
Healthcare Policy
Exploring Wait List Prioritization and Management Strategies for Publicly Funded Ambulatory Rehabilitation Services in Ontario, Canada: Further Evidence of Barriers to Access for People with Chronic Disease
Abstract
Background: Timely access to publicly funded health services is a priority issue across the healthcare continuum in Canada. The purpose of this study was to examine wait list management strategies for publicly funded ambulatory rehabilitation services in Ontario, Canada.
Methods: Ambulatory rehabilitation services were defined as community occupational therapy (OT) and physiotherapy (PT) services. A mailed self-administered questionnaire was sent to all 374 Ontario publicly funded sites. Descriptive statistics were used to explore management strategies.
Results: The response rate was 57.2%. Client acuity was the most common method used to prioritize access across all settings. The most frequently reported methods to manage wait lists included teaching self-management strategies (85.0%), implementing attendance policies (69.5%) and conducting wait list audits (67.3%).
Conclusions: Ambulatory rehabilitation settings have implemented a number of strategies for wait list management. The results of this study suggest that an increasing number of Ontarians encounter barriers when accessing publicly funded ambulatory rehabilitation services.
As shifts in the demographic characteristics of the population continue to occur at an unprecedented pace, and as other factors affecting supply and demand for healthcare change over time, timely access to comprehensive health services has become elusive (Murray et al. 2002). Multiple demands on healthcare systems are occurring across the continuum, and much of the policy focus has recently been placed on wait times for surgical and diagnostic services (CIHI 2005; OMHLTC 2006; Esmail and Walker 2002; Frankel et al. 1999; Juni et al. 2003; Trypuc et al. 2006). Despite the ongoing research and policy interest in the hospital-based aspects of care delivery, others have noted that wait lists for community-based services have become overshadowed by surgical and medical wait times (Young and Turnock 2001). A recent study examining wait times for community rehabilitation indicated that individuals with chronic conditions have excessive wait times for outpatient and community occupational therapy (OT) and physiotherapy (PT) services in Ontario, particularly if these individuals are waiting for services in hospital outpatient departments (Passalent et al. 2009). The consequences of lack of access to rehabilitation services have been explored previously, and the outcomes seem to suggest that individuals who require and receive services are statistically more likely to self-report improved health status compared to those who are unable to access services (Landry et al. 2007). Landry and colleagues (2007) suggest that given the association between poor self-reported health status, morbidity and mortality, future research needs to examine the long-term impact to determine the extent to which barriers to access, including long wait times, may be associated with increased utilization of hospitals and family physicians.
As chronic disease continues to place increasing demands on the healthcare system, some chronic conditions such as arthritis, musculoskeletal disorders and stroke are more likely than other conditions to be associated with disability, and are presumably more likely to require rehabilitation intervention to optimize function, mobility and independence in the community (Barr et al. 2003; Wagner 1998; Rothman and Wagner 2003; Beaglehole et al. 2007; Tsasis and Bains 2009). Moreover, the recent shift in emphasis for service delivery from hospital-based to community-based settings has resulted in additional demand on community rehabilitation providers (Landry et al. 2007; Baranek et al. 2004; Randall and Williams 2006). These factors, in combination, appear to be placing increased demand on rehabilitation service provision and therefore affecting timely access to appropriate healthcare providers.
Few studies have examined wait lists and wait times for outpatient PT and OT services. For instance, the provincial regulatory body for physiotherapists in Ontario reported that patients waited, on average, 10 days longer for urgent PT outpatient care through hospitals than through community PT clinics (College of Physiotherapists of Ontario 2000). In a 2007 study of rehabilitation in primary care, wait times were found to be shorter in privately funded practice settings compared to publicly funded settings, and for acute patient populations compared to those with chronic conditions (Cott et al. 2007). The literature that has examined community OT wait times indicates that over half of community occupational therapists wait an average of one week or less from receipt of referral to a client's first visit (Cott et al. 2007). Furthermore, data from the 2004 Ontario Auditor General's report of community healthcare services suggest that 45.6% of all people waiting for such services were waiting for home-based OT (Auditor General of Ontario 2004).
Most recently, an Ontario study (Passalent et al. 2009) indicates that (a) wait times for community PT were longer than OT wait times, with the median wait time for OT and PT being 12.5 and 35 days, respectively; (b) maximum wait times for PT are more than twice as long compared to maximum wait times for OT (114 days waiting for PT compared to a maximum of 63 days waiting for OT); and (c) over 10,000 people reported waiting for OT or PT services across Ontario. Despite this limited examination of wait time and wait lists for outpatient and community rehabilitation services, little in the literature examines the management of these extensive wait lists. The purpose of this study was to explore the various wait list management strategies currently used for OT and PT services across publicly funded outpatient and community settings in Ontario.
Methods
In order to explore wait list prioritization and management strategies used within publicly funded ambulatory rehabilitation services, we employed a mail-out survey across Ontario. The development of the survey tool has been reported elsewhere (Passalent et al. 2009) and will be only briefly reviewed in this paper. The study protocol was approved by the University Health Network Research Ethics Board, Toronto, Ontario, Canada.
Survey development process
Individuals working in a management position in outpatient OT and PT settings across Ontario were invited in July 2006 to participate as key informants to obtain information on the extent, management and perceptions of wait lists in community-based rehabilitation in Ontario, and to inform the development of the questionnaire used in the survey. A purposive, snowball sample of healthcare providers involved in community-based rehabilitation were invited to participate as key informants in this study. The purpose of the sampling was to ensure that key informants represented a range of community-based rehabilitation settings, geographic settings and health professions. Key informants were identified by the researchers as known experts or those who were in a position to discuss current issues surrounding wait times and wait lists in community-based rehabilitation. These individuals were identified through existing and emerging contacts with professional associations, rehabilitation academics and service delivery organizations. A semi-structured interview guide was developed for the key informant interviews based on review of recent national and international peer-reviewed and grey literature on the topic of waiting times and rehabilitation. Questions regarding wait time and wait list measurement, management of wait lists and perceptions of the impact of community-based rehabilitation wait times and wait lists on the healthcare system were posed to key informants. Data were collected during the key informant interviews using written field notes and audiotape. Audiotapes were not transcribed but were used as a supplement to field notes when the interviews were summarized.
A questionnaire was developed based on the results of the key informant interviews. The key informants reviewed the survey and made important suggestions regarding the clarity, scope and feasibility of completing the questionnaire. This process served to strengthen the questionnaire's face and content validity, clarity, relevance and format. Among the more important findings gained from the key informants was that wait times and wait lists are generally not an important issue among settings that deliver privately funded rehabilitation services. For instance, a private for-profit clinic that delivers rehabilitation services funded through private sources (e.g., out-of-pocket, third-party insurance) and quasi-public sources (e.g., workers' compensation insurance, motor vehicle accident insurance) generally do not have wait lists or long wait times to access services. As a result, we did not sample private for-profit clinics or other privately owned settings that access private funding for service delivery in this survey; rather, we sampled not-for-profit settings that deliver publicly funded services.
We acknowledge that restricting our sample limits the generalizability of our analysis; on the other hand, it did allow us to explore these issues with a relatively homogenous cohort. Nevertheless, we chose to include designated physiotherapy centres (DPCs), formerly known as schedule 5 clinics, in the study sample because, although they are privately owned and operate on a for-profit basis, they invoice the Ontario Hospital Insurance Plan (OHIP) for services on a fee-for-service basis, which qualifies them as delivering publicly funded services. DPCs provide publicly funded community-based PT services, and there are no equivalent structures for OT in the province of Ontario.
Sampling
In this study, community rehabilitation managers, professional practice leaders or senior therapists of all (N=374) publicly funded outpatient and community sites that provide OT and/or PT services to adults (age 19 years and older) in Ontario were surveyed using a self-administered mailed questionnaire. This included hospital outpatient departments (OPDs); community health centres (CHCs); community care access centres (CCACs); the Arthritis Society Rehabilitation and Education Program (AREP); and designated physiotherapy clinics (DPCs).1 Community rehabilitation services provided through mental health institutes or institutes that provide rehabilitation to children and adolescents, as well as specialty ambulatory programs (such as amputee programs or hand clinics), were excluded.
Identification of all the sites and key contact persons who provide publicly funded outpatient and community OT and PT services in Ontario was obtained from the following sources: the Ontario Ministry of Health and Long-Term Care website (for DPCs, n=93); the Ontario Hospital Association website (for Hospital OPDs, n=208); the Ontario Association of Community Care Access Centres (for CCACs, n=42); the College of Occupational Therapists of Ontario; the College of Physiotherapists of Ontario (for OTs and PTs working in CHCs, n=10); and the Senior Director of Client Programs, AREP (for regional directors of client services and individual therapists, n=21). Where necessary, organizations were contacted directly by telephone to identify the most appropriate person in the organization to receive the questionnaire. A key contact was identified for each setting for PT services and for OT services. If there was one contact for both PT and OT services, this individual served as the single key contact for the setting.
Potential participants were mailed an information letter, a questionnaire and a pre-paid return envelope on November 14, 2005. Three weeks after the initial mailing, all non-respondents were mailed a second information letter, a questionnaire and a pre-paid return envelope. The final cut-off date for returned questionnaires was January 12, 2006. Return of a completed questionnaire implied informed consent. The data from the questionnaires were entered into a database management system (Access for Windows 2000). Double data entry was undertaken to ensure data quality.
Key study variables/measures
SETTINGS
Settings included hospital outpatient departments; community health centres (CHCs); community care access centres (CCACs); the Arthritis Society Rehabilitation and Education Program (AREP); and designated physiotherapy clinics (DPCs) that provided either community outpatient occupational therapy, physiotherapy or both.
GEOGRAPHIC REGION
Outpatient and community OT and PT settings were defined as urban or rural using Canada Post's most basic definition as indicated by the second digit of the respondent's postal code. The number "0" indicates a rural location, and the numbers "1" through "9" indicate an urban location.
WAIT LIST MANAGEMENT STRATEGIES
A list of 14 management strategies was provided (based on the results of a literature review and the key informant interviews). These included: use a centralized wait list (a single wait list for all patients within a setting or with other OT/PT facilities or institutions); hire more staff; allow clients with episodic needs to re-enter rehabilitation without having to re-enter the system at the point of screening/referral; accept only in-house referrals (i.e., a specific clinical setting does not accept community referrals); provide education to clients regarding self-management; ensure strict enforcement of attendance policies; use group intervention rehabilitation for patients with similar conditions; use an "ad hoc" appointment to start the patient on a simple home program while the patient awaits assessment; use rehabilitation assistants to offset intervention time; use evidence-based benchmarks for wait list management; use guaranteed maximum waiting times; audit routine wait lists to determine whether clients awaiting assessment continue to require rehabilitation services; refer wait-listed clients to other clinics or facilities; use a computerized wait list to track referrals and wait times. Respondents were asked which wait list management strategies they have used in the past, currently used or never used. They were also asked to rate the perceived effectiveness of strategies they used to manage wait lists.
METHODS TO PRIORITIZE WAIT LISTS
A list of 10 ways of prioritizing wait lists was provided. Respondents were asked which methods they had ever used and which they used most frequently.
EFFECTIVENESS OF MANAGEMENT STRATEGIES
The choices were very effective, somewhat effective and not at all effective.
Data analysis
Descriptive statistics were used to describe the study sample, to summarize results from the study questionnaires and to address the study objectives. SAS Version 9.1 was used for all analyses. Open-ended response items from the questionnaire were entered into N6/NVivo, coded and analyzed in order to explore the key informants' beliefs and interpretations of the status of their wait list management. The qualitative analysis allowed for a rich description of the issues being explored, and permitted some degree of interpretation of the quantitative data.
Results
The overall response rate to the survey was 57.2%, or 214 out of a possible 374 responses. As indicated in Table 1, the response rates according to each setting were as follows: CCAC (45.2%), CHC (70.0%), OPD (58.7%), DPC (50.5%) and AREP (90.5%).
The majority of the respondent settings were located in urban locations. The proportion of settings reporting that they have a wait list varied. Thirty-six per cent of DPCs reported having a wait list, whereas more than 85% of OPDs and AREP reported having a wait list for OT outpatient services, PT outpatient services or both.
| TABLE 1. Description of sample by setting | |||||
| Characteristic | Setting | ||||
| Community Care Access Centres n (%) | Community Health Centres n (%) | Hospital Outpatient Departments n (%) | Designated Physiotherapy Clinics n (%) | The Arthritis Society Rehabilitation and Education Program n (%) | |
| OT services only | 0 | 2 (28.6) | 18 (14.8) | n/a | 4 (21.1) |
| PT services only | 0 | 5 (71.4) | 75 (61.5) | 47 (100) | 10 (52.6) |
| OT and PT services | 19 (100) | 0 | 29 (23.8) | n/a | 5 (29.3) |
| Urban setting | 19 (100*) | 7 (100) | 85 (69.7) | 47 (100) | 19 (100*) |
| Report having a waiting list for OT or PT outpatient services | 9 (47.4) | 5 (71.4) | 108 (87.8) | 17 (36.2) | 18 (94.7) |
| OT = occupational therapy; PT = physiotherapy; n/a = not applicable | |||||
| * Although community care access centres and the Arthritis Society Rehabilitation and Education Program centres are all located in urban settings, services offered by these settings can extend to rural communities. | |||||
Approaches used to prioritize wait lists
Respondents across all settings described the challenges they face when dealing with long wait lists. For instance, as one respondent from a hospital outpatient department (OPD) reported, "You do the best you can with the ever-decreasing resources, giving some attention to those that have greater potential for rehabilitation. The rest either wait or get nothing." The primary way in which to prioritize clients was by acuity, and was reported across all settings (see Figure 1). In other words, clients who presented with greater acuity were ranked as a higher priority for ambulatory rehabilitation services across Ontario. Respondents indicated that chronic conditions have the lowest priority; according to one professional in a community setting, "We will put re-referrals for the same person and the same condition, especially if it is a chronic condition and physio didn't help the first time, at the bottom of the wait list." The other common strategies to prioritize wait lists included chronology, referral source, client complexity and other. There was wide variation in the proportion of different methods used by each setting. For example, CCACs used a number of different prioritization methods, whereas DPCs used primarily acuity and chronological prioritization methods.

Wait list management strategies
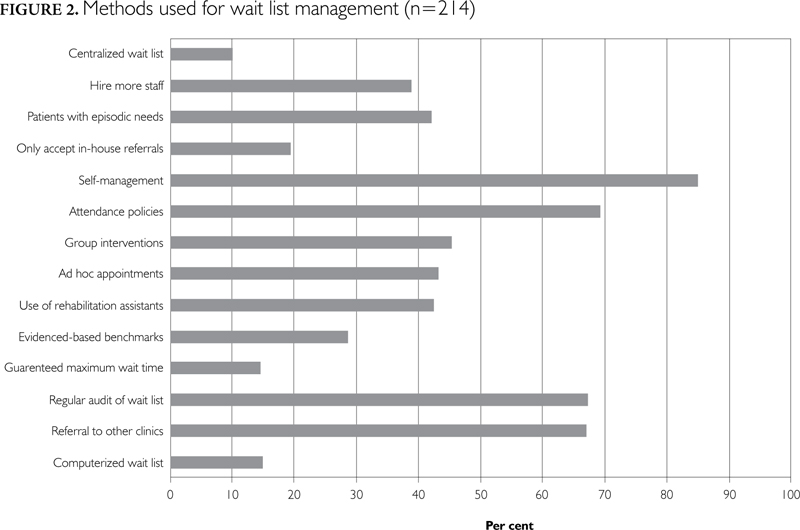
The most common methods used to manage wait lists are presented in Figure 2. Self-management methods (e.g., education pamphlets, generalized exercise) (85%) were the most commonly used, followed by attendance policies (69.5%), regular wait list audits (67.3%) and referral to other clinics (67.0%). The least common methods to manage wait lists included the use of a computerized wait list management system (14.8%), guaranteed maximum wait times (14.5%) and centralized wait lists (10.1%).
The most common wait list management strategies used by hospital OPDs included prioritizing wait lists by acuity or referral source, encouraging clients to utilize other community-based services and educating referral sources. Many hospital OPDs described putting clients with chronic musculoskeletal conditions at the bottom of the list. As one respondent reported, "We have closed our wait list and no longer accept chronic referrals (only acute referrals and specialty programs accepted)."
Encouraging patients to utilize other rehabilitation services by providing information about other PT clinics is one strategy that is often used, but it is limited in effectiveness owing either to the lack of other publicly funded options or to clients' inability to pay because of lack of private insurance. This situation arose particularly in rural and remote areas. As one rural hospital OPD stated, "Geographically, we are quite isolated. For much of our clientele, a private clinic would be over 50 kilometres away … so we're it." One respondent concluded, "Many patients are denied treatment as a result [because] they cannot afford private." The partial delisting of designated physiotherapy clinics has also limited the options available. "We used to refer patients to [DPCs] … but this is very limited now due to changes in Ministry of Health guidelines."
Hospital OPDs are in a relatively unique position in that they do not receive their funding directly from OMHLTC; rather, their funding comes through their hospital's global budget. As a result, they are more limited than other settings in their ability to utilize various wait list management strategies. Whereas a DPC has the option to hire more staff to meet wait list demands, a hospital OPD must compete with other services within the hospital for funding. As one respondent stated, "We continue to put in increased staffing requests but have been restricted by the hospital budget." Another said, "We have discontinued seeing or accepting referrals for chronic musculoskeletal disorders since we can't see them in a timely manner anyway. We don't have the ability to hire more staff. Our priority is to support post-total joint replacements and acute orthopaedic injuries (within 6 weeks)."
Further, some respondents reported that in response to the need to balance budgets, many hospitals are considering reducing outpatient rehabilitation services in order to save money. In some of these situations, the hospital OPD represents the only publicly funded outpatient rehabilitation service in the region (often rural or remote), leaving huge issues of access to community-based rehabilitation for Ontario residents living in these areas.
The survey also asked respondents to rank the perceived effectiveness of their wait list management strategies (Figure 3). Based on self-reports, self-management, attendance policies, regular wait list audits and referrals to other clinics were identified as the most commonly used management methods; however, these were not the methods identified as most effective. Over half of respondents (54.2%) reported that self-management is an effective wait list management strategy, whereas only about a third (36.3%) found attendance policies to be effective. Not surprisingly, hiring more staff was seen as the most effective method (71.2%), followed by the use of evidence-based benchmarks (65.4%), accepting only in-house referrals (64.5%) and using rehabilitation assistants (64.0%).

Discussion
Acuity of condition is the primary way in which publicly funded rehabilitation settings prioritize clients on wait lists in the province of Ontario. However, it is unknown whether this method, or other methods, is effective in prioritizing wait lists in rehabilitation settings. A study examining the accuracy of referral priorities for OT within the United Kingdom indicated that 56% of low-priority cases were inappropriately prioritized, with a tendency to underestimate an accurate level of priority (Wright and Ritson 2001). While many agree that patients should be prioritized on a wait list based on need, and that this prioritization should be based on the best possible evidence (OMHLTC 2004; Wait Time Alliance 2005; Shortt and Shaw 2003; Sanmartin et al. 2000; Elwyn et al. 1996; DeCoster 2002; Meiland et al. 2002; Western Canadian Waiting List Project 2001), few organizations implement evidence-based practice for prioritization within rehabilitation settings (GTA Rehab Network 2003).
In terms of managing wait lists, the use of centralized wait list management systems was not a common approach. The literature suggests, however, that the use of a central referral system allows patients to be triaged to the appropriate service, ensuring that there is no duplication of referrals and that appropriate referrals are received and managed through a systematic process (Maddison et al. 2004). Centralized systems facilitate wait list management by redirecting referrals to clinicians with shorter waiting times (OMHLTC 2004; Sanmartin et al. 2000). In the United Kingdom, the use of centralized systems reduced wait times for PT from 16 to four weeks and decreased non-attendance rates from 18% to 2% (Pattinson 2003). The Auditor General of Ontario (2004) has recommended the establishment of consistent policies for maintaining centralized wait lists for community rehabilitation services in lieu of the common practice of maintaining separate lists by individual service providers.
An essential component of the centralized wait list management strategy is the need to perform regular audits to ensure that patients are listed appropriately (Romanow 2002; Sanmartin et al. 2000; Elwyn et al. 1996; Sullivan and Baranek 2002). Wait lists may be inflated by 20% to 30% owing to a change in condition, the patient's death or move from the jurisdiction, change of mind regarding the procedure, or resolution of symptoms (McDonald et al. 1998). Despite these evidence-based findings, very few respondents reported using this management strategy. Further inquiry into why this approach is seldom used for community and outpatient OT and PT wait list management would be beneficial.
Despite findings in the literature suggesting specific strategies for wait list management, few settings employed evidence-based strategies, as indicated above. A recent review examining the determinants of wait time management suggests that culture, human resources and information management tools are important factors for successful wait time management (Pomey et al. 2008). In their work, Pomey and colleagues used a mixed-methods approach to report that wait list management appears not to have been a linear process across Canada; rather, there are a multitude of interacting complex factors. In order to improve wait list management approaches, these authors suggested a series of factors, raging from increased physician involvement to targeted funds. Given the few empirical studies in this particular area, future health services research may be warranted to examine the impact (or lack thereof) of such factors on wait list management strategies used in community rehabilitation settings.
The results presented in our study add to the growing body of evidence indicating that the various management methods used by outpatient physiotherapy clinics do not necessarily help to ameliorate the barriers to access to community physiotherapy services for persons with chronic disease. As found in the study by Passalent and colleagues (2009), people with chronic disease make up the largest proportion of those waiting for physiotherapy services, and this situation is compounded by management strategies that further disadvantage this patient population, such as prioritization based on acuity, that were found in all the settings we surveyed. This finding highlights the issue of potential complications, such as prolonged dependency on social benefits and indirect societal costs that may arise from the inability of patients with chronic conditions to seek service. For instance, persons with chronic diseases such as arthritis and stroke contribute the most to the burden of disease in Canada (Health Canada 2003; Perruccio et al. 2004; BC Ministry of Health 2004), and the projected rates of chronic diseases by the year 2028 (for those aged 65 and older) will constitute 20.3% of Ontario's population (Ontario Ministry of Finance 2002). The evidence that the presence of chronic conditions in older persons can lead to progressive disability signals the need to assess policies affecting access to community rehabilitation services. Another potential complication could be the costly hospitalizations that might ensue if chronic conditions are not well managed at the earlier pathogenesis. For instance, other research has suggested that poor access results in poor self-reported health status (Landry et al. 2007), and other literature has reported that a higher utilization of costly hospital and physician services occurs when individuals self-report poor health status (Alarcon et al. 2004; Borglin et al. 2005; Frankenberg and Jones 2004; Kind et al. 2005; Lindquist and Lindquist 1999; Nelson et al. 2001; Nord et al. 2005; Reijneveld 2000; Reijneveld and Stronks 2001). Although empirical research is required to substantiate such hypotheses, it stands to reason that long wait times could drive overall healthcare costs, especially in light of the growing proportion of people reporting chronic disease.
Limitations
There are limitations to this study that affect the degree to which our data and analysis can be generalized to other settings. First, the exclusion of specialty ambulatory rehabilitation services (e.g., amputee programs and hand clinics), where PTs and OTs are employed, may underrepresent the methods used to manage wait lists in community OT and PT settings. Furthermore, this study examined wait lists and wait times only for adult rehabilitation, excluding paediatric settings, a factor that may also contribute to an underestimation of wait list management utilization. Second, although there was an acceptable response rate (57.2%) to the survey, there remains a potential for response bias. For instance, it is unclear whether the non-responders did not participate in the survey because they did not have a wait list and were therefore not interested, or alternatively, whether they did have wait lists but were reluctant to represent these data. Lastly, it would appear that there was underrepresentation from settings where OT services are provided at CHCs, OPDs and through the AREP program of the Arthritis Society, with less than a 30% response rate from these settings. This situation may be a result of fewer OT services being offered in community settings throughout Ontario; however, the potential for non-response bias should be considered in terms of underestimating the wait list management strategies utilized by this subgroup.
Conclusions
The data from our survey indicate that acuity is a primary indicator for access to publicly funded ambulatory rehabilitation service in Ontario. Moreover, the results have also highlighted that the ways in which wait lists are managed are not consistent across the continuum. Collectively, these results add further evidence that a growing number of individuals with chronic disease may increasingly encounter barriers to accessing service.
These results signal a need for stewardship within the publicly funded healthcare system to ensure that all residents have equal access to community rehabilitation services, especially in light of the forecasted increase in prevalence of chronic conditions.
Examen des stratégies de priorisation et de gestion des listes d'attente pour les services ambulatoires de réadaptation subventionnés par les fonds publics en Ontario, Canada : données additionnelles sur les obstacles d'accessibilité pour les personnes souffrant d'une maladie chronique
Résumé
Contexte : L'accès en temps opportun aux services de santé financés par les fonds publics est un enjeu prioritaire du continuum des services au Canada. L'objectif de cette étude était d'examiner les stratégies de gestion des listes d'attente pour les services ambulatoires de réadaptation financés par les fonds publics en Ontario, Canada.
Méthodologie : Nous avons défini les services ambulatoires de réadaptation en tant que services communautaires d'ergothérapie et services de physiothérapie. Nous avons envoyé un questionnaire autoadministré aux 374 établissements ontariens financés par les fonds publics. Les stratégies de gestion ont été examinées à l'aide de la statistique descriptive.
Résultats : Le taux de réponse a été de 57,2 %. Dans tous les établissements, le degré d'affection des patients est la méthode la plus fréquemment utilisée pour prioriser l'accès. La méthode la plus souvent indiquée pour la gestion des listes d'attente comprend, notamment, l'enseignement des stratégies d'autogestion (85,0%), la mise en place de politiques d'assiduité (69,5%) et le contrôle des listes d'attente (67,3%).
Conclusions : Les établissements ambulatoires de réadaptation ont mis en place un certain nombre de stratégies pour la gestion des listes d'attente. Les résultats de cette étude laissent croire qu'un nombre grandissant d'Ontariens se heurtent à des obstacles en matière d'accessibilité aux services ambulatoires de réadaptation financés par les fonds publics.
About the Author(s)
Laura A. Passalent, BSCPT, MHSC, Physiotherapist Practitioner, University Health Network, Lecturer, Department of Physical Therapy, University of Toronto, Toronto, ON
Michel D. Landry, PT, PHD, Assistant Professor, Department of Physical Therapy, University of Toronto, Toronto, ON, Adjunct Assistant Professor, Department of Health Policy and Administration,, University of North Carolina, Chapel Hill, NC
Cheryl A. Cott, PT, PHD, Deputy Director, Arthritis Community Research and Evaluation Unit, Professor, Department of Physical Therapy, University of Toronto, Toronto, ON
Correspondence may be directed to: Laura Passalent, Toronto Western Hospital, University Health Network, 3EW-400 399 Bathurst St., Toronto, ON M5T 2S8; tel.: 416-603-5800 ext. 6149; fax: 416-603-5318; e-mail: laura.passalent@uhn.on.ca.
References
Alarcon, G.S., G. McGwin Jr., A. Uribe, A.W. Friedman, J.M. Roseman, B.J. Fessler, H.M. Bastian, B.A. Baethge, L.M. Vila and J.D. Reveille. 2004. "Systemic Lupus Erythematosus in a Multiethnic Lupus Cohort (LUMINA). XVII. Predictors of Self-Reported Health-Related Quality of Life Early in the Disease Course." Arthritis and Rheumatism 51(3): 465–74.
Auditor General of Ontario. 2004. Annual Report of the Auditor General of Ontario. Retrieved April 6, 2010. <http://www.auditor.on.ca/en/reports_en/en04/307en04.pdf>.
Baranek, P.M., R.B. Deber and A.P. Williams. 2004. Almost Home: Reforming Home and Community Care in Ontario. Toronto: University of Toronto Press.
Barr, V.J., S. Robinson, B. Marin-Link, L. Underhill, A. Dotts, D. Ravensdale and S. Salivaras. 2003. "The Expanded Chronic Care Model: An Integration of Concepts and Strategies from Population Health Promotion and the Chronic Care Model." Healthcare Quarterly 7(1): 73–82.
BC Ministry of Health Services. 2004 (March). Number of People with Specific Chronic Disease by Age Group: British Columbia, 2002/2003. Retrieved April 6, 2010. <http://www.health.gov.bc.ca/cdm/research/cdm_cases_age_02-03.pdf>.
Beaglehole, R., S. Ebrahim, S. Reddy, J. Vaute and S. Leeder, on behalf of the Chronic Disease Action Group. 2007. "Prevention of Chronic Diseases: A Call to Action." Lancet 370(9605): 2152–57.
Borglin, G., U. Jakobsson, A.K. Edberg and I.R. Hallberg. 2005. "Self-Reported Health Complaints and Their Prediction of Overall and Health-Related Quality of Life among Elderly People." International Journal of Nursing Studies 42(2): 147–58.
Canadian Institute of Health Information (CIHI) National Rehabilitation Reporting System. 2005. Inpatient Rehabilitation in Canada 2003–2004. Retrieved April 6, 2010. <http://secure.cihi.ca/cihiweb/dispPage.jsp?cw_page=PG_373_E&cw_topic=373&cw_rel=AR_363_E>.
College of Physiotherapists of Ontario. 2000 (Winter). Communiqué. Retrieved July 2005. <http://www.collegept.org/college/content/pdf/en/Winter2000.pdf>.
Cott, C.A., R.M.A. Devitt, L. Falter, L.J. Soever and L.A. Passalent. 2007. "Barriers to Rehabilitation in Primary Health Care in Ontario: Funding and Wait Times for Physical Therapy Services." Physiotherapy Canada 59(3): 173–83.
DeCoster, C. 2002. "Measuring and Managing Waiting Times: What's to Be Done?" Healthcare Management Forum 15(2): 6–50.
Elwyn, G.J., L.A. Williams, S. Barry and P. Kinnersley. 1996. "Waiting List Management in General Practice: A Review of Orthopaedic Patients." British Medical Journal 312(7035): 887–88.
Esmail, N. and M. Walker. 2002. Waiting Your Turn: Hospital Waiting Lists in Canada (12th ed.). Retrieved April 6, 2010. <http://www.fraserinstitute.org/researchandpublications/publications/6240.aspx>.
Frankel, S., J. Eachus, N. Pearson, R. Greenwood, P. Chan, T.J. Peters et al. 1999. "Population Requirement for Primary Hip-Replacement Surgery: A Cross-Sectional Study." Lancet 353(9161): 1304–09.
Frankenberg, E. and N.R. Jones. 2004. "Self-Rated Health and Mortality: Does the Relationship Extend to a Low Income Setting?" Journal of Health and Social Behavior 45(4): 441–52.
Government of Ontario. 2002 (last updated 2009). Changes in Coverage for Physiotherapy Services. Retrieved April 6, 2010. <http://www.health.gov.on.ca/english/public/pub/ohip/physiotherapy.html>.
GTA Rehab Network. 2003. Measuring and Managing Supply and Demand: A Waiting List Information Management Proposal for Musculoskeletal Rehabilitation in the Greater Toronto Area. Retrieved April 6, 2010. <http://www.gtarehabnetwork.ca/downloads/rpt-waitlist-2003.pdf>.
Health Canada. 2003. Arthritis in Canada: An Ongoing Challenge. Ottawa: Author.
Juni, P., P. Dieppe, J. Donovan, T. Peters, J. Eachus, N. Pearson et al. 2003. "Population Requirement for Primary Knee Replacement Surgery: A Cross-Sectional Study." Rheumatology (Oxford) 42(4): 516–21.
Kind, P., G. Hardman and B. Leese. 2005. "Measuring Health Status: Information for Primary Care Decision Making." Health Policy 71(3): 303–13.
Landry, M.D., S.B. Jaglal, W.P. Wodchis, N.S. Cooper and C.A. Cott. 2007. "Rehabilitation Services After Total Joint Replacement in Ontario, Canada: Can ‘Prehabilitation' Programs Mediate an Increasing Demand?" International Journal of Rehabilitation Research 30(4): 297–303.
Lindquist, C.H. and C.A. Lindquist. 1999. "Health Behind Bars: Utilization and Evaluation of Medical Care among Jail Inmates." Journal of Community Health 24(4): 285–303.
Maddison, P., J. Jones, A. Breslin, C. Barton, J. Fleur, R. Lewis et al. 2004. "Improved Access and Targeting of Musculoskeletal Services in Northwest Wales: Targeted Early Access to Musculoskeletal Services (TEAMS) Programme." British Medical Journal 329(7478): 1325–27.
McDonald, P., S. Shortt, C. Sanmartin, M. Barer, S. Lewis and S. Sheps. 1998. Waiting Lists and Waiting Times for Health Care in Canada: More Management!! More Money?? Retrieved April 6, 2010. <http://www.chspr.ubc.ca/node/402>.
Meiland, F.J., J.A. Danse, J.F. Wendte, L.J. Gunning-Schepers and N.S. Klazinga. 2002. "Urgency Coding as a Dynamic Tool in Management of Waiting Lists for Psychogeriatric Nursing Home Care in the Netherlands." Health Policy 60(2): 171–84.
Murray, G., J. Gilbert and J. Wong. 2002. "Managing the Demand for Healthcare in Canada." Hospital Quarterly 6(1): 55–58.
Nelson, K., W. Cunningham, R. Andersen, G. Harrison and L. Gelberg. 2001. "Is Food Insufficiency Associated with Health Status and Health Care Utilization among Adults with Diabetes?" Journal of General Internal Medicine 16(6): 404-11.
Nord, C., A. Mykletun, L. Thorsen, T. Bjoro and S.D. Fossa. 2005. "Self-Reported Health and Use of Health Care Services in Long-Term Cancer Survivors." International Journal of Cancer 114(2): 307–16.
Ontario Ministry of Finance. 2002 (August). Update to Ontario Population Projections 2001–2028. Retrieved April 6, 2010. <http://www.ontla.on.ca/library/repository/mon/4000/10305276.pdf>.
Ontario Ministry of Health and Long-Term Care (OMHLTC). 2004. Ontario's Wait Time Strategy. Retrieved July 2005. <http://www.health.gov.on.ca/transformation/wait_times/wt_data.html>.
Ontario Ministry of Health and Long-Term Care (OMHLTC). 2006. Waiting for Health Care in Canada: What We Know and What We Don't Know. Retrieved April 6, 2010. <http://www.cihi.ca/cihiweb/dispPage.jsp?cw_page=PG_549_E&cw_topic=549&cw_rel=AR_1385_E>.
Passalent, L.A., M.D. Landry and C.A. Cott. 2009. "Wait Times for Publicly Funded Outpatient and Community Physiotherapy and Occupational Therapy Services: Implications for the Increasing Number of Persons with Chronic Conditions in Ontario, Canada." Physiotherapy Canada 61(1): 5–14.
Pattinson, J. 2003. "Primary Care. Central Reservations." Health Services Journal 113(5838): 30–31.
Perruccio, A.V., E.M. Badley and J. Guan. 2004. "Burden of Disease." In E.M. Badely and R.H. Glazier, eds., Arthritis and Related Conditions in Ontario: ICES Research Atlas (2nd ed.) (pp. 15–40). Toronto: Institute for Clinical Evaluative Sciences.
Pomey, M., P. Forest, C. Sanmartin, C. DeCoster and M. Drew. 2008 (December). Determinants of Waiting Time Management for Health Services: A Policy Review and Synthesis. Retrieved April 6, 2010. <http://www.gris.umontreal.ca/rapportpdf/R09-01.pdf>.
Randall, G.E. and A.P. Williams. 2006. "Exploring Limits to Market-Based Reform: Managed Competition and Rehabilitation Home Care Services in Ontario." Social Science and Medicine 62(7): 1594–604.
Reijneveld, S.A. 2000. "The Cross-Cultural Validity of Self-Reported Use of Health Care: A Comparison of Survey and Registration Data." Journal of Clinical Epidemiology 53(3):267-72.
Reijneveld, S.A. and K. Stronks. 2001. "The Validity of Self-Reported Use of Health Care Across Socioeconomic Strata: A Comparison of Survey and Registration Data." International Journal of Epidemiology 30(6): 1407–14.
Romanow, R. 2002. Building on Values: The Future of Health Care in Canada. Retrieved April 6, 2010. <http://www.chpca.net/public_policy_advocacy/romanow/romanow_commission.html>.
Rothman A.A. and E.H. Wagner. 2003. "Chronic Illness Management: What Is the Role of Primary Care?" Annals of Internal Medicine 138(3):256-61.
Sanmartin, C., S.E. Shortt, M.L. Barer, S. Sheps, S. Lewis and P.W. McDonald. 2000. "Waiting for Medical Services in Canada: Lots of Heat, But Little Light." Canadian Medical Association Journal 162(9): 1305–10.
Shortt, S.E. and R.A. Shaw. 2003. "Equity in Canadian Health Care: Does Socioeconomic Status Affect Waiting Times for Elective Surgery?" Canadian Medical Association Journal 168(4): 413–16.
Sullivan, T. and P.M. Baranek. 2002. First Do No Harm: Making Sense of Canadian Health Care Reform. Vancouver: UBC Press.
Trypuc, J., A. Hudson and H. MacLeod. 2006. "Ontario's Wait Time Strategy: Part 1." Healthcare Quarterly 9(2): 44–51, 2.
Tsasis, P. and J. Bains. 2009. "Chronic Disease: Shifting the Focus of Healthcare in Canada." Healthcare Quarterly 12(2): 1–11.
Wagner, E.H. 1998 (August/September). "Chronic Disease Management: What Will It Take to Improve Care for Chronic Illness?" Effective Clinical Practice 1(1): 2–4.
Wagner, E.H. and T. Groves. 2002. "Care for Chronic Disease." British Medical Journal 325: 913–14.
Wait Time Alliance. 2005. No More Time to Wait: Toward Benchmarks and Best Practices in Wait Time Management. Retrieved April 6, 2010. <http://www.eyesite.ca/pdf/no_more_time_to_wait.pdf>.
Western Canadian Waiting List Project. 2001 (March 31). From Chaos to Order: Making Sense of Waiting Lists in Canada – Final Report. Retrieved April 6, 2010. <http://www.wcwl.org/media/pdf/library/final_reports.2.pdf>.
Wright, C. and E. Ritson. 2001. "An Investigation into Occupational Therapy Referral Priorities within Kensington and Chelsea Social Services." British Journal of Occupational Therapy 64(8): 393–97.
Young, J. and S. Turnock. 2001. "Community Care Waiting Lists and Older People." British Medical Journal 322(7281): 254.
Footnotes
1Regarding DPCs, the Ontario Ministry of Health and Long-Term Care introduced strict eligibility criteria to access community-based, publicly funded physiotherapy provided in the network of DPCs across the province in 2005. Prior to this, there were no criteria and all residents were eligible for 150 visits per year. After April 2005, Ontarians were required to meet any of the following eligibility criteria: (a) under 20 years or over 64 years of age; (b) resident of a long-term care facility; (c) clients who require home PT services after hospitalization; and (d) individuals who qualify for Family Benefits, Ontario Works or the Ontario Disability Support Program (Government of Ontario 2002, last updated 2009).
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed