberta Heritage Foundation for Medical Research.
Bowen, S., T. Erickson and P. Martens., The Need to Know Team. 2009. "More Than "Using Research": The Real Challenges in Promoting Evidence-Informed Decision-Making." Healthcare Policy 4(3): 87-102.
Bowen, S. and P.J. Martens., The Need to Know Team. 2005. "Demystifying Knowledge Translation. Learning from the Community." Journal of Health Research and Policy 10(4): 203-11.
Bowen, S. and A.B. Zwi. 2005. "Pathways to 'Evidence-Informed' Policy and Practice: A Framework for Action." PLoS Medicine 2(7): e166.
Canadian Health Services Research Foundation (CHSRF). November, 2008. "Buying Time and Getting a Bonus: How a Regional Health Organization Is Tackling a Barrier to Building Research Use Capacity and Discovering Additional Benefits." Promising Practices in Research Use. Retrieved December 22, 2008. <http://www.chsrf.ca/promising/html/pp16_e.php>.
Canadian Health Services Research Foundation (CHSRF). 2009. Glossary of Knowledge Exchange Terms (on-line). Canadian Health Services Research Foundation website. Retrieved September 1, 2009 <http://www.chsrf.ca/keys/glossary_e.php>.
Canadian Institutes of Health Research (CIHR). (1) Moving Population and Public Health Knowledge into Action: A Casebook of Knowledge Translation Stories. (2) Evidence in Action, Acting on Evidence: A Casebook of Health Services and Policy Research Knowledge Translation Stories. Ottawa, ON: CIHR-IHSPR.
Conrad, P. 2008. "To Boldly Go: A Partnership Enterprise to Produce Applied Health and Nursing Services Researchers in Canada." Healthcare Policy 3: 13-29.
Davies, D., M. Evans, A. Jadad, L. Perrier, D. Rath, G. Sibbald, S. Straus, S. Rappolt, M. Wowk, M. Zwarenstein. 2003. "The case for knowledge translation: shortening the journey from evidence to effect." British Medical Journal 327(7405): 33-5.
Eccles, M., J. Grimshaw, A. Walker, M. Johnston and N. Pitts. 2005. "Changing the Behaviour of Healthcare Professionals: the Use of Theory in Promoting the Uptake of Research Findings." Journal of Clinical Epidemiology 58: 107-12.
Estabrooks, C.A., P. Norton, J.M. Birdsell, M.S. Newton, A.J. Adewale and R. Thornley. 2008. "Knowledge Translation and Research Careers: Mode I and Mode II Activity Among Health Researchers." Research Policy 37: 1066-78.
Graham, K. and J. Logan. 2004. "Using the Ottawa Model of Research Use to Implement a Skin Care Program." Journal of Nursing Care Quality 19: 18-24.
Greenhalgh, T., G. Robert, P. Bate, F. MacFarlane and O. Kyriakidou. 2005. Diffusion of Innovations in Health Service Organizations: a Systematic Review of the Literature. Oxford: Blackwell Publishing.
Grimshaw, J. and I. Graham. 2004. Environmental Scan of Knowledge Translation Activities of Canadian Health Researchers 2003-2004. Clinical Epidemiology Program, Ottawa Health Research Institute. Funded by the Canadian Institutes of Health Research (CIHR).
Hazlett, S.A., R. McAdam and V. Beggs. 2008. "An Exploratory Study of Knowledge Flows: a Case Study of Public Sector Procurement." Total Quality Management 19(1-2): 57-66.
Johnson K., S. Bowen, L. Zhang, S. Kreindler. 2007. Evaluation of the Manitoba Demonstration Project in Physician Demand-Side Control for Diagnostic Imaging. Winnipeg. WRHA. September 2007.
K2A 2007. Knowledge Into Action Strategic Blueprint. Unpublished policy document. Calgary, AB: Knowledge Into Action Department, Calgary Health Region.
Knowledge Exchange Centre. 2005. Knowledge Exchange Glossary. Provincial Centre of Excellence for Child and Youth Mental Health at the Children's Hospital of Eastern Ontario (CHEO). Retrieved October 14, 2005. <http://www.onthepoint.ca/resources/archives.htm.>
Lomas, J. 2006. "Commentary: Whose Views Count in Evidence Synthesis? And When Do They Count?" Healthcare Policy 1(2): 55-7.
Lomas, J. 2000. "Using 'Linkage and Exchange' to Move Research into Policy at a Canadian Foundation." Health Affairs 19(3): 236-40.
Rycroft-Malone, J., A. Kitsen, G. Harvey, B. McCormack, A. Titchen and C Estabrooks. 2002. "Ingredients for Change: Revisiting a Conceptual Framework." Quality & Safety in HealthCare 11: 174-80.
Rycroft-Malone, J., K. Seers, A. Titchen, G. Harvey, A. Kitsen and B. McCormack. 2004. "What Counts as Evidence in Evidenced-Based Practice?" Nursing and Healthcare Management and Policy 47(1): 81-90.
Plsek, P.E. and T. Greenhalgh. 2001. "Complexity science: the challenge of complexity in health care." British Medical Journal 323, 625-628.
Saskatchewan Health Research Foundation. 2007. Health Research in Action: A Framework for Building Capacity to Share and Use Health Research. Saskatoon, SK: Author.
Scott, C. and N. Gall. August, 2006. Knowledge Use in the Calgary Health Region: a Scan of Initiatives That Support Use of Evidence in Practice. Final Report. Calgary, AB: Calgary Health Region.
Snowden, D.F. and M.E. Boone. 2007. "A Leader's Framework for Decision Making." Harvard Business Review (November): 69-76.
Seidel, J., C. Scott, V. Austen-Wiebe, S. Dean, C. DeCoster and D. McNeil. 2009. Embedded Research: A Knowledge Exchange Strategy for Health System Improvement. A report prepared for Alberta Health Services - Calgary Health Region.
Suter, E., N.D. Oelke, C.E. Adair, C. Waddell, G.D. Armitage and L.A. Buebner. 2007. Health Systems Integration: Definitions, Processes & Impact - Research Synthesis. Calgary, AB: Calgary Health Region.
Suter, E, N.D. Oelke, C. E. Adair and G.D. Armitage. 2009. "Ten Key Principles for Successful Health Systems Integration." Healthcare Quarterly 13(Special Issue October 2008): 16-23.
Westley, F., B. Zimmerman and M.Q. Patton. 2006. Getting to Maybe: How the World Is Changed. Toronto, ON: Random House Canada.
World Health Organization. 2004. World Report on Knowledge for Better Health: Strengthening Health Systems. Geneva: Author.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Note: Please enter a display name. Your email address will not be publically displayed