
World Health & Population
Engaging Informal Providers in TB control: What Is the Potential in the Implementation of the WHO Stop TB Strategy? A Discussion Paper
Abstract
The World Health Organization (WHO) Stop TB Strategy calls for involvement of all healthcare providers in tuberculosis (TB) control. There is evidence that many people with TB seek care from informal providers before or after diagnosis, but very little has been done to engage these informal providers. Their involvement is often discussed with regard to DOTS (directly observed treatment – short course), rather than to the implementation of the comprehensive Stop TB Strategy.
This paper discusses the potential contribution of informal providers to all components of the WHO Stop TB Strategy, including DOTS, programmatic management of multi-drug-resistant TB (MDR-TB), TB/HIV collaborative activities, health systems strengthening, engaging people with TB and their communities, and enabling research.
The conclusion is that with increased stewardship by the national TB program (NTP), informal providers might contribute to implementation of the Stop TB Strategy. NTPs need practical guidelines to set up and scale up initiatives, including tools to assess the implications of these initiatives on complex dimensions like health systems strengthening.
Introduction
Formal and Informal Providers in Healthcare
Globally, people resort to an array of health providers – public, private, qualified and non-qualified – as well as to self-medication to respond to their healthcare needs. Many factors, including the perceived nature and severity of the disease, geographical accessibility, financial constraints, providers' attitudes, cultural sensitiveness, and so forth, determine people's choices among different types of healthcare providers.
The World Health Organization (WHO) recommends that all available healthcare providers be involved in tuberculosis (TB) control. Generic public–private mix approaches (PPM) have been developed to provide TB control programs with recommendations on how to engage all relevant providers outside the network of the national TB control program (such as public institutions outside of ministries of health, businesses, individual private medical practitioners, practitioners of traditional medicine, etc.). These non-state providers can be purposefully divided into formal and informal ones (Travis and Cassels 2006). Figure 1 provides an overview of the different types of formal and informal private providers.
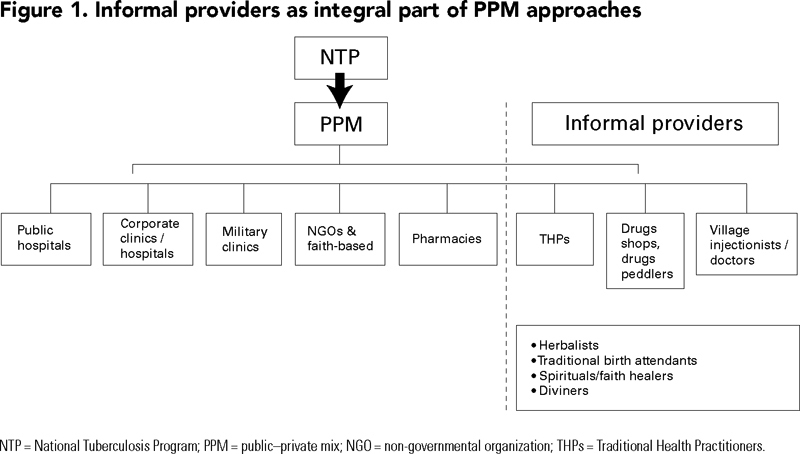
Informal providers are defined here as individuals working independently (not accountable to any institution or organization), providing health-related services in a context not formally structured or clearly regulated (e.g., practitioners of traditional medicine in African countries); or practitioners not fully qualified to provide the type of services they offer (e.g., non-qualified providers, village doctors, drug shops, village injectionists, etc.) (Figure 1). The line between formal and informal practice might be blurred at times. It is in reality the characteristics of the practice that determine whether it is formal or informal, rather than the practitioner per se. For instance, while a pharmacy registered as operating under supervision of a qualified health worker – even if in reality the services are provided by under-qualified staff, is part of the formal sector, small shops selling similar drugs alongside foodstuffs or ambulant drug sellers moving from one market to another with a stock of drugs are regarded as informal providers. Moreover, "informal" does not necessarily mean illegal. A country's healthcare regulations may well allow informal providers to practise in a number of ways, while restricting a number of functions, such as prescribing certain drugs, to formally certified practitioners. It is also common to find practitioners involved in both formal and informal practice. In such a case, from our standpoint, a qualified health worker who, besides his or her formal work in the public or private health sector, practises traditional medicine is seen as informal provider when performing those services.
The Use of Informal Providers by TB patients
The contribution of informal providers in healthcare is not well documented, yet there are indications that significant proportions of people with different ailments seek care from informal providers. Use of informal sources of care is substantial among TB patients prior to TB diagnosis. Several studies found that informal care providers were the first choice of many TB patients. The proportion of reported use of traditional medicine ranged between 10% of TB patients in a rural district in South Africa (Wilkinson et al. 1999) to 85% of hospitalized children in Ethiopia, of whom 34% had TB (Schneider et al. 1989). In Malawi, between 30% and 40% of TB patients reported having been to traditional healers (THs) prior to seeking medical care (Salaniponi et al. 2000). Another study from South Africa found that 58% of the interviewed TB patients had sought care from THs before coming to hospital (Barker et al. 2006). The use of drug shops by TB patients was reported as 30% in Malawi (Salaniponi et al. 2000) and 40% in Uganda (Kiwuwa et al. 2005). Informal providers might be seeing even higher proportions of people with TB, since the figures above relate only to people with TB who end up coming into contact with National Tuberculosis Control Programs (NTPs) or their partners. Little is known about healthcare seeking of people infected with TB who remain undiagnosed, or who are diagnosed outside the public network of TB care and whose case is not reported to the NTP.
The WHO Stop TB Strategy: Where Do Informal Providers Fit?
Within the framework of the Millennium Development Goals (MDGs), the WHO and the Stop TB Partnership developed a plan targeted to detect and treat at least 70% of sputum smear-positive TB cases, with at least 85% of those cured by 2005; to reduce the global TB burden by 50% by 2015 relative to 1990 levels; and to bring the global incidence of active TB to less than one case per one million population per year by 2050 (Stop TB Partnership 2006).
To achieve these targets, the WHO launched the Stop TB Strategy, which is broader than the implementation of directly observed treatment – short course (DOTS) alone. The strategy comprises the following components:
- Pursuing DOTS expansion and enhancement
- Addressing TB/HIV, MDR-TB (multi-drug-resistant TB) and other challenges
- Contributing to health systems strengthening
- Engaging all healthcare providers
- Empowering people with TB, and communities
- Enabling and promoting research
There is an increasing consensus about the importance of NTPs' nurturing initiatives that systematically link all available healthcare providers and actors, including informal providers, in TB prevention and care. Most of the discussion on involving all healthcare providers has so far concentrated on improving collaboration among public sector providers, the formal segments of the private sector, and the corporate and non-governmental providers (Lönnroth et al. 2004). However, "all" providers implies more than qualified practitioners, or practitioners of Western medicine. The call for all providers' involvement is equally relevant for informal providers.
The potential contribution of informal providers to TB control is largely undocumented and unexplored. The few published studies on this topic have concentrated on DOTS-related aspects: identification and referral of TB suspects, treatment supervision and preventive work. This paper proposes to take the discussion further, that is, on the potential contribution (opportunities, challenges and risks) of informal providers' with regard to implementing all components of the WHO Stop TB Strategy. In other words, the paper examines what the role of informal providers might be with regard the above-mentioned components of this strategy.
Expansion and Enhancement of High-Quality DOTS
Case Detection and Treatment Supervision
Case detection is concerned with both the number of TB cases detected (as many cases as possible) and the timeliness of the detection (early enough). A literature review showed that delays from the onset of symptoms to the first contact with a DOTS centre are highly variable, between 4 and 12 weeks (Thomas 2002). Shortening diagnostic delays (both patient and health systems delays) is an important issue in case detection. A relationship has been found between resorting first to informal providers (traditional health practitioners [THPs], drug shops, etc.) and longer delays to seek formal care, resulting in adverse treatment outcomes (Barker et al. 2006; Mesfin et al. 2009). Establishing mechanisms for timely referral from informal providers might thus impact positively on detection rates.
Supervision of DOTS by THPs was found to be at least as good as that performed by clinicians and community members (Colvin et al. 2003). However, similar studies are rare and thus pilot interventions are needed to understand the mechanisms, incentives and enablers for using THPs as DOTS supervisors. One compelling and unique example is the involvement of village doctors in DOTS implementation in Bangladesh: 11% of all TB cases detected in the areas concerned were referred by village doctors, who provided between 20% and 45% of directly observed treatment, with a treatment success rate of 90% throughout the period from 1998 to 2003 (Hamid Salim et al. 2006).
Addressing TB/HIV, MDR-TB and Other Challenges
Addressing Misconceptions (and Enhancing Prevention)
Issues of common interest in TB and HIV include the persistent claims of TB and HIV cure among informal providers. Such claims represent a matter needing serious scrutiny. Peltzer and colleagues found that 21% of THPs believed there was a cure for AIDS (Peltzer et al. 2006), just as another study from Malawi reported on THPs claiming to cure TB with traditional remedies (Banerjee et al. 2000). This is consistent with widespread perceptions in some communities that TB (like HIV) is a result of magic, a curse, or punishment from God (Edginton et al. 2002). Such messages might slow uptake of vital services such as voluntary counselling and testing for HIV as well as TB screening. For informal providers to serve as an entry point to TB/HIV screening (rather than a delaying "station"), mutual understanding and functioning referral channels to both TB and HIV screening centres (and between them) are required.
Engaging community injectionists in TB might benefit HIV prevention. One study from Uganda reported of extensive use of injections in the informal sector, which raised serious concerns with regard to transmission of HIV. Only a few of these neighbourhoods' "needle men" had been trained to perform the procedure in question (Birungi 1998). This also applies to some traditional practices that put THPs and/or patients at risk of HIV infection. Collaborative frameworks providing training and information opportunities might be ideal arenas in which to address such problems.
Enhancing Adherence: Preventing Drug Resistance Development and Amplification
As far as adherence is concerned, studies from industrialized countries show that use of alternative and complementary therapies is associated with HIV patients not taking antiretroviral (ART) medication, not adhering to the regimen or not regarding ART as beneficial (Owen-Smith et al. 2007). In the African setting, it has been argued that any conflict between traditional and Western medicine will be detrimental to adherence for both TB and HIV patients, as well as co-infected ones. Fear has recently been expressed over patients defaulting from ART programs for herbal remedies (Ahmad 2007).
Mills and colleagues found that use of some African herbal remedies would affect ART metabolism, increasing risk of drug failure and toxicity in the case of parallel use (Mills et al. 2005). No data exist on the extent of simultaneous use of informal and formal care by TB patients under DOTS, although such practices are likely to be recurrent. Involvement of informal providers would contribute to reducing the frequency of parallel use of medications and therefore mitigate the risks of interactions, adverse effects and drug failure in TB/HIV co-infected patients.
As to strengthening management of MDR-TB and prevention of extensively drug-resistant TB (XDR), available (unpublished) data from the WHO show that in Bangladesh engaging the over 10,000 village doctors (informal providers) is contributing to diagnosis and treatment of patients with resistant TB. Village doctors act as MDR field supervisors; they visit the patients at least four times during the ambulatory treatment phase (after the intensive phase in hospital). Their role in MDR management is to provide DOT, help identify and counsel patients about side effects, and help ensure that follow-up tests and clinical checkups are done on schedule. Currently, village doctors provide 90% of ambulatory care for MDR-TB patients, with remarkably high treatment outcomes: 89% cure rate, 5% death rate and 1% failure (Lönnroth 2009).
Opportunities for Collaborative TB/HIV Activities
Any involvement of informal providers in TB control will benefit HIV control efforts and vice versa. The HIV control arena has been more active than TB control in attempting to engage informal providers, yet such initiatives have largely been on a limited scale (UNAIDS 2002). Given TB/HIV co-morbidity, substantial proportions of TB patients in high HIV prevalence settings are in need of palliative care. In this respect, strengthened collaboration with informal providers would contribute to provision of palliative care, including the psychosocial support that most AIDS/TB patients need in later stages of the diseases (Kang'ethe 2009).
Health Systems Strengthening
Health systems strengthening is increasingly recognized as a cross-cutting and strategic issue in all WHO work. The WHO's framework for action defines a health system as "all organizations, people and actions whose primary intent is to promote, restore or maintain health" (WHO 2000: 5). Regarding the content of a health system, The World Health Report 2000 stated in explicit terms that "formal health services, including the professional delivery of personal medical attention, are clearly within these boundaries. So are actions by traditional healers, and all use of medication, whether prescribed by a provider or not" (WHO 2000: 5). According to this definition, informal providers are an integral part of health systems (Travis and Cassels 2006). Any attempt to strengthen relationships between providers in the public, private (including non-governmental organizations) and other informal sectors constitutes health systems strengthening actions.
It is essential, but also challenging, to demonstrate that increased involvement of informal providers in TB care is beneficial to the whole health system's structure, that is, to the six blocks building a health system. These building blocks are (1) delivery of health services, (2) human resources for health, (3) health information systems, (4) medical products and technologies, (5) health financing (collecting, pooling and purchasing) and (6) stewardship (WHO 2006: 3).
Delivery of Health Services
There are indications that significant numbers of TB patients seek care from informal providers. Building formal relationships between these providers and NTPs would potentially improve access to and uptake of standardized and quality-assured TB care and other medical conditions. Indications for increased service delivery might include referral of patients from informal providers to TB screening centres, more TB patients receiving supervision from informal providers, more patients co-infected with TB/HIV getting palliative care or counselling from informal providers, and so forth. Thinking from a systems perspective, one would also argue that informal providers involved in TB care should be prepared and empowered to assist in other aspects of health services, such as maternal and child health.
|
Challenges and suggestions for solutions on engaging informal providers Identification of genuine informal providers. It is generally believed that an important proportion of informal providers are less than genuine, and that they deceive patients and put their lives at risk. Lack of a professional organization with capacity for selfregulation and control contributes to difficulty of controlling these providers. Qualification/literacy of informal providers. Low literacy levels are another challenge to programs targeting informal providers. As a rule, providers' experience with caregiving, recognition by the community and willingness to get involved in TB control should be taken as criteria for qualification of informal providers. Low literacy should not be an exclusion criterion. It should be up to program managers to design strategies that respond to the needs of less-educated informal providers. Quality assurance of services provided by informal providers. This is a consequence of the previous two challenges. Care should be taken so that involvement of informal providers is not used as validation of other, non-evidence based, practices they may be involved in. Antagonisms/lack of trust between informal providers and formally trained medical and paramedical personnel. Medical and paramedical personnel are often accused of looking down on informal providers (mainly traditional healers) and of scolding patients who disclose their visits to informal providers. Strategies to address this antagonism and to empower informal providers and patients should be put in place by programs seeking to engage these providers. Capacity of NTPs to coordinate this new and large group of providers. National Tuberculosis Programs will need strengthened capacity to oversee this process. First of all, a shift in attitudes, implying more openness, is required. Promotion of a sector-wide perspective. Gains and challenges in relation to involving informal providers in TB care needs to be assessed and addressed within the perspective of health systems, rather than in vertical terms. |
Health Workforce
In line with the WHO's definition of health workers as "all people engaged in actions whose primary intent is to enhance health," (WHO 2006: 16) informal providers are an integral part of a country's health workforce. Many low-income countries experience shortages of personnel, a skills-mix imbalance, a weak knowledge base and so forth. Thus, positive engagement of informal providers in TB control strengthens the overall health system. In line with current debates on task shifting, a well-designed delegation of tasks between formal and informal providers could help achieve a lot. Task-shifting schemes would allow medical and other qualified clinicians to concentrate on the most complicated tasks. This should be a result of careful task analysis and well-developed task distribution. In addition to task distribution, involving informal providers in TB control raises its own range of challenges that require consideration; these include identification of genuine providers, the structure of their professional organization (if any) and the quality assurance of the services they provide (see Box 1).
Health Financing
Improvements in financing include better mobilization of financial resources from national budgets, health insurance, out-of-pocket expenditures and external sources. NTPs have prime responsibility for this function of resource mobilization, as well as to ensure services are provided at the most affordable price, preferably at no charge. Clear agreements are needed between NTPs and informal providers to ensure TB patients are not charged unnecessarily by informal providers. NTPs' alignment with other disease control programs and with the basic primary care system is an essential component in the financing element. Mobilizing resources to finance incentives schemes and compensation for specific tasks for informal providers – sustaining their involvement in delivering TB services free of charge – are just a few ways of financing health services.
Health Information Systems
Bringing informal providers onboard would be of little use unless the initiative contributes to production, analysis and dissemination of information on people's health, use of services and the impact of informal providers in health improvements. It is important to ensure that informal providers' involvement will contribute to better production and circulation of health information feeding into decision-making. This presupposes informal providers' capacity to handle records as well as collect the information and processes it.
Stewardship
Informal provider involvement in TB control, as well as in other public health interventions, requires sufficient governmental structures for regulation, coordination and quality control of all aspects of healthcare provision. The need for strong stewardship for informal providers is perhaps even more critical than for formal private providers. Informal providers do not belong to structured professional bodies providing self-regulation, sanctioning malpractice, and so forth, as compared to formal health professionals whose practice is always guided by their specific professional bodies. National guidelines should therefore clarify the process of engaging informal providers in a way that reinforces national health authorities' oversight. Weak stewardship will mean opening the way for widespread malpractice, resulting in risk to patient safety. Examples of issues that need consideration in the context of strong stewardship are summarized in the Box 1.
Empowering TB Patients and Communities
Approaches to strengthen the position of patients who use private providers' services include direct consumer information on procedures, information about prices and strong social marketing (Mills et al. 2002). It was from this perspective that the WHO developed guidelines on consumer information for safe and effective use of traditional medicine (WHO 2004).
Patients' associations can play critical roles in empowering their members. In recent years, associations bringing former TB patients together have increasingly been visible at the country and global levels. However, the impact of these associations is not yet sufficiently documented to advance achievement of the Stop TB Strategy. Within the TB/HIV collaborative framework, associations of people living with HIV/AIDS (PLWA) will be useful to TB patients, since many PLWAs eventually develop TB. More documentation of experiences in countries is needed in this respect, too.
Empowerment of TB patients is directly relevant to equity in access to TB care. Gender differences have been mentioned in relation to TB care seeking. For instance, women are more likely to use informal providers' services (traditional healers) than men are (Needham et al. 2001). Women also tend to experience longer health-seeking delays, both in Asia (Yamasaki-Nakagawa et al. 2001) and Africa (Mesfin et al. 2009). It has also been shown that resorting to informal providers might be a way of concealing one's disease because of stigma associated with it (Izugbara and Afangideh 2005). Proper engagement of informal providers may therefore improve equity of access to early diagnosis and treatment, and may mitigate TB-related social stigma.
Enable and Promote Research
Operational research is needed in many aspects of informal provider involvement, including its processes and its outcomes, measured by cases referred and detected, supervised and cured; costs implied; and other aspects of health systems strengthening. Also, continued efforts in basic biological research are needed in the fight against TB. Some plants used in traditional medicine in Mexico have been shown to have effect against MDR-TB (Camacho-Corona Mdel et al. 2008). A study from rural Tanzania reported on seven different plants used by THPs to treat AIDS-related opportunistic infections, including TB (Kisangau et al. 2007). In engaging informal providers, one should consider options of promoting investigations of these therapies whenever possible.
Conclusion
Engaging informal providers seems relevant to several aspects of the implementation of the WHO Stop TB Strategy. However, this involvement requires commitment and strong stewardship. Practical guidelines are needed to help NTPs initiate and manage such initiatives that might have enormous sector-wide impact, beyond TB control. Also, tools to help assess the implications of this involvement for health systems strengthening, for instance, are called for.
Disclaimer
MU and KL are staff members of the World Health Organization. The authors alone are responsible for the views expressed in this publication and they do not necessarily represent the decisions or policies of the World Health Organization.
About the Author(s)
Berthollet Bwira Kaboru, PhD, Researcher, Division of Global Health (IHCAR), Department of Public Health Sciences, Karolinska Institutet, Stockholm, Sweden
Mukund Uplekar, MD, Medical Officer, TB Strategy and Health Systems (TBS), Stop TB Department (STB), WHO, Geneva, Switzerland
Knut Lönnroth, MD, PhD, Medical Officer, TB Strategy and Health Systems (TBS), Stop TB Department (STB), WHO, Geneva, Switzerland
Correspondence may be directed to: Berthollet Bwira Kaboru, PhD, Researcher, Division of Global Health (IHCAR), Department of Public Health Sciences, Karolinska Institutet, SE-171 77 Stockholm, Sweden; E-mail: Bwira.Kaboru@ki.se.
References
Ahmad, K. 2007. "Antiretroviral Therapy Abandoned for Herbal Remedies." The Lancet Infectious Diseases 7(5): 313.
Banerjee, A., A.D. Harries, T. Nyirenda and F.M. Salaniponi. 2000. "Local Perceptions of Tuberculosis in a Rural District in Malawi." The International Journal of Tuberculosis and Lung Disease 4(11): 1047–51.
Barker, R.D., F.J. Millard, J. Malatsi, L. Mkoana, T. Ngoatwana, S. Agarawal and S. de Valliere. 2006. "Traditional Healers, Treatment Delay, Performance Status and Death from TB in Rural South Africa." The International Journal of Tuberculosis and Lung Disease 10(6): 670–5.
Birungi, H. 1998. "Injections and Self-help: Risk and Trust in Ugandan Health Care." Social Science & Medicine 47(10): 1455–62.
Camacho-Corona Mdel, R., M.A. Ramirez-Cabrera, O.G. Santiago, E. Garza-Gonzalez, P. Palacios Ide and J. Luna-Herrera. 2008. "Activity against Drug-Resistant Tuberculosis Strains of Plants Used in Mexican Traditional Medicine to Treat Tuberculosis and Other Respiratory Diseases." Phytotherapy Research 22(1): 82–5.
Colvin, M., L. Gumede, K. Grimwade, D. Maher and D. Wilkinson. 2003. "Contribution of Traditional Healers to a Rural Tuberculosis Control Programme in Hlabisa, South Africa". The International Journal of Tuberculosis and Lung Disease 7(9 Suppl 1): S86–91.
Edginton, M.E., C.S. Sekatane and S.J. Goldstein. 2002. "Patients' Beliefs: Do They Affect Tuberculosis Control? A Study in a Rural District of South Africa." The International Journal of Tuberculosis and Lung Disease 6(12): 1075–82.
Hamid Salim, M.A., M. Uplekar, P. Daru, M. Aung, E. Declercq and K. Lönnroth. 2006. "Turning Liabilities into Resources: Informal Village Doctors and Tuberculosis Control in Bangladesh." Bulletin of the World Health Organization 84(6): 479–84.
Izugbara, C.O. and A.I. Afangideh. 2005. "Urban Women's Use of Rural-Based Health Care Services: The Case of Igbo Women in Aba City, Nigeria." Journal of Urban Health 82(1): 111–21.
Kange'ethe, S.M. 2009. "Traditional Healers as Caregivers to HIV/AIDS Clients and Other Terminally Challenged Persons in Kanye Community Home-Based Care Programme (CHBC), Botswana." Sahara 6(2): 83–91.
Kisangau, D.P., H.V. Lyaruu, K.M. Hosea and C.C. Joseph. 2007. "Use of Traditional Medicines in the Management of HIV/AIDS Opportunistic Infections in Tanzania: A Case in the Bukoba Rural District. Journal of Ethnobiology and Ethnomedicine 3: 29.
Kiwuwa, M.S., K. Charles and M.K. Harriet. 2005. "Patient and Health Service Delay in Pulmonary Tuberculosis Patients Attending a Referral Hospital: A Cross-Sectional Study." BMC Public Health 5: 122.
Lönnroth, K. 2009. PPM for MDR Prevention and Management in Bangladesh. Unpublished report. Geneva: WHO Stop TB Department.
Lönnroth, K., M. Uplekar, V.K. Arora, S. Juvekar, N.T. Lan, D. Mwaniki and V. Pathania. 2004. "Public-Private Mix for DOTS Implementation: What Makes It Work?" Bulletin of the World Health Organization 82(8): 580–6.
Mesfin, M.M., J.N. Newell, J.D. Walley, A. Gessessew and R.J. Madeley. 2009. "Delayed Consultation among Pulmonary Tuberculosis Patients: A Cross Sectional Study of 10 DOTS Districts of Ethiopia." BMC Public Health 9: 53.
Mills, A., R. Brugha, K. Hanson and B. McPake. 2002. "What Can Be Done about the Private Health Sector in Low-Income Countries?" World Hospitals and Health Services 38(3): 24–30, 41–24.
Mills, E., B.C. Foster, R. van Heeswijk, E. Phillips, K. Wilson, B. Leonard, K.Kosuge and I. Kanfer. 2005. "Impact of African Herbal Medicines on Antiretroviral Metabolism." AIDS 19(1): 95–7.
Needham, D.M., S.D. Foster, G. Tomlinson and P. Godfrey-Faussett. 2001. "Socio-economic, Gender and Health Services Factors Affecting Diagnostic Delay for Tuberculosis Patients in Urban Zambia." Tropical Medicine & International Health 6(4): 256–9.
Owen-Smith, A., R. Diclemente and G. Wingood. 2007. "Complementary and Alternative Medicine Use Decreases Adherence to HAART in HIV-Positive Women." AIDS Care 19(5): 589–93.
Peltzer, K., N. Mngqundaniso and G. Petros. 2006. "HIV/AIDS/STI/TB Knowledge, Beliefs and Practices of Traditional Healers in KwaZulu-Natal, South Africa." AIDS Care 18(6): 608–13.
Salaniponi, F.M., A.D.Harries, H.T. Banda, C. Kang'ombe, N. Mphasa, A. Mwale, B. Upindi, T.E. Hyirenda, A. Banerjee and M.J Boeree. 2000. Care seeking behaviour and diagnostic processes in patients with smear-positive pulmonary tuberculosis in Malawi. The International Journal of Tuberculosis and Lung Disease 4(4): 327–332.
Schneider, P., E. Shewangizaw, E. Taye, T. Gebrehiwot, S. Worku, J. Oppermann, W. Leupold and T. Teka. 1989. ["Traditional medicine in Ethiopia in childhood diseases"]. Kinderarztl Prax 57(8): 393–399.
Stop TB Partnership. 2006. The Global Plan to Stop TB, 2006–2015. Geneva: World Health Organization.
Thomas, C. 2002. "A Literature Review of the Problems of Delayed Presentation for Treatment and Non-completion of Treatment for Tuberculosis in Less Developed Countries and Ways of Addressing These Problems Using Particular Implementations of the DOTS Strategy." Journal of Management in Medicine 16(4–5): 371–400.
Travis, P., and A. Cassels. 2006. "Safe in Their Hands? Engaging Private Providers in the Quest for Public Health Goals." Bulletin of the World Health Organization 84(6): 427.
UNAIDS. 2002. Ancient Remedies, New Disease: Involving Traditional Healers in Increasing Access to AIDS Care and Prevention in Eastern Africa. Geneva: UNAIDS.
World Health Organization (WHO). 2000. The World Health Report 2000. Health Systems: Improving Performance. Geneva: WHO.
World Health Organization (WHO). 2004. WHO Guidelines on Developing Information on Proper Use of Traditional, Complementary and Alternative Medicine. Geneva: WHO.
World Health Organization (WHO). 2006. World Health Report 2006: Working Together for Health. Geneva: WHO.
Wilkinson, D., L. Gcabashe and M. Lurie. 1999. "Traditional Healers as Tuberculosis Treatment Supervisors: Precedent and Potential." The International Journal of Tuberculosis and Lung Disease 3(9): 838–842.
Yamasaki-Nakagawa, M., K. Ozasa, N. Yamada, K. Osuga, A. Shimouchi, N. Ishikawa, D.S. Bam and T. Mori. 2001. "Gender Difference in Delays to Diagnosis and Health Care Seeking Behaviour in a Rural Area of Nepal. The International Journal of Tuberculosis and Lung Disease 5(1): 24–31.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed