
World Health & Population
Household Expenditures as a Measure of Socioeconomic Status among Iraqis Displaced in Jordan and Syria
James R. Cope, Shannon Doocy, Shannon Frattaroli and John McGready
Abstract
Background: Various measures are used to represent socioeconomic status (SES) in health research, including income. However, reliability of income data can be low. Household expenditures are an accepted proxy for income as a more reliable measure but have been studied little in refugee populations.
Methods: Health and SES measures from cross-sectional surveys of Iraqi refugees in Jordan and Syria were analyzed using logistic regression to assess the interchangeability of household income and expenditures.
Results: In Jordan, odds ratios in the regression models including income quartiles were frequently similar to odds ratios found in the models including expenditure quartiles, indicating interchangeability. In Syria, fewer similarities were observed.
Conclusions: This study provides some evidence that household expenditures may be used interchangeably with household income for some populations, allowing for the potential collection and use of data related to expenditures as a measure of SES, similar in importance to that of income.
Background
The 2003 conflict in Iraq resulted in a large displacement of Iraqis, with many fleeing to neighbouring countries. In 2011, an estimated 1,000,000 Iraqis were thought to be in Syria and an additional 450,000 to 500,000 in Jordan (United Nations 2010). Most Iraqis chose to settle in Jordan and Syria because of both to their proximity to Iraq and their readiness to accept the displaced population (Fagen 2007). Iraqis are the largest urban refugee population being assisted by the United Nations, and the size of the displaced population relative to the populations of Jordan and Syria is substantial (US Government Accountability Office 2009). However, this has resulted in Jordan and Syria bearing much of the burden of the displacement, which has placed significant pressures on their public sectors, costing Jordan an estimated $1.6 billion US per year and Syria an estimated $150 million per year (IRIN News 2008; Mamaux and Kaufmann 2008). While funding from the international community provides some assistance, shortfalls due to the global economic slowdown and other contributing factors are a persisting challenge (United Nations 2011). Tenuous access to medical care and the high prevalence of chronic and degenerative diseases have resulted in higher costs and increased need for secondary and tertiary care among Iraqi refugees (Mowafi and Spiegel 2008). The inability to gain legal employment, which limits income earning abilities and gradually depletes household savings, further restricts the population's ability to access medical care (Doocy et al. 2010; United Nations High Commissioner for Refugees [UNHCR] 2011a, 2011b).
Various measures are used to represent socioeconomic status (SES) in health research, including income, wealth and education, which all impact health (Adler and Ostrove 1999; Anderson and Armstead 1995; Metcalf et al. 2008). With respect to health, income is a particularly important SES measure because of its relationship to health status and access to care, including mechanisms such as paying for medical care, purchasing more nutritious foods and affecting the choice of where one lives (Kennedy et al. 1998; Robert Wood Johnson Foundation to Build a Healthier America 2009). Limited income can cause struggles with day-to-day life by restricting one's ability to access resources and adopt healthy behaviours. The need for additional research into the effects of SES on health, including a determination of the potential interchangeability of SES measures and data quality and availability, has been well documented (Adler et al. 1995; Adler and Ostrove 1999). Issues with non-reporting and reliability of income data are common, in part due to reluctance to report this information to a stranger, but also due to potential complications related to non-standard forms of income, seasonal variations and measurement issues (Lipton and Ravallion 1995). Household expenditures are an accepted alternative often used as a proxy for household income and have been shown to be a more reliable indicator (Deaton 1997; Morris et al. 2000; Xu et al. 2009). This paper examines the interchangeability of household income and expenditure data in relation to health outcomes and access to care among displaced Iraqi refugees in Jordan and Syria.
Methods
In this study we analyzed health and SES components of cross-sectional surveys conducted among Iraqi refugees in Jordan (October 2008) and Syria (March 2009) to assess a variety of health and well-being measures. Stratified cluster sample designs (120 clusters 10 households in Jordan; 80 clusters 10 households in Syria) were used to distribute the sample in proportion to Iraqi residence locations. (For a detailed explanation of the sampling methodology, see Doocy et al. 2010.) The clusters were split proportionally between the capital city and non-capital Iraqi populations, resulting in 75% and 70% of the sample in Jordan and Syria, respectively, being allocated to Amman and Damascus. Clusters were assigned to smaller administrative units using similar probability-based methods; cluster start points within each area were randomly selected, and the 10 nearest Iraqi households identified were interviewed. The primary data collection tool was a household questionnaire that was completed by oral interview with an adult household member, most often the household head and/or his or her spouse.
The questionnaire was initially developed in Jordan with input from multiple stakeholders, including UN agencies, the Government of Jordan, domestic and international organizations that provide services to Iraqis, and Iraqis with expertise in humanitarian assistance. The Jordan questionnaire was subsequently adapted for use in Syria; the final questionnaires in Jordan and Syria included many sections that were identical, although some questions differed. Questionnaires focused on general food security and living conditions, health status, access to health services and receipt of humanitarian assistance. All interviewers underwent a minimum of four days training that included basic interviewing techniques, informed consent, the survey instrument and sampling methods. Interviews averaged from 30 to 50 minutes in duration; prospective respondents were informed that participation was voluntary, and no direct benefits were associated with completion of the interview. Full names and addresses were not recorded to protect the anonymity of respondents.
The Aday and Andersen framework for the study of access to medical care served as the basis for our analysis (Aday and Anderson 1974; Urrutia-Roja and Aday 1991). Individual- and household-level demographic and socioeconomic characteristics were categorized as predisposing or enabling. Predisposing characteristics include variables such age, sex, health knowledge, household size and arrival date, whereas enabling characteristics detail the ability of persons or households to access services and include such variables as income, household expenditures, borrowing money, registration status and financial situation. Exploratory analysis was conducted to assess whether factors within the model could be used as feedback mechanisms to formulate policies in response to the needs of displaced Iraqis. An overriding goal was to discern variables that could be used to identify vulnerable urban refugees by associating characteristics of the population at risk with health conditions and access to care outcomes of interest.
Data analysis was conducted using Stata/IC 10.0 (StataCorp 2007). Logistic regression was utilized to determine associations between independent variables (predisposing and enabling characteristics) and outcome variables of interest (health conditions and access to care). Variables that showed potential association in univariate logistic regression (p < .25) were incorporated into multiple logistic regression models. Manual backwards selection was used to remove variables that were not significant (p < .05). (Variables that were not significant but appeared to affect the p-value and/or odds ratio of one or more remaining variables were controlled for and included in final models.) This process allowed for the results from each model to contain those predisposing or enabling variables associated with each outcome of interest, attempting to include all relevant variables in each model and to account for any potential confounding. Adjustments were made to account for both clustering within household clusters and clustering within individual households using appropriate methods in Stata.
Both studies were approved by the Johns Hopkins Bloomberg School of Public Health Institutional Review Board. The Ministry of Planning and International Cooperation approved the study in Jordan. In Syria, the protocol and survey instrument were reviewed and approved by a locally composed review committee that included Iraqi community leaders, physicians and humanitarian assistance professionals.
Results
The final study populations included 1200 households with 4997 individuals in Jordan and 813 households with 3684 individuals in Syria. Average household size was 4.5 persons in both Jordan and Syria, and 20% to 25% of households, respectively, were headed by a female. Educational attainment was high, with 89% to 93% of households having a member who had completed secondary schooling. In Jordan and Syria, 52% and 59% of households, respectively, reported having children, including 30% and 22%, respectively, with children less than five years of age. Large minorities of Iraqi households in Jordan (17%) and Syria (41%) lived below the international poverty line of < 2 US dollars/person/day; however, low response rates were a problem specific to income data. Population summary statistics for health conditions and access to care, the outcomes of focus of the SES analysis, are summarized in Table 1.
| Table 1. Health Conditions and Access to Medical Care Among Iraqi Refugees in Jordan and Syria | ||||
| Health Conditions | Jordan | Syria | ||
| Prevalence (95% CI) | Prevalence (95% CI) | |||
| Chronic Conditions in Adults | n = 3414 | n = 2,342 | ||
| Hypertension | 19.6% | (18.3–21.0) | 19.6% | (18.0–21.3) |
| Musculoskeletal | 18.5% | (17.2–19.9) | 16.6% | (15.1–18.2) |
| Digestive | 11.3% | (10.3–12.4) | 7.1% | (6.1–8.2) |
| Diabetes | 9.1% | (8.2–10.1) | 7.6% | (6.6–8.7) |
| Cardiovascular | 6.7% | (5.9–7.6) | 7.8% | (6.8–9.0) |
| Lung/Respiratory | 3.1% | (2.5–3.7) | 6.0% | (5.1–7.1) |
| Kidney | 1.9% | (1.5–2.4) | 2.9% | (2.3–3.7) |
| Cancer | 1.3% | (0.9–1.7) | 0.6% | (0.4–1.1) |
| Others | 13.7% | (12.6–14.9) | 29.8% | (28.0–31.7) |
| Any chronic condition | 41.0% | (39.4–42.7) | 51.5% | (49.4–53.5) |
| Disability | n = 4997 | n = 3684 | ||
| Any disability | 3.4% | (3.0–3.9%) | 7.1% | (6.3–8.0%) |
| Physical disability | 1.7% | (1.4–2.1%) | 3.0% | (2.5–3.6%) |
| Access to Medical Care | Percent | Percent | ||
| Sought care last time medical attention was needed | 85.8% | 84.4% | ||
| We are able to get medical care when necessary | 62.5% | 58.8% | ||
| We can always afford medical care | 32.4%* | 23.5%* | ||
| We have access to the medical specialists we need | 53.3%* | 40.8%* | ||
| We receive enough information to stay healthy | 55.4%* | 30.4%* | ||
| Households with a member hospitalized within past year | 30.2%* | 43.1%* | ||
|
*Statistically significant difference (p < .05) between Jordan and Syria. CI = confidence interval. |
||||
Approximately two thirds of respondents answered the income question (64% in Jordan, 66% in Syria), leaving a large proportion of respondents without income data. Expenditure data was reported at a much higher level in both countries (91% in Jordan; 96% in Syria). To test that the distribution of non-responses was random, the association between SES factors and income reporting was assessed (Table 2).
| Table 2. Comparison of socioeconomic factors and reporting of income in Jordan and Syriaa | ||||||
| Household characteristics | Jordan | Syria | ||||
| Households not reporting income (n = 430, 36%) | Households reporting income (n = 770, 64%) | p-value | Households not reporting income (n = 267, 34%) | Households reporting income (n = 533, 66%) | p-value | |
| Employment | ||||||
| Household member(s) employed | 117 (27%) | 462 (60%) | p < .01 | 47 (19%) | 217 (41%) | p < .01 |
| No employed household member | 313 (73%) | 308 (40%) | 200 (81%) | 316 (59%) | ||
| Education | ||||||
| Primary | 34 (8%) | 94 (12%) | p < .01 | 20 (8%) | 31 (6%) | p < .00 |
| Secondary | 88 (20%) | 198 (26%) | 91 (35%) | 119 (22%) | ||
| Institutional | 68 (16%) | 133 (17%) | 42 (16%) | 124 (23%) | ||
| University | 240 (56%) | 345 (45%) | 109 (41%) | 258 (49%) | ||
| Residence location | ||||||
| Lives in capital city | 339 (79%) | 561 (73%) | p = .02 | 210 (80%) | 353 (66%) | p < .00 |
| Lives outside of capital | 91 (21%) | 209 (27%) | 52 (20%) | 180 (34%) | ||
| Arrived prior to 2003 | ||||||
| Yes | 350 (81%) | 573 (77%) | p < .01 | 10 (4%) | 14 (3%) | p = .46 |
| No | 80 (19%) | 167 (23%) | 249 (96%) | 514 (97%) | ||
| Home ownership | ||||||
| Residence owned | 97 (23%) | 89 (12%) | p < .01 | 25 (9%) | 74 (12%) | p = .04 |
| Residence not owned | 333 (77%) | 681 (88%) | 242 (91%) | 457 (88%) | ||
| Registered with UNHCR | ||||||
| Yes | 328 (76%) | 599 (78%) | p = .47 | 231 (87%) | 495 (94%) | p < .00 |
| No | 102 (24%) | 168 (22%) | 36 (13%) | 32 (6%) | ||
|
a Due to missing data, some differences exist in the number of households reported compared to study totals. UNHCR = United Nations High Commissioner for Refugees. |
||||||
Households in both Jordan and Syria that reported no adult member employed were more likely to not report their income. A difference in reporting also appeared among people with different levels of education, but the pattern varied by country. In Jordan, a higher percentage of households with an adult with a university education failed to report an income, whereas in Syria, households with an adult with a primary level of education were more likely to not report an income. Similarly, results for proximity to the capital, home ownership, arrival year and UNHCR registration status were not consistent between the countries. No differences were seen with regard to respondent age, reporting a chronic disease, or access to care variables. Assuming there are no obvious confounding factors influencing the reporting of income that can be adjusted for, it stands to reason that other available indicators with more complete reporting should be used as alternative SES proxies.
Logistic regression models where income and expenditures were significantly associated with a health condition (Table 3) and access to care outcomes (Table 4) have several similarities, particularly in Jordan.
| Table 3. Comparison of income and expenditure quartile results for health condition regression models | |||||
| Jordan | Syria | ||||
| Expenditure quartiles odds ratio (95% CI) |
Income quartiles odds ratio (95% CI) |
Expenditure quartiles odds ratio (95% CI) |
Income quartiles odds ratio (95% CI) |
||
| Diabetes | 1st | Reference | Reference | Reference | Reference |
| 2nd | 0.48 (0.30–0.79) | 0.54 (0.35–0.82) | 0.85 (0.53–1.38) | 0.52 (0.29-0.93) | |
| 3rd | 0.92 (0.61–1.40) | 0.81 (0.54–1.24) | 0.91 (0.61–1.36) | 0.84 (0.53–1.37) | |
| 4th | 0.79 (0.49–1.25) | 0.73 (0.48–1.12) | 0.97 (0.61–1.55) | 0.97 (0.59–1.60) | |
| Musculoskeletal disease | 1st | Reference | Reference | Reference | Reference |
| 2nd | 0.75 (0.53–1.06) | 0.79 (0.57–1.10) | 0.60 (0.44–0.82) | 0.70 (0.50–0.97) | |
| 3rd | 0.86 (0.62–1.19) | 0.74 (0.51–1.07) | 0.60 (0.47–0.78) | 0.66 (0.43–0.99) | |
| 4th | 0.79 (0.53–1.16) | 0.52 (0.27–0.61) | 0.62 (0.46–0.84) | 0.77 (0.53–1.12) | |
| Respiratory disease | 1st | Reference | Reference | Reference | Reference |
| 2nd | 0.75 (0.43–1.33) | 0.45 (0.19–1.05) | 0.55 (0.30–1.01) | 0.58 (0.32–1.06) | |
| 3rd | 0.65 (0.36–1.19) | 0.64 (0.29–1.40) | 0.82 (0.51–1.34) | 1.04 (0.64–1.68) | |
| 4th | 0.39 (0.18–0.82) | 0.33 (0.12–0.93) | 0.78 (0.49–1.24) | 1.02 (0.67–1.57) | |
| Dialysis | 1st | Reference | Reference | Reference | Reference |
| 2nd | 0.43 (0.20–0.94) | 0.83 (0.36–1.92) | 1.12 (0.55–2.30) | 0.71 (0.29–1.70) | |
| 3rd | 0.63 (0.30–1.33) | 0.32 (0.13–0.82) | 0.59 (0.28–1.26) | 0.85 (0.39–1.86) | |
| 4th | 0.45 (0.21–1.00) | 0.24 (0.09–0.59) | 1.06 (0.59–1.91) | 0.24 (0.07–0.92) | |
| Physical disability | 1st | Reference | Reference | Reference | Reference |
| 2nd | 0.79 (0.53–1.97) | 0.61 (0.34–1.09) | 0.74 (0.45–1.20) | 0.73 (0.38–1.40) | |
| 3rd | 0.62 (0.38–0.99) | 0.38 (0.19–0.76) | 0.52 (0.31–0.87) | 0.64 (0.33–1.21) | |
| 4th | 0.43 (0.23–0.80) | 0.28 (0.14–0.57) | 0.97 (0.65–1.48) | 1.33 (0.78–2.27) | |
|
Note. Bold value indicates statistically significant results (p < .05); only predictors that showed potential association in univariate logistic regression (p < .25) were incorporated into multiple logistic regression models. UNHCR = United Nations High Commissioner for Refugees. |
|||||
| Table 4. Comparison for income and expenditure quartile results for access to care regression models | |||||
| Jordan | Syria | ||||
| Expenditure quartiles odds ratio (95% CI) |
Income quartiles odds ratio (95% CI) |
Expenditure quartiles odds ratio (95% CI) |
Income quartiles odds ratio (95% CI) |
||
| Sought care when last needed | 1st | Reference | Reference | Reference | Reference |
| 2nd | 2.13 (1.24–3.66) | 2.75 (1.42–5.35) | 0.64 (0.38–1.07) | 1.13 (0.62–2.07) | |
| 3rd | 1.95 (1.15–3.30) | 2.49 (1.35–4.57) | 1.04 (0.57–1.90) | 1.30 (0.71–2.39) | |
| 4th | 4.05 (2.02–8.10) | 2.74 (1.37–5.47) | 0.85 (0.45–1.60) | 2.80 (1.19–6.44) | |
| Not able to access care | 1st | Reference | Reference | Reference | Reference |
| 2nd | 0.86 (0.57–1.30) | 0.74 (0.49–1.12) | 3.16 (0.76–13.19) | 0.97 (0.34–2.79) | |
| 3rd | 0.60 (0.40–0.92) | 0.55 (0.33–0.90) | 0.95 (0.24–3.71) | 1.65 (0.14–19.32) | |
| 4th | 0.51 (0.31–0.82) | 0.28 (0.15–0.52) | 2.09 (0.51–8.41) | 0.74 (0.05–11.62) | |
| Not able to access health information | 1st | Reference | Reference | Reference | Reference |
| 2nd | 0.78 (0.57–1.06) | 0.79 (0.50–1.24) | 1.81 (1.04–3.15) | 1.03 (0.59–1.81) | |
| 3rd | 0.80 (0.54–1.19) | 0.73 (0.46–1.17) | 1.88 (0.98–3.60) | 1.25 (0.60–2.63) | |
| 4th | 0.54 (0.34–0.85) | 0.37 (0.23–0.61) | 2.59 (1.16–5.60) | 0.90 (0.41–2.00) | |
| Not able to access specialist care | 1st | Reference | Reference | Reference | Reference |
| 2nd | 0.89 (0.65–1.23) | 0.65 (0.40–1.04) | 0.83 (0.53–1.31) | 0.99 (0.56–1.74) | |
| 3rd | 0.60 (0.42–0.86) | 0.57 (0.35–0.94) | 0.81 (0.49–1.35) | 1.37 (0.71–2.63) | |
| 4th | 0.24 (0.15–0.39) | 0.19 (0.11–0.35) | 0.74 (0.43–1.25) | 0.65 (0.34–1.23) | |
| Hospitalized in the past year | 1st | Reference | Reference | Reference | Reference |
| 2nd | 1.71 (1.07–2.74) | 1.42 (0.89–2.28) | 0.91 (0.56–1.48) | 1.22 (0.77–1.93) | |
| 3rd | 2.01 (1.24–3.25) | 1.79 (1.13–2.84) | 0.81 (0.51–1.28) | 1.25 (0.70–1.22 | |
| 4th | 2.33 (1.46–3.72) | 1.98 (1.24–3.16) | 1.13 (0.68–1.88 | 1.43 (0.70–2.92) | |
| Note. Bold value indicates statistically significant results (p < .05); only predictors that showed potential association in univariate logistic regression (p < .25) were incorporated into multiple logistic regression models. | |||||
In many cases, the odds ratios found in the model that included income quartiles were similar in value to the odds ratios found in the model that included expenditure quartiles. For instance, in Jordan, those households in the 2nd, 3rd and 4th expenditure quartiles as well as those in the 2nd, 3rd and 4th income quartiles were significantly more likely to have sought care when last needed compared to those in the 1st quartile. Also in Jordan, those households in the 4th expenditure quartile as well as those in the 4th income quartile were significantly less likely to have reported difficulty accessing health information compared to those in the 1st quartile. In Syria, fewer similarities were observed between the income and expenditure models. This is likely attributable to weaker association between income and expenditures that was observed in Syria. In Jordan, a clear linear relationship between income and expenditures can be observed (Figure 1), whereas in Syria the relationship is less apparent (Figure 2).
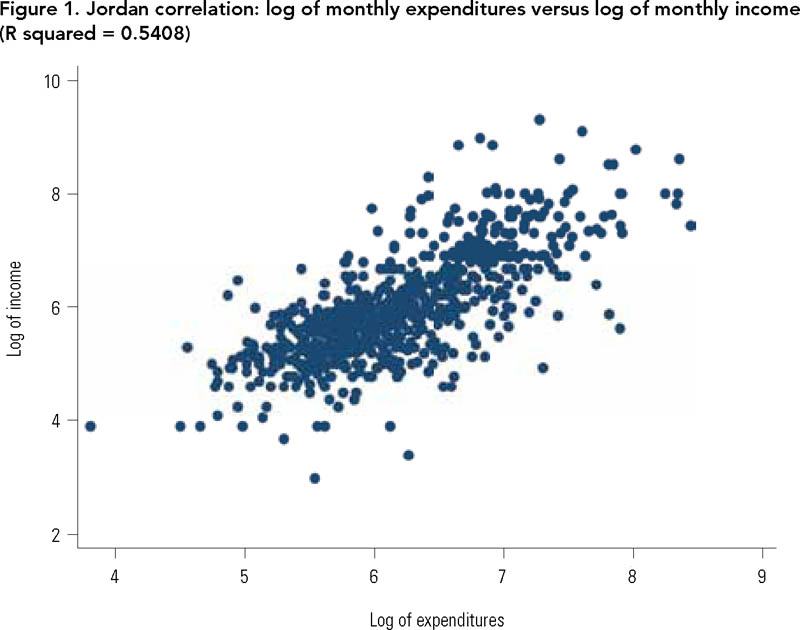
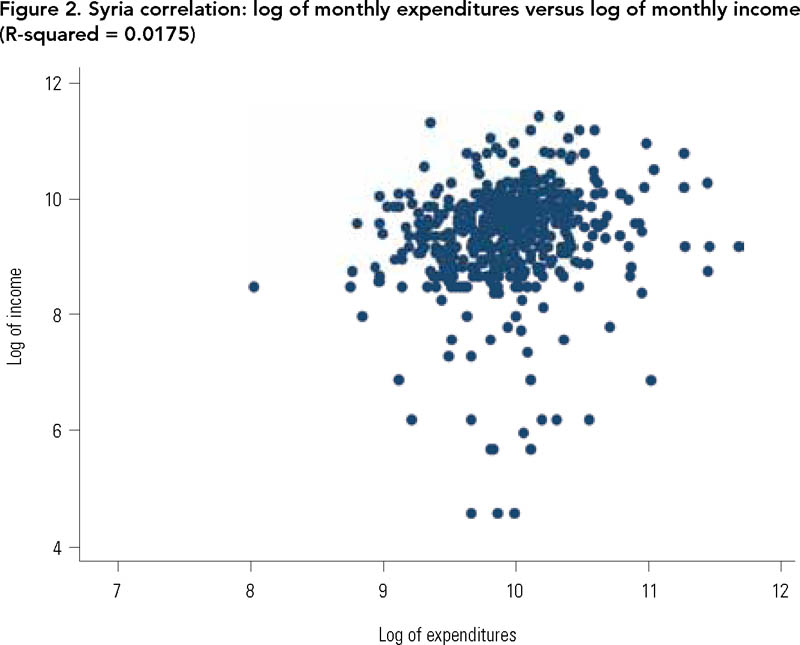
Pair-wise correlations for income and expenditure quartiles led to similar conclusions. Among households reporting both measures, the household income quartile was more likely to be the same as the household expenditure quartile in Jordan than in Syria, with pair-wise correlations of 0.69 (p < .00) and 0.20 (p < .00), respectively.
Discussion
Household income and expenditure as measures of socioeconomic status were significantly associated with multiple health conditions and access to care measures in Iraqi refugee populations in both Jordan and Syria. In many cases, lower likelihood of health conditions was observed among individuals in higher income and expenditure quartiles, compared to those in the lowest quartile. With regard to access to care, households in the higher expenditure and income quartiles generally reported less difficulty accessing care. In Jordan, households in the higher quartiles, compared to those in the lowest quartile, were less likely to have reported not being able to access care, not being able to obtain health information, not being able to access specialist care and not being able to afford care. In Syria, the results were less compelling, which could in part have to do with the difference in how Iraqis access care in the two countries. In Jordan, the private sector is more developed and serves as the primary source of care for the Iraqi population, whereas in Syria the Syrian Arab Red Crescent (SARC) is the most common primary care provider (Doocy et al. in press). Overall in Jordan, households reporting higher monthly expenditures and incomes were less likely to have someone reporting a health condition and less likely to report difficulty accessing care.
More importantly, however, these results support the assumption that household expenditures are a reasonable proxy for household income. In many cases, the results from logistic regression models that included income quartiles were similar in value to those found in the logistic models that included expenditure quartiles, thus providing evidence of the interchangeability of the two measures in the study models. The linear association between income and expenditure values and the correlation between household expenditure and income quartiles in Jordan further demonstrated similarity.
However, findings from Syria are again not as compelling, which may in part be due to measurement error. The one consistent factor between the two countries was the higher percentage of non-employed households failing to report an income. It is possible that the stigma associated with reporting income is further complicated when there is a lack of current employment. It is also possible that some respondents were reluctant to provide income information out of concern that reporting it could decrease humanitarian assistance or compromise their situation, since they are not legally able to seek employment.
Our findings support previous research and practice that have used expenditures as a proxy for income, while extending the concept to vulnerable and displaced populations, for which there are a limited number of studies available. Food security is one area where this concept has been applied. In examining food security based on national household budget surveys, the Food and Agriculture Organization (FAO) of the United Nations notes that income can be difficult to aggregate, while household expenditures as a proxy for income can be used to estimate inequalities in food consumption relative to income (FAO 2008). Quality estimates of such measures are critical to estimating the prevalence of food poverty; thus, national household surveys often use expenditures as opposed to income when estimating the prevalence of food deprivation and poverty. A report from the US Agency for International Development noted several key advantages to using expenditures as a proxy for income in measuring indicators related to food availability (Kumar 1989). Advantages included the fact that expenditure data are more reliable than income data because people are more willing to discuss expenditures; they are easier to recall and they represent actual as opposed to potential consumption. Community and household surveillance of refugee camps in Tanzania utilized household expenditures as a proxy for income, successfully demonstrating that, compared to households with higher expenditures, those with lower expenditures had proportionally higher expenditures on food (World Food Program and UNHCR 2011).
A survey of Palestinian refugees utilized household expenditure as a proxy for income to show that low expenditures among refugees equated to higher rates of poverty (Chaaban et al. 2010). Efforts in Uganda to quantify poverty routinely use expenditure as a proxy for income, which allows for the adjustment of expenditure data to ensure comparability between surveys over time and in different geographic locations (Okidi and Mugambe 2002). Similar research in Uganda has noted that this approach is favoured by economists because it reflects a household's ability to cushion its standard of living through saving and borrowing despite income fluctuations, while income data is often viewed as an unreliable measure (Mukasa and Masiga 2003). In Burundi, a study assessing the role of local institutions as determinants of income in a conflict setting used expenditures as a proxy for income, noting that it is a better measure of permanent income than current income (Voors and Bulte 2008). Finally, research on malaria in Kenya assessed the links between malaria, poverty and vulnerability at the household level, using expenditures as a proxy for income (Chuma et al. 2006).
Limitations
There are a few limitations with this study. While efforts were made to standardize the questionnaires, the adaptation process to contextualize the survey instrument to the Syrian context could have changed how questions were framed and affected the reliability of the income and expenditure data. Jordanian interviewers were used in Jordan and Iraqi interviewers were used in Syria. Interviewer nationality in conjunction with differing security situations could have led to reporting biases and differences between the two study populations, particularly since income and expenditure data are self-reported. While some time has passed since the data were collected and the political situation in Syria has changed dramatically, potentially limiting the impact of the findings, significant Iraqi populations remain in Jordan and Syria and it appears that the protracted nature of the situation will continue into the foreseeable future. Finally, there is also some concern regarding the differences between the Syria and Jordan datasets, with the significant findings being limited to Jordan. Future research is needed to help assess the generalizability of our results.
Conclusions
While the relationship between expenditures and income would be expected in general, the results from this research showed that household expenditures may be used interchangeably with household income for some populations. This would potentially allow for the collection and use of data related to expenditures as a measure of SES, similar in importance to that of income. A stigma can be associated with the reporting of income, and there can be potential reluctance by some to provide a response based on the specific situation, as possibly shown by the relatively low response rate in the data. This can be particularly important in refugee populations where there are real and perceived consequences of providing household income information, including both legal status and qualifying for humanitarian assistance. Future research is needed to validate these findings, in particular in light of the results from Jordan compared to those from Syria. Income is an important measure of SES, so demonstrating the potential interchangeability of income with another, less stigmatized measure of SES is of value, particularly in refugee, hidden and marginalized populations who may not be legally able to seek employment and generate income. By demonstrating such potential, it may be possible to enhance the understanding of SES and its impact on health, and improve policy recommendations for vulnerable populations such as refugees.
About the Author(s)
James R. Cope, PhD, MPH, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD
Shannon Doocy, PhD, Assistant Professor, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD
Shannon Frattaroli, PhD, MPH, Assistant Professor, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD
John McGready, PhD, MS, Assistant Scientist, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD
Correspondence may be directed to: James Cope, e-mail: jrcope9@gmail.com
Acknowledgment
Dissertation Committee Chair: Gil Burnham, MD, PhD, MS, Professor, Johns Hopkins Bloomberg School of Public Health
Dissertation Committee Member and Primary Investigator: Doug Storey, PhD, MA, Assistant Professor, Johns Hopkins Bloomberg School of Public Health
References
Aday, L. and A.M. Andersen. 1974. "A Framework for the Study of Access to Medical Care." Health Services Research 9(3): 208–20.
Adler, N.E., T. Boyce, M.A. Chesney, S. Cohen, S. Folkman, R.L. Kahn and S.L. Syme. 1995. "Socioeconomic Status and Health: The Challenge of the Gradient." American Psychology 49(1): 15–24.
Adler, N.E. and A.M Ostrove. 1999. "Socioeconomic Status and Health: What We Know and What We Don't." Annals of the New York Academy of Sciences 896: 3–15.
Anderson, N.B. and C.A. Armstead. 1995. "Toward Understanding the Association of Socioeconomic Status and Health: A New Challenge for the Biopsychosocial Approach." Psychosomatic Medicine 57(3): 213–25.
Chaaban, J., H. Ghattas, R.R. Habib, S. Hanafi, N. Sahyoun, N. Salti et al. 2010. Socio-Economic Survey of Palestinian Refugees in Lebanon. Retrieved February 16, 2012. <http://www.unrwa.org/userfiles/2011012074253.pdf>.
Chuma, J.M., M. Thiede and C.S. Molyneux. 2006. "Rethinking the Economic Costs of Malaria at the Household Level: Evidence from Applying a New Analytical Framework in Rural Kenya." Malaria Journal 5: 76.
Deaton, A. 1997. The Analysis of Household Surveys: A Microeconometric Approach to Development Policy. Baltimore, MD: Johns Hopkins University Press.
Doocy, S., A. Sirois, J. Anderson, M. Tileva, E. Biermann, J.D. Storey and G. Burnham. 2010. "Food Security and Humanitarian Assistance among Displaced Iraqi Populations in Jordan and Syria." Social Science & Medicine 72(2): 273–82.
Doocy, S., A. Sirois, M. Tileva, J.D. Sotrey and G. Burnham. In press. "Chronic Disease and Disability among Iraqi Populations Displaced in Jordan and Syria." International Journal of Health Planning and Management.
Fagen, P.W. 2007. Iraqi Refugees: Seeking Stability in Syria and Jordan. Retrieved on March 12, 2012. <http://isim.georgetown.edu/publications/20071231_Iraqi_Refugees.pdf>.
Food and Agriculture Organization of the United Nations. 2008. Deriving Food Security Information from National Household Budget Surveys. Experiences, Achievements, Challenges. Accessed February 16, 2012. <http://www.fao.org/docrep/011/i0430e/i0430e00.htm>.
IRIN News. 2008, July 16. "Jordan: Government Stops Issuing Residency Permits for Iraqis." Retrieved March 12, 2012. <http://www.irinnews.org/Report/79276/JORDAN-Government-stops-issuing-residency-permits-to-Iraqis>.
Kennedy, B.P., I. Kawachi, R. Glass and D. Prothrow-Stith. 1998. "Income Distribution, Socioeconomic Status, and Self Rated Health in the United States: Multilevel Analysis." BMJ 317(7163): 917–21.
Kumar, K. 1989. Indicators for Measuring Changes in Income, Food Availability and Consumption, and the Natural Resource Base. A.I.D. Program Design and Evaluation No. 12 (Document Order No. PN-AAX-223) U.S. Agency for International Development. Retrieved February 16, 2012. <http://pdf.usaid.gov/pdf_docs/PNAAX223.pdf>.
Lipton, M. and M. Ravallion. 1995. "Poverty and Policy." In H. Chenery and T.N. Srinivasan, eds., Handbook of Development Economics pp. 2551-657. Elsevier.
Mamaux, L. and M. Kaufmann. 2008. Iraqi Refugees: A Humanitarian Surge Is Needed for an Invisible Humanitarian Crisis. The US Helsinki Commission. Retrieved March 12, 2012. <http://www.csce.gov/index.cfm?FuseAction=ContentRecords.ViewDetail&ContentRecord_id=146&Region_id=163&Issue_id=0&ContentType=G&ContentRecordType=G&CFID=6362336&CFTOKEN=71125241>.
Metcalf, P.A., R.R. Scragg, D. Schaaf, L. Dyall, P.N. Black and R.T. Jackson. 2008. "Comparison of Different Markers of Socioeconomic Status with Cardiovascular Disease and Diabetes Risk Factors in the Diabetes, Heart and Health Survey." The New Zealand Medical Journal 121(1269): 45–56.
Morris, S.S., C. Carletto, J. Hoddinott and L.J. Christiaensen. 2000. "Validity of Rapid Estimates of Household Wealth and Income for Health Surveys in Rural Africa." Journal of Epidemiology and Community Health 54(5): 381–7.
Mowafi, H. and P. Spiegel. 2008. "The Iraqi Refugee Crisis: Familiar Problems and New Challenges." JAMA: The Journal of the American Medical Association 299(14): 1713–5.
Mukasa, E. and S. Masiga. 2003. Regional Workshop on Ageing and Poverty. Uganda Country Position Paper. Retrieved February 16, 2012. <http://www.un.org/ageing/documents/workshops/Tanzania/uganda.pdf>.
Okidi, JA and G.K. Mugambe. 2002. An Overview of Chronic Poverty and Development Policy in Uganda. Retrieved February 12, 2012. <http://www.dfid.gov.uk/r4d/PDF/Outputs/ChronicPoverty_RC/11OkidiMugambe.pdf>.
Robert Wood Johnson Foundation to Build a Healthier America. 2009. Reaching America's Health Potential: A State-by-State Look at Adult Health. Retrieved March 12, 2012. <http://www.commissiononhealth.org/Documents/AdultHealthChartbookFullReport.pdf>.
StataCorp. 2007. Stata Statistical Software: Release 10. College Station, TX: StataCorp LP.
United Nations. 2010. UNHCR Global Appeal 2010–2011 Update. Retrieved March 21, 2012. <http://www.unhcr.org/ga11/#/home>.
United Nations. 2011. "UNHCR Faces Funding Shortfall for Iraq Operation." Retrieved March 12, 2012. <http://www.un.org.sy/forms/stories/viewStories.php?id=4>.
United Nations High Commissioner for Refugees (UNHCR). 2012. "2012 UNHCR Country Operations Profile – Jordan." Retrieved March 12, 2012. <http://www.unhcr.org/pages/49e486566.html>.
UNHCR. 2012. "2012 UNHCR Country Operations Profile – Syrian Arab Republic." Retrieved March 12, 2012. <http://www.unhcr.org/pages/49e486a76.html>.
Urrutia-Roja, X. and L. Aday. 1991. "A Framework for Community Assessment: Designing and Conducting a Survey in a Hispanic Immigrant and Refugee Community." Public Health Nursing 8(1): 20–6.
US Government Accountability Office. 2009. Iraqi Refugee Assistance: Improvements Needed in Measuring Progress, Assessing Needs, Tracking Funds, and Developing an International Strategic Plan. Retrieved March 12, 2012. <http://www.gao.gov/products/GAO-09-120>.
Voors, M.J. and E.H. Bulte. 2008. Unbundling Institutions at the Local Level: Conflict, Institutions and Income in Burundi Households in Conflict Network (HiCN). Retrieved February 16, 2012. <http://www.humansecuritygateway.com/documents/HICN_UnbundlingInstitutionsLocalLevel_Burundi.pdf>.
World Food Program and UNHCR. 2011. "Community and Household Surveillance in North Western Tanzania: Programme Outcome Monitoring in Nyarugusu Refugee Camp." Retrieved February 16, 2012. <http://www.wfp.org/content/tanzania-community-and-household-surveillance-north-western-june-2011>.
Xu, K, F. Ravndalb, D.B Evansa and G. Carrina. 2009. "Assessing the Reliability of Household Expenditure Data: Results of the World Health Survey." Health Policy 91(3): 297–305.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed