
Healthcare Quarterly
Designing Effective Governance for Quality and Safety in Canadian Healthcare
G. Ross Baker, Jean-Louis Denis, Marie-Pascale Pomey and Anu MacIntosh-Murray
Governing boards of healthcare organizations in Canada are accountable for the performance of their organization and provide oversight on their decisions. Traditionally, many healthcare boards have focused on finances and community relations and have deferred responsibility for quality of care to the medical or professional staff. This deferral reflects not only recognition of the expertise of clinical leaders on these issues but also the historical separation of responsibilities between the administration and the medical staff, the former being responsible for financial and operational issues, and the latter for quality of care.
Governing boards of healthcare organizations in Canada are accountable for the performance of their organization and provide oversight on their decisions. Traditionally, many healthcare boards have focused on finances and community relations and have deferred responsibility for quality of care to the medical or professional staff. This deferral reflects not only recognition of the expertise of clinical leaders on these issues but also the historical separation of responsibilities between the administration and the medical staff, the former being responsible for financial and operational issues, and the latter for quality of care.
A number of recent developments have altered this situation. First is the growing evidence of problems in the general level of quality and safety of care across healthcare organizations (e.g., Baker et al. 2004; Bruce et al. 2006; Canadian Institute for Healthcare Information 2008; Health Quality Council 2007). This information clearly demonstrates gaps between current performance and achievable results. Related to this is the growing movement to publicly release performance data and use them in creating explicit accountabilities on quality and safety. As a result of these pressures, there is growing interest in understanding the strategies, tactics and tools through which boards can establish quality and safety goals and stimulate improvements in healthcare organizations.
Can Healthcare Boards Influence Performance?
Efforts to engage boards in improving care are based on the rationale that an "activated board, in partnership with executive leadership, can provide the will and set system-level expectations and accountability for high performance and the elimination of harm … to dramatically and continuously improve the quality of care" (Conway 2008: 215). Yet the empirical evidence supporting this argument is slim. Two US studies have found correlations between board and senior leader activities and higher quality of care. The first study by Vaughn and colleagues (2006) used data from a survey of hospital leadership in eight states and risk-adjusted measures of morbidity, morality and complications. The authors found that better-quality outcomes were associated with board and medical staff who spend more time in setting quality strategy, where boards receive a formal performance measurement report and where compensation of senior executives was based in part on quality performance.
A second recent study by Jiang and colleagues (2009) used data derived from a survey of board practices linked to administrative data on care processes and outcomes for heart attack, heart failure and pneumonia. The authors in this study found a statistically significant correlation between process of care and mortality measures and a number of self-reported measures of board activities. These measures included the presence of a board quality committee, the setting of strategic goals for quality improvement by the board, the use of indicators of clinical quality and patient safety by the board, the presence of specific items on the board agenda devoted to quality, the spending of more than 20% of board meeting time on quality issues and the performance evaluation of chief executive officers (CEOs) including measures for clinical improvement and patient safety.
In addition to the studies by Vaughn and Jiang and their colleagues, there have been several case studies reporting hospital and health system experiences in board engagement (e.g., Rose et al. 2006; Slessor et al. 2008) and less formal web reports (e.g., IHI.org) that note improvements in clinical process and outcome measures following greater board involvement. The Institute for Healthcare Improvement (IHI) has carried out a high-profile effort with its Boards on Board campaign (IHI 2008), which focuses on stimulating board involvement and leadership in improving quality of care. While the IHI focus has been primarily on US hospitals and health systems, its work has captured the attention of leaders in Canada as well.
Clearly, additional research is needed on how to influence quality and patient safety and the extent to which this can be done by boards. The existing literature and case reports are almost entirely based on US experience. More research on how boards function in Canadian healthcare organizations and their impact on quality of care and patient safety is needed to assess their effectiveness in these areas. This study focused on identifying the extent to which boards of Canadian hospitals and healthcare regions set goals, monitor performance and influence improvements in quality of care and patient safety.
Methods
Semi-structured interviews were held between February and August 2008 with 15 experts in Canada and the United States on board performance and strategies and tools for helping boards to set goals, monitor performance and improve quality and safety. Experts were selected based on the results of a literature review and nominations from key informants. Based on these interviews, we selected and developed case studies of four healthcare boards, three in Canada and one in the United States, that were identified as using leading practices in the governance of quality and patient safety. These organizations – the Ottawa Hospital, Saskatoon Health Region, Vancouver Island Health Authority and Virginia Mason Medical Center (in Seattle, Washington) – were selected to include examples from regional authorities and hospitals. In June, July and November 2008, between two and four team members paid one visit to each of the four sites. In advance of each visit, the researchers reviewed a range of background documents provided by system informants, including strategic plans, annual reports, terms of reference, improvement reports and committee minutes. Site visits included meetings and interviews with board chairs and members, CEOs and their executive teams, senior clinical leaders and support staff.
For each case study, the unit of analysis was the board and its governance practices in regard to quality and safety, including its interface with the CEO, executive team and clinical leadership as well as its relationships with key external agencies, including government, accreditors and other bodies, such as IHI. An average of 10 interviews per case was conducted, supplemented by documentary analysis (Kvale 1996; Lofland and Lofland 1995). The analysis focused on key aspects of governance practices and on the resources, competencies and instruments that support the implementation of such practices. The analysis was based on interpretive methods (Coffey and Atkinson 1996) to identify key themes and concepts and the relationships between them. The case studies were crafted based on a thematic analysis of extensive notes recorded during the interviews, integrating details from the strategic and operational documents from each site (Miles and Huberman 1994; Yin 2003). Key interview participants at each of the four sites reviewed the draft reports to ensure factual accuracy.
Results
Interviews with Canadian leaders, including CEOs of hospitals, health region board chairs and executives of other healthcare organizations, and with US experts suggest that efforts to improve the governance of quality and patient safety in Canada are still in early stages in many organizations. As one of our interviewees noted: "Each board has dealt with [quality and safety] from a different perspective. They are not using consistent indicators, they are not using a consistent approach, and they don't really understand what their role is, what their fiduciary responsibility is with respect to quality … In some cases they are a little mixed up because they think the MAC [Medical Advisory Committee] is responsible for quality and they don't understand what the governors' role in quality is. And if they think they have a role, they don't know how to carry it out."
For much of the past decade, most Canadian boards have been concerned with financial and access questions, which have been seen as the most critical issues for Canadian healthcare organizations. Another interviewee remarked, "We have no one in the public sector putting pressure on healthcare [organizations]; no province is doing so. We are doing it through CCHSA – [those] standards are going to help. [CCHSA is the Canadian Council on Health Services Accreditation, now Accreditation Canada.] The Saskatchewan Health Department issued a governance manual, but they leave a lot of execution to the boards; they didn't mandate it."
Adopting a greater responsibility for quality and safety performance is challenging for many boards. Few board members have much experience or knowledge of quality activities, in healthcare or other industries, and not many boards target the recruitment of members with skills in the quality arena. Moreover, there are few avenues for education on these issues. A former Canadian hospital CEO could not identify any education programs offered by Canadian organizations in this area. And a former board quality committee chair lamented that there is no forum in Canada for board members to learn about quality and safety so that they can discharge their oversight responsibilities. Several health association CEOs noted that there is a growing concern with quality and safety issues in their member organizations, but they also noted the limited responses to prepare board members to address these issues.
When asked to nominate healthcare regions or organizations whose boards represented leading performance, many of our interviewees found it difficult to nominate organizations, or qualified their nominations, saying that "they were making progress, but were still in early stages." Interviewees did not believe that many boards in Canada are spending 25% or more of their time on quality and safety oversight, a figure cited by US experts (Conway 2008; Vaughn et al. 2006).
Several factors constrain attempts to change the current membership skill mix and board activities. In several provinces, board members are appointed by government to regional boards, restricting the ability of regions to recruit members with skills in quality and safety. The Carver model of governance (Carver 2006), which is popular in many organizations, encourages boards to focus on issues of organizational purpose and policy and to leave decisions on how organizations achieve these policies to management. This model, sometimes termed "policy governance," makes it awkward for boards to discuss the details of patient safety events or consider the means by which healthcare organizations are attempting to improve safety. Interviewees in several provinces noted that the board's reluctance to "get into management issues" was a frequently cited reason for not discussing patient safety matters. One board member explained that the provincial government had not expected the regional board to create a quality committee. "This was the time that they were talking about policy governance, a Carver [model]," explained one board member, "and they thought that we would be drilling down too much and going into operations by getting into quality."
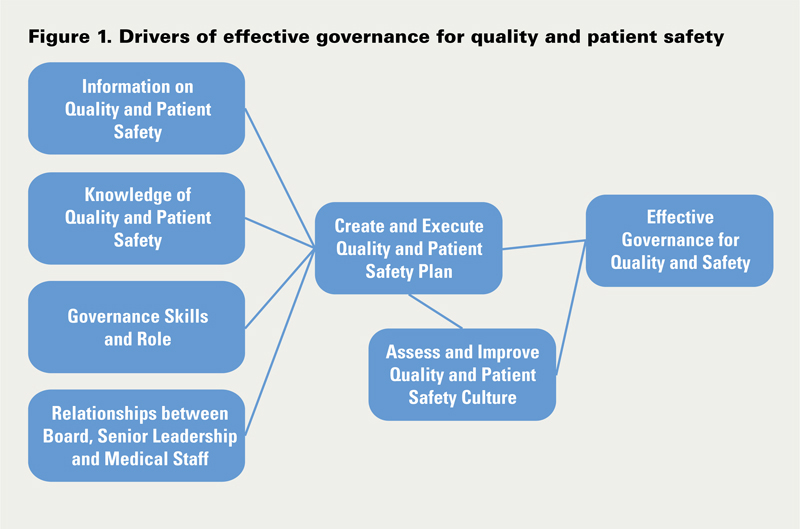
Board members, senior healthcare leaders and other key informants identified a number of critical drivers for more effective governance of quality and patient safety, including better information on quality and patient safety; improved trustee education and skills; changes to governance roles and processes; improved efforts to create and monitor a quality and safety plan; and new relationships between board members, senior leadership and medical staff leadership.
Information on Quality and Patient Safety
Many healthcare organizations face challenges in creating useful performance measures that can be easily interpreted by lay members of a healthcare board. Such measures need to be timely assessments of current performance in targeted areas. Hundert and Topp stress that "the board as a whole should routinely monitor results for a small number of critical corporate indicators" (2003: 61) and ensure that management and the MAC are monitoring quality results in a more detailed fashion. One of our interviewees also noted that the frequent variability of measures used in different programs, the lack of longitudinal data necessary to assess whether performance is improving and the lack of comparisons to other organizations make improvement difficult. He also noted that many board quality committees are unsystematic and unquestioning about the information they receive on quality of care.
In regional authorities, the search for a few good measures to inform the board is even more difficult since these boards need to understand performance for a wider variety of services and types of care. As one regional CEO described it, "Part of our challenge in a regional system is it's not just acute care. And so you know you want to keep this [report as a] small two-pager, and yet you've got services in such a broad range of programs that to get some that relate to the other part of the business is a bit of a challenge too – you know mental health and addictions and public health and some of these – so that is still a work in progress."
Some organizations have created voluminous reports with dozens of measures across many programs. The Ottawa Hospital is devoting considerable effort and resources to develop a data warehouse, but creating appropriate and useful measures for the board continues to be an issue. Until recently, their board received 75 or more measures. The director of the Centre for Patient Safety noted, "There is still not a very sophisticated method of capturing data across the organization in a way that the board can understand it and it's not minutia." New data formats, including a balanced scorecard, are being discussed, but some board members are concerned that this format oversimplifies the complex nature of the hospital's work.
The Saskatoon Health Region uses two dashboards, one developed by the Ministry of Health that includes financial and access measures and one produced internally that focuses more on quality and safety. Some measures are dictated externally and do not provide sufficient information to assess the impact of local improvement projects, while some internal measures cannot be compared with other organizations' performance. The board is working to develop a more effective report.
Virginia Mason Medical Center also sees quality and safety measures as a critical tool for the board and agrees that finding the right set of measures is a challenge. The Virginia Mason approach incorporates several aspects that help to ensure that the performance measures presented to the board are relevant and informative. The roughly 20 measures are tightly linked to key strategies. Moreover, while the Quality Oversight Committee (QOC) examines the data in detail, the measures are collapsed to three or four measures of quality and patient safety when the performance is reported to the board as a whole. For example, the measure of patient safety includes data on a range of different initiatives and outcomes, including performance on clinical care "bundles" (e.g., the bundle of care process measures for acute myocardial infarction), surgical site infections and adverse drug events. This strategy allows the full board to assess the overall patient safety performance, while the QOC drills down on specific measures and assesses whether the work plan for each goal is on track.
Virginia Mason struggled with the issue of reconciling the demands for external accountability on specified measures (which may vary between different regulatory bodies) with the information needed to assess performance and guide strategic and operational decisions. The external measures are required for accreditation and other oversight activities, but they may not reflect the critical strategic goals for the organization. Gary Kaplan, Virginia Mason's CEO, described the dilemma and the organization's response: "Five years ago we had what we called the 54 Must Dos, 54 metrics that were in the public domain from some bodies we respected – Leapfrog, National Quality Forum, IHI [and the Joint Commission]. But you realize that if you are chasing 54 priorities, you are not really chasing any of them adequately. So we've gotten much better at honing in and trying to triangulate … and putting our own work to it, so we've got clear organizational quality and safety goals."
This challenge of reconciling the information needed for external accountability and that needed to inform local improvement is present in both US and Canadian organizations. Another issue facing Canadian organizations is the extent to which they will make information about their performance available publicly. Most boards have used quality and safety information for internal purposes and have reported only what is required, principally to government. Expectations in this area are changing rapidly. For example, Ontario hospitals receiving additional funding for surgical cases for specified conditions are now required to report on the incidences of Clostridium difficile, methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci infections and on measures of ventilator-associated pneumonias, central line infections and compliance with measures to reduce surgical site infections. Some hospitals had made this information publicly available prior to the ministry requirements, but others are approaching this issue more cautiously. One of our interviewees noted, "Our annual report is not really an accountability report to the community about how we are performing on quality and safety. It's a marketing document."
The push to develop external measures needs to be balanced against the types of measure that are useful for boards and senior leadership. James Reinertsen (2007), a former hospital CEO, believes that the most useful measures for boards are not the risk-adjusted and highly analyzed comparisons developed by third parties but raw local hospital data on key counts such as deaths, surgical complications, infections, patient complaints and patient satisfaction. Rather than asking, "How do we compare to others?" Reinertsen (2007) urges board members to set ambitious goals and to use more timely hospital data to answer the questions, "Is our care getting better?" and, "If not, is the strategy wrong, or is it not being executed effectively?"
Knowledge of Quality and Patient Safety
What skills and knowledge does a board need in order to fulfill its fiduciary responsibilities on quality of care and patient safety? This issue seems to perplex many boards. Few boards have many members who have extensive background in healthcare quality or skills in industrial quality improvement, Lean production and similar techniques. There is a growing call for more education on this topic for board members, and many board members are participating in educational sessions designed for the staff of healthcare organizations.
There is no consensus on the extent to which all board members should be capable of assessing quality and patient safety. Some believe that orientation and continuing education in this area are essential for all members. Others emphasize the need for board members to rely upon the skills that they have in measuring performance and assessing the outcomes that they have developed in other domains. The issue is to ensure that boards can rely on sufficient expertise in this domain.
Another issue is whether boards should broaden their recruitment of members who have quality and patient safety knowledge and skills. A number of boards are now targeting members of their community who have quality skills in other industries. One of the key members of the Virginia Mason Medical Centre board is a vice-president of Boeing and an expert in Lean production techniques. The Governance Committee at Virginia Mason has developed a skills matrix to guide the recruitment of new members. The board chair identified how this is used: "So, our overall selection grid looks at the expertise that is needed, looks at what we have on the board presently, looks at when board members are going to be retiring and matches that all up so that when the Governance Committee goes out and is charged with looking and selecting the board members, they are looking for somebody specifically with a safety and quality background, for example."
Similarly, another one of our interviewees discussed the approach his region's board is taking to improve the board's assessment and guidance on quality and safety. He noted that the board began by developing a governance committee and creating a skills-based assessment of the board. This analysis helps to establish a foundation for developing a board that is capable of ensuring that patients receive high-quality and safe care. In our case studies, the approach to improving board skills on quality and safety seems to rest on the effectiveness of governance committees, board self-evaluations and the extent to which boards have identified their needs for orientation and education.
Creating a Quality and Patient Safety Plan
Timely and relevant information about current performance and knowledge on quality of care and patient safety are important ingredients in creating strategic goals for the organization. The Ottawa Hospital Corporate Quality Plan provides a good example of a quality plan that includes specific objectives, defined measures with clear targets and assigned responsibility for execution for each element of the plan. For 2007–2008, the objectives included improving patient flow and access for both emergent and elective patients, improving transitions of care through clinical pathway use, safer medication practices and improving patient safety through improved adverse event reporting, root-cause analysis at system and unit levels and mortality and morbidity rounds.
Since most board members have limited knowledge about the quality improvement initiatives in the organization, the leadership in developing quality plans often rests with management. However, in the case study organizations, the role of the board or board quality committee was not passive. In Saskatoon Health Region, the board participates in the development of the quality plan. One member of the senior management team noted that "the quality plan falls right out of our strategic plan; it drives some of the very specific work and goals." At Virginia Mason Medical Center, the board's QOC assumes the responsibility for developing the quality plan. The board chair described the process this way: "It was led by the QOC, not just by management, and the QOC worked on the goals and objectives. It went back to the larger management teams for review and came back to the QOC. We have gotten to a point where that sort of a quality and safety strategy is being led by the QOC, versus management recommending and the QOC simply approving. We had several late nights wherein the total focus of the QOC meeting was, what revisions do we believe are necessary, or what enhancements do we believe will be helpful, to our quality strategy going forward?"
In all our case studies, board and senior managers strove to create a quality plan that was an integral part of the broader strategic agenda. Such plans need to be more than just reactions to targets set elsewhere. They need to be anchored in core metrics of organizational performance. And they need to be aligned with other key aspects of the strategic plan. At Vancouver Island Health Authority, the board works with staff to set quality and patient safety priorities, taking into account the Ministry of Health's directions in their annual "letter of expectations." Staff provide reports and monitor trends, but board members also identify issues and initiate new directions.
In addition to identifying specific areas for clinical improvement, boards need to ensure that their organizations have created an environment that is conducive to improving the quality and safety of care. Boards can encourage and endorse disclosure policies, the development of a just culture and effective patient safety reporting and learning strategies that help to create an atmosphere of openness, trust and improvement. Boards need to encourage the development of a patient safety culture that provides a fertile environment for specific quality and safety initiatives.
Governance Skills and Role
Highly effective governance processes are challenging to develop and maintain in any area. But the challenge in quality and safety is increased by the difficulty in maintaining a focus on the board's responsibilities for providing oversight and strategic direction, and avoiding the temptations of directing management and reviewing operations. How can boards do this when discussions of patient safety inevitably lead to a review of failures in clinical processes or lapses in information transfers?
Our case studies revealed several ways in which effective governance processes allow boards to negotiate these potential conflicts. At the Ottawa Hospital, the board spends time with management in "generative governance," deliberating on organizational challenges such as the need to improve patient flow and reduce the numbers of alternative-level-of-care patients (who need to be transferred to other facilities but, for various reasons, cannot be). Such discussions allow board members to probe the nature of specific operational issues and to build a better understanding of hospital systems (Chait et al. 2005; Taylor et al. 1996). Such discussions require trust on both sides. As on CEO noted, "If you're a seasoned CEO, I can understand that you might be hesitant to have the board so involved. If you are a seasoned board member, you might be hesitant to get too involved in operational business. So, it's a risk on both sides that can turn into a disaster."
The Ottawa Hospital board reduces these risks by being clear about when it is engaging in such discussions, by limiting these to specific and important issues that require such clarification and by using the expertise of one board member who is experienced in these methods and helps to guide the discussions.
The QOC of the board at Virginia Mason Medical Center has also developed a strategy that challenges the traditional division between policy and management responsibilities. Following a visit to Japan, where they were impressed with the delegation of authority to all production line workers to "stop the line" to correct quality problems, Virginia Mason decided to implement a patient safety alert (PSA) system by which any staff member can flag a safety and quality issue. These issues led to immediate situation assessments and root-cause analyses, with the goal of making corrections in real time (usually finished within three to 18 hours). The PSAs are categorized as yellow, orange or red based on their severity or potential for harm (Furman and Caplan 2007). Initially, the QOC only reviewed the numbers, categories and issues involved in the PSAs. But following a highly public patient safety failure that resulted in the death of a patient, the QOC decided that it could not discharge its fiduciary responsibilities if it did not understand how the most serious PSAs were being addressed. Now the QOC reviews all red PSAs (i.e., the most severe events), assessing whether the reports adequately identify the issues and the necessary actions to avoid a repetition of these events. The QOC is now the only body authorized to sign off and close a red PSA. On average, there are three red PSAs per month.
The success of a quality committee such as that at Virginia Mason depends on a clear understanding by committee members that they are focused on assessing the investigation process, not the specific outcomes. Such a committee needs strong leadership, dedicated and experienced members and effective work processes. The board chair at Virginia Mason noted that board members were aware of the tension between governance and operations: "There are two things here that I would characterize as being different from other places where I have worked. One is that there is a sufficient level of sophistication on the board from their prior experience that they know where to draw that line [between policy and operations]. Or they learn it quickly in this setting."
Effective Relationships between the Board, Medical Staff and Senior Leadership
The capability of boards and board quality committees to function effectively and to move appropriately between fiduciary, strategic and generative modes relies on trust as well as skills. Boards, senior leadership and medical staff need to develop an understanding of each other's roles and create strong collaborative relationships for achieving the organization's goals. Effective relationships can require new structures and approaches. When Vancouver Island Health Authority was established in 2001, the MAC was composed of 50 members and 80 quality councils and committees. Beyond the cumbersome nature of this structure, the Health Authority MAC was focused on traditional medical quality assurance, and some physicians were hesitant to embrace the shift from a blame culture to a culture that emphasized learning and understanding the broader system contexts for adverse events. The agenda of the Health Authority MAC was focused on credentialing, disciplinary issues, bylaws and little else. Changes in these structures take time, and leadership is needed to align medical staff structures with new board roles and expectations. To help build trust and communicate new approaches, the Vancouver Island Health Authority board makes a point of meeting with local physicians at every meeting, rotating its meeting location around the region.
Better alignment between medical staff and administrative structures can mean changing the medical leadership structure and developing new leadership. The Ottawa Hospital has placed considerable emphasis on reorganizing the key roles and committees, emphasizing the quality and patient safety dimensions of the vice-president medical role and integrating structures to facilitate the review of issues related to clinical, financial and operations portfolios.
Executing Effective Governance for Quality and Safety
Despite growing agreement that boards need to assume fiduciary responsibilities for quality and safety, many boards appear to struggle to execute effectively. One approach for improving healthcare board performance in quality and patient safety draws on creating structures and processes analogous to financial oversight and performance review. In quality, like finance, goals need to be established, relevant indicators selected, progress monitored and appropriate action taken if goals are not achieved (Hundert and Topp 2003). The Saskatoon Health Region has adopted an approach that incorporates these elements. The board sees its role in relationship to quality as setting direction, monitoring and asking good questions. Board members review reports and dashboards and then "ask questions about what kind of processes have changed to prevent this from happening or to keep making improvement," explained one Health Region board member.
Recent efforts by some US hospitals, adopting ideas from the IHI's Boards on Board campaign, go beyond this approach, emphasizing efforts to deepen the engagement of board members and encourage more ambitious aims in improving care. In particular, IHI argues that boards need to "put a human face" on harm data, reviewing specific cases where patients experienced harm while receiving care. Boards also need to commit to creating and spreading a just culture and to adopting policies and practices that encourage the disclosure of adverse events and resolving issues that led to harm. Many US hospitals appear to be following this advice, as do some Canadian hospitals.
Discussion
Based on the information gathered for this report, there appear to be a number of key elements necessary for boards to fulfill their responsibilities on quality and patient safety. These are displayed in Figure 1. Each element is critical, but elements are also interdependent – effective performance relies on the information available about quality of care, and also on the knowledge of quality and safety and the governance skills of trustees.
One critical issue facing boards is the need to clarify their role in improving quality and patient safety versus the roles of leadership and medical staff. Traditionally, boards have delegated responsibilities for quality issues to medical staff, in particular, the MAC, which reports to the board. This approach is inconsistent with the board's accountability for setting goals and monitoring performance (Reinertsen 2008). Yet the MAC and senior management have continued responsibilities to identify and resolve issues and to support the board. Thus, a revision of current structures and the creation of more explicit "compacts" (Silversin and Kornacki 2002) that clarify the expectations and roles of the board, medical staff and management are keys to creating more effective healthcare organization governance. Board leadership and skills are critical elements, but effective governance requires the participation of many parties, along with the investment of time and new resources to create and sustain high levels of performance.
Effective governance for quality and safety is first and foremost based on generic good governance practices. Prybil notes that high-performing hospital boards are those in which there is an "'extensive exchange of views before decisions are made' and where 'constructive questions and scepticism' dominate the boardroom deliberations" (2006: 226). These findings echo the thoughts of Sonnenfeld (2002), who noted that the key to exemplary boards is the existence of "robust, effective social systems." Such boards generate "a virtuous cycle of respect, trust, and candor" and foster a culture of open and constructive dissent (Sonnenfeld 2002: 4). Board processes in the oversight of quality and patient safety build on their capabilities to act collectively as effective governors.
Canadian healthcare organizations are largely funded by provincial and territorial governments that provide strategic direction and exert regulatory control. Ministers of health appoint regional health authority board members; indeed, in some provinces they do so without any input from the managers of these regions. While regions maintain some operational autonomy within a broader strategic and fiscal framework (as do hospitals and long-term care organizations in Ontario), these entities are clearly limited in the extent to which they can initiate and fund new strategic directions. Thus, governance in Canadian healthcare ultimately reflects the interests and intents of provincial governments. Regional and organizational initiatives to improve the quality of care and patient safety occur within a broader policy and financial framework that may acknowledge the critical nature of these objectives but may not always provide commensurate resources to achieve them.
Expanding reports of quality and patient safety problems, and more explicit accountability agreements between governments and healthcare organizations have created growing pressures for healthcare organizations to improve the quality and safety of care they provide. Recent research coupled with well-publicized campaigns suggest that boards can be effective in helping to focus attention on these issues, setting strategic aims, monitoring performance and holding CEOs accountable for this performance.
This broadening of fiduciary responsibilities is neither simple nor easy because it requires important changes in the work and membership of boards. Boards need better information about quality and safety in their organization, including a performance dashboard that organizes key measures and provides an ongoing assessment of performance on strategic goals. Boards need to recruit new members whose expertise in this area will guide quality committees and improve the dialogue with senior administrative and clinical leadership. Boards and management also need to support efforts to deepen the knowledge of quality and safety issues for all board members.
Conclusions
In adopting a greater focus on quality and patient safety, board members need to develop knowledge and judgment concerning the factors influencing quality and safety of care, without losing sight of their responsibilities to remain focused on the strategic issues. A more co-operative approach on governance does not exclude the importance of a clear accountability framework and relationships between senior leadership and boards. But it underlines the need to go beyond monitoring and control to focus also on how boards can help organizations to develop the internal capacity for continuous improvement.
About the Author(s)
G. Ross Baker, PhD, is a professor in the Department of Health Policy, Management and Evaluation at the University of Toronto, Toronto, Ontario.
Jean-Louis Denis, PhD, is a professor in the Département d'Administration de la Santé, Université de Montréal, Montréal, Québec.
Marie-Pascale Pomey, PhD, is an associate professor in the Département d'Administration de la Santé, Université de Montréal.
Anu MacIntosh-Murray, PhD, is a consultant and member of the Department of Health Policy, Management and Evaluation at the University of Toronto.
Acknowledgment
The research reported in this paper was supported by funding from the Canadian Health Services Research Foundation and the Canadian Patient Safety Institute. The authors thank Johanne Preval for her invaluable assistance on this project.References
Baker, G.R., P.G. Norton, V. Flintoft, R. Blais, A. Brown, J. Cox, E. Etchells, W.A. Ghali, P. Hébert, S.R. Majumdar, M. O'Beirne, L. Palacios-Derflingher, R.J. Reid, S. Sheps and R. Tamblyn. 2004. "The Canadian Adverse Events Study: The Incidence of Adverse Events among Hospital Patients in Canada." Canadian Medical Association Journal 170(11): 1678–86.
Bruce, S., H. Prior, A. Katz, M. Taylor, S. Latosinsky, P. Martens, C. De Coster, M. Brownell, R.-A. Soodeen and C. Steinback. 2006. Application of Patient Safety Indicators in Manitoba: A First Look. Winnipeg, MB: Manitoba Centre for Health Policy. Retrieved August 29, 2008. <http://mchp-appserv.cpe.umanitoba.ca/reference/patient.safety.pdf>.
Canadian Institute for Health Information. 2008. Health Indictors 2008. Ottawa, ON: Canadian Institute for Health Information.
Carver, J. 2006. Boards That Make a Difference: A New Design for Leadership in Non-profit and Public Organizations (3rd ed). San Francisco, CA: Jossey-Bass.
Chait, R.P., W.P. Ryan and B.E. Taylor. 2005. Governance as Leadership. New York: John Wiley and Sons.
Coffey, A. and P. Atkinson. 1996. Making Sense of Qualitative Data: Complementary Research Strategies. Thousand Oaks, CA: Sage.
Conway, J. 2008. "Getting Boards on Board: Engaging Governance in Quality and Safety." Joint Commission Journal on Quality and Patient Safety 34(4): 214–20.
Furman, C. and R. Caplan. 2007. "Applying the Toyota Production System: Using a Patient Safety Alert System to Reduce Error." Joint Commission Journal on Quality and Patient Safety 33(7): 376–86.
Health Quality Council. 2007. Quality of Surgical Care in Saskatchewan: A Look at Eight Complex Procedures. Saskatoon, SK: Health Quality Council.
Hundert, M. and A. Topp. 2003. "Issues in the Governance of Canadian Hospitals IV: Quality of Hospital Care" Hospital Quarterly 6(4): 60–62.
Institute for Healthcare Improvement. 2008. Getting Started Kit: Governance Leadership "Boards on Board" How-to Guide. Cambridge, MA: Author. <www.ihi.org>.
Jiang, H.J., C. Lockee, K. Bass and I. Fraser. 2009. "Board Oversight of Quality: Any Differences in Process of Care and Mortality?" Journal of Healthcare Management 54(1): 15–29.
Kvale, S. 1996. InterViews. An Introduction to Qualitative Research Interviewing. Thousand Oaks, CA: Sage.
Lofland, J. and L.H. Lofland. 1995. Analyzing Social Settings: A Guide to Qualitative Observation and Analysis (3rd ed.). Belmont, CA: Wadsworth Publishing Co.
Miles, M.B. and A.M. Huberman. 1994. Qualitative Data Analysis: An Expanded Sourcebook (2nd ed.). Thousand Oaks, CA: Sage Publications Inc.
Prybil, L.D. 2006. "Size, Composition and Culture of High Performing Hospital Boards" American Journal of Medical Quality 21(4): 224–29.
Reinertsen, J.L. 2007, June. Boards, Dashboards and Data. Presented at From the Top: Getting the Boards on Board, Boston, MA.
Reinertsen, J.L. 2008. "Part 02 – Board Leadership in Clinical Quality: A US Perspective" In Quality and Patient Safety: Understanding the Role of the Board. Toronto, ON: Ontario Hospital Association.
Rose, J.S., C.S. Thomas, A. Tersigni, J.B. Sexton and D. Pryor. 2006. "A Leadership Framework for Culture Change in Health Care" Joint Commission Journal on Quality and Patient Safety 32(8): 433–42.
Silversin J. and M.J. Kornacki. 2002. "Creating a Physician Compact That Drives Group Success" Medical Group Management Journal 47: 54–62.
Slessor, S.R., J.B. Crandall and G.A. Nielsen. 2008. "Case Study: Getting Boards on Board at Allen Memorial Hospital, Iowa Health System" Joint Commission Journal on Quality and Patient Safety 34(4): 221–27.
Sonnenfeld, J.A. 2002. "What Makes Good Boards Great" Harvard Business Review 80(9): 106–13.
Taylor, B.E., R.P. Chait and T.P. Holland. 1996. "The New Work of the Nonprofit Board" Harvard Business Review 74(5): 36–38, 40, 42–46.
Vaughn, T., M. Koepke, E. Kroch, W. Lehrman, S. Sinha and S. Levey. 2006. "Engagement of Leadership in Quality Improvement Initiatives: Executive Quality Improvement Survey Results" Journal of Patient Safety 2(1): 2–9.
Yin, R.K. 2003. Case Study Research: Design and Methods (3rd ed.). Thousand Oaks, CA: Sage.
Additional or Related Reading
Accreditation Canada. 2008. Standards for Sustainable Performance v2. Ottawa, ON: Author.
Alexander, J.A., S.Y.D. Lee, V. Wang and F.S. Margolin. 2009. "Changes in the Monitoring and Oversight Practices of Not-for-Profit Hospital Governing Boards 1989–2005 Evidence from Three National Surveys" Medical Care Research and Review 66(2): 181–96.
Alexander, J.A., B.J. Weiner and R.J. Bogue. 2001. "Changes in the Structure, Composition, and Activity of Hospital Governing Boards, 1989–1997: Evidence from Two National Surveys" Milbank Quarterly 79(2): 253–79.
Alexander, J.A. and S.Y.D Lee. 2006. "Does Governance Matter? Board Configuration and Performance in Not-for-Profit Hospitals" Milbank Quarterly 84(4): 733–58.
Broadbent Panel on Accountability and Governance in the Voluntary Sector. 1999. Building on Strength: Improving Governance and Accountability in Canada's Voluntary Sector – Final Report. Ottawa, ON: Author.
Callender, A.N., D.A. Hastings, M.C. Hemsley, L. Morris and M.W. Peregrine. 2007. Corporate Responsibility and Health Care Quality: A Resource for Health Care Boards of Directors. Washington, DC: US Department of Health and Human Services Office of Inspector General and American Health Lawyers Association.
Centers for Medicare and Medicaid Services. 2006. Hospital Leadership Summit: Moving from Good to Great. Summary of Conference Proceedings. Baltimore, MD: Author.
Corbett, A. and M. Baker. 2008. "Part 01 – Quality and Safety in Ontario Hospitals" In Quality and Patient Safety: Understanding the Role of the Board. Toronto, ON: Ontario Hospital Association.
Dalton, D.R., C.M. Daily, A.E. Ellstrand and J.L. Johnson. 1998. "Meta-analytic Reviews of Board Composition, Leadership Structure, and Financial Performance" Strategic Management Journal 19: 269–90.
Denis J.L., F. Champagne, M.P. Pomey, J. Préval and G. Tré. 2005. Towards a Framework for the Analysis of Governance in Health Care Organizations. Preliminary report presented to the Canadian Council on Health Services Accreditation, October 2005, Université de Montréal, Montréal, PQ.
Fyke, K.J. 2002. Caring for Medicare: Sustaining a Quality System. Regina, SK: Saskatchewan Commission on Medicare. <http://www.health.gov.sk.ca/medicare-commission-final-report>. (Accessed May 12, 2008)
Health Quality Council of Alberta. 2007. Review of the Infection Prevention and Control and CSR Sterilization Issues in East Central Health Region. Edmonton, AB: Author.
Institute of Medicine. 2001. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy of Sciences.
Jiang, H.J., C. Lockee, K. Bass and I. Fraser. 2008. "Board Engagement in Quality: Findings of a Survey of Hospital and System Leaders" Journal of Healthcare Management 53(2): 121–34.
Joint Commission on Accreditation of Healthcare Organizations. 2008. Standards Revisions. Oakbrook Terrace, IL: Author.
Kirby, M.J.L. 2002. The Health of Canadians – The Federal Role: Interim Report. Volume Five: Principles and Recommendations for Reform – Part I. Ottawa, ON: Standing Senate Committee on Social Affairs, Science and Technology. Retrieved May 12, 2008. <http://www.parl.gc.ca/37/1/parlbus/commbus/senate/com-e/soci-e/rep-e/repapr02vol5-e.htm>.
Kroch, E., T. Vaughn, M. Koepke, S. Roman, D. Foster, S. Sinha and S. Levey. 2006. "Hospital Boards and Quality Dashboards" Journal of Patient Safety 2(1): 10–19.
Lockee, C., K. Droom, E. Zablocki and B. Bader. 2006. Quality. San Diego, CA: The Governance Institute.
Lohr, K.M., ed. 1990. Medicare: A Strategy for Quality Assurance. Washington, DC: National Academy Press.
Martin, L., E. Nelson, R. Lloyd and T. Nolan. 2007. Whole System Measures. Cambridge, MA: Institute for Healthcare Improvement.
Milstein, A. 2009. "Ending Extra Payment for 'Never Events' – Stronger Incentives for Patients' Safety" New England Journal of Medicine 360(23): 2388–90.
Nadler, D.A. 2004. "Building Better Boards" Harvard Business Review 82(5): 102–11.
National Quality Forum. 2004. Hospital Governing Boards and Quality of Care: A Call to Responsibility. Washington, DC: Author.
Ontario Health Performance Initiative. 2007. Survey of Ontario Healthcare Organizations on Quality Structures and Processes. Toronto: Author.
Ontario Hospital Association. 2007. Governance Survey Overall Results. Toronto, ON: Author.
Ontario Hospital Association. 2008. Quality and Patient Safety: Understanding the Role of the Board. Toronto, ON: Author.
Orlikoff, J.E. 2005. "Building Better Boards in the New Era of Accountability" Frontiers of Health Services Management 21(3): 3–12.
Pointer, D.D. and J.E. Orlikoff. 2002. Getting to Great: Principles of Health Care Organization Governance. San Francisco, CA: Jossey-Bass.
Rhodes, R.A.W. 1997. Understanding Governance: Policy Networks, Governance, Reflexivity, and Accountability. Buckingham, United Kingdom: Open University Press.
Romanow, R.J. 2002. Building on Values: The Future of Health Care in Canada. Ottawa, ON: The Commission on the Future of Health Care in Canada. Retrieved May 12, 2008. <http://www.hc-sc.gc.ca/hcs-sss/alt_formats/hpb-dgps/pdf/hhr/romanow-eng.pdf>.
Salamon, L.M. 2002. "The New Governance and the Tools of Public Action: An Introduction" In L.M. Salamon, ed., The Tools of Government: A Guide to the New Governance. New York: Oxford University Press.
Sarbanes-Oxley Act. 2002. United States Pub. L. 107-204, 116 Stat. 745, enacted July 30, 2002.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed