
Nursing Leadership
Continuous Quality Improvement: A Shared Governance Model That Maximizes Agent-Specific Knowledge
Abstract
Motivate, Innovate, Celebrate: an innovative shared governance model through the establishment of continuous quality improvement (CQI) councils was implemented across the London Health Sciences Centre (LHSC). The model leverages agent-specific knowledge at the point of care and provides a structure aimed at building human resources capacity and sustaining enhancements to quality and safe care delivery. Interprofessional and cross-functional teams work through the CQI councils to identify, formulate, execute and evaluate CQI initiatives. In addition to a structure that facilitates collaboration, accountability and ownership, a corporate CQI Steering Committee provides the forum for scaling up and spreading this model. Point-of-care staff, clinical management and educators were trained in LEAN methodology and patient experience-based design to ensure sufficient knowledge and resources to support the implementation.
To date, 61 interprofessional and cross-functional councils have been established. There are 120 quality improvement and patient safety initiatives at various stages of implementation and evaluation. These improvements range from evidence-based practice integration "firsts" to staff-led process and system redesign. The standardization of processes and procedures across CQI council initiatives has spurred development of a variety of best practices and clinical efficiencies. Projects have been replicated up to 14 times across clinical units, and learnings from initial projects have supported scaling-up opportunities. In addition, two evidence-based practice firsts – including the development of an acute oral care assessment tool and guidelines for implementation of oral care clinical neuroscience patients, as well as the utilization of colostrum for oral immune therapy for neonates and infants – have been introduced. Integral to sustained transformation is the clear articulation of expectations regarding system redesign through the eyes of the patient. Professional Scholarly Practice leadership, a robust communication strategy including a real-time, web-based registry program, GEMBA TV, weekly CQI stories and monthly continuous quality improvement reviews have supported the success of the model. The establishment of CQI councils at the unit level including supportive structures and processes helped to embed continuous quality improvement into our organizational culture.
Introduction
Widely observed and researched, radical changes in the work environment within the healthcare sector often have significant consequences for health professionals in fulfilling their professional practice mandates (Bamford-Wade and Moss 2010; Baumann et al. 2001). In response, organizations have developed a variety of professional practice models to guide individual clinical practice while empowering the health workforce and improving the quality of patient care (Bamford-Wade and Moss 2010; Baumann et al. 2001). Shared governance and continuous quality improvement (CQI) are concepts that have been re-introduced into the healthcare sector over recent decades through several iterations for the purpose of empowering point-of-care staff. Shared governance is an organizational commitment intended to empower staff through decision-making control over individual clinical practice, based on the principles of partnership, equity, accountability and ownership (Porter O'Grady 1992). The Registered Nurses' Association of Ontario notes that engagement with point-of-care staff is a requirement to achieve successful implementation of shared governance and foster mutual responsibility to improve nurses' work environments (RNAO 2008).
CQI is an approach to quality management that builds upon traditional quality assurance methodologies through emphasis on organizations and systems, with particular attention to process improvements rather than individuals. In their research, economists Wruck and Jensen (1994) defined quality improvement as a scientific, non-hierarchical application of technologies that increase an organization's efficiency and quality. Jensen and Meckling's (2009) work in economics and market analysis suggested that the critical factor for achieving quality in organizations is based on the cost of transferring information between individuals at all levels for everyday decision-making.
Although a positive relationship has been established between shared governance and CQI, the intervening concept, which is referred to as agent-specific knowledge, has not been explicitly identified (Bamford-Wade and Moss 2010; Brody et al. 2012; Anderson 2011). The existence of agent-specific knowledge is inferred as the value generated through the transfer of the locus of decision-making control to point-of-care staff (Jensen and Meckling 2009). A greater understanding of the structures and processes necessary to leverage agent-specific knowledge can enhance the opportunity for healthcare organizations to achieve continuous quality improvement goals.
Background
In 2011, London Health Sciences Centre (LHSC) renewed its vision for professional scholarly practice and embarked on a journey to establish structures and processes for shared governance as a means to achieve continuous quality improvement while maximizing agent-specific knowledge. The vision emphasized the importance of each point-of-care staff in shaping the direct delivery of care to patients, as well as the direct impact they have on their work environment through the use of general and specific knowledge to achieve continuous quality improvements.
Within the quality improvement paradigm, the organization of procedures and processes has the potential to increase efficiency and quality of care. However, these elements are highly dependent on the utilization of data and scientific method in decision-making. Quality improvement and shared governance can be linked by mobilizing specific knowledge. Jensen and Meckling (2009) defined specific knowledge as knowledge that is "costly to transfer." In the healthcare setting, specific knowledge refers to unique insights and knowledge that agents of the organization possess, which can be difficult to extract and transfer to other team or organizational members.
Generous funding was provided in September 2011 through the Quality Nursing Environments – Quality Patient Care Fund and Late Career Nurse Initiative of the Ontario Ministry of Health and Long-Term Care (MOHLTC) to implement the CQI initiative at LHSC. The STAR model was adapted and used to frame large-scale change management for LHSC's multi-site organization, with consideration for goals and tasks, structure, information and decision support, people and human resources management, and acknowledgement to create a culture that values leveraging and mobilizing agent-specific knowledge (Golden and Martin 2004; Golden 2006).
Initiative Overview
LHSC undertook to implement throughout the organization a shared governance structure that embraced CQI. Planning for the initiative began in early 2011 with the launch of the inaugural Professional Scholarly Practice conference, Professional Practice at Its Best. This conference engaged front-line management, point-of-care staff and clinical educators to discuss factors affecting their work environment and to visualize the ideal setting in which to practise. The plan to integrate CQI councils at the unit level was announced, and expectations of staff and their role in this new model were set. Through standardized principles and terms of reference applied to all CQI councils, the councils were mandated to incorporate interprofessional and cross-functional membership to reflect the complexity of direct and indirect services that must be seamlessly integrated to achieve high-quality results and support short- and long-term planning, implementation and evaluation of CQI projects.
To enable the work of the CQI councils, over 175 point-of-care staff, clinical management and educators were provided training in quality improvement methodologies such as LEAN, root-cause analysis, 5S organization and Plan-Do-Check-Act. Furthermore, patient experience-based design was incorporated into the educational components of the program to maximize the redesign of systems and processes using "patient-specific knowledge" along with agent-specific knowledge. The training provided the knowledge and skill that empowered staff to diagnose poor quality, define problems, identify root causes, conduct detailed analyses, and lead, implement and evaluate quality improvement initiatives.
CQI councils reported progress and accomplishments to a corporate CQI Steering Committee, which was the central structure that facilitated collaboration, accountability and ownership and provided the forum for the scaling up and spread of initiatives. Staff were engaged through a robust communication strategy including a real-time, web-based registry program, GEMBA TV (recorded visits to CQI councils), weekly CQI stories available to all staff through the LHSC intranet and monthly continuous quality improvement reviews – all of which have supported the success of the model through ongoing acknowledgement and dissemination of information.
In November 2012, approximately 12 months following the implementation of the CQI councils, Professional Practice at Its Best was held, providing participants the opportunity to present CQI initiatives in scientific abstract, poster and presentation format. Through collaboration with Professional Scholarly Practice and the Health Sciences Library, point-of-care staff submitted and presented 25 CQI projects. Participants revealed key enablers to achieving success through CQI councils and sustaining the cultural transformation including: administrative support and willingness to leverage agent-specific knowledge; resource and capacity building to implement quality improvement initiatives; dissemination of information and opportunity to spread leading practices through the CQI Steering Committee; and consistent acknowledgement of accomplishments.
Outcomes
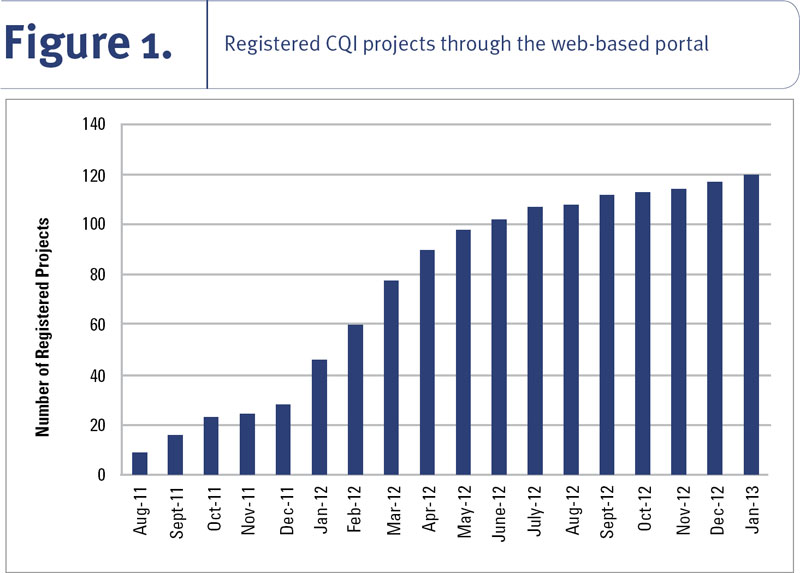
To date, 61 interprofessional and cross-functional councils have been established at LHSC, registering 120 quality improvement and patient safety initiatives in various stages of implementation and evaluation. These improvements range from evidence-based practice integration firsts to staff-led process and system redesign. As projects were registered with the real-time CQI Registry (Figure 1), LHSC has sustained an average of five new initiatives implemented per month over the last 18 months.
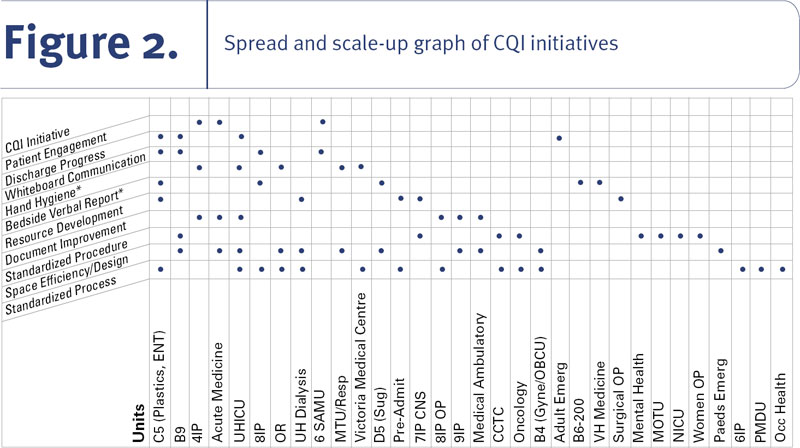
As registrations increased, a distinct pattern began to appear in which CQI councils began to undertake rapid-cycle improvements based on the observed work of other councils. This led to mapping the development of spread and scale-up of CQI initiatives across the organization (Figure 2). Importantly, some initiatives have been replicated up to 14 times, increasing standardization, best practices and clinical efficiencies in multiple clinical units.
In addition, arising from direct observations and specific knowledge at the point of care, two evidence-based practice firsts have been implemented at LHSC, including the development of an acute oral care assessment tool and guideline for implementation of oral care for clinical neurological patients (Letsos et al. 2013) and utilization of colostrum for oral immune therapy for neonates and infants (Pletsch et al. 2013). Several CQI councils reported findings from the evaluation of quality and safety improvement initiatives that demonstrated success. For example, the implementation of verbal bedside reporting resulted in an 80% decrease in critical incident reports across several clinical units. Similarly, units implementing whiteboard communication systems experienced a 45% increase in accuracy for daily predictive discharge. Feedback was regularly solicited from staff regarding the implementation of the shared governance model. Table 1 identifies the key themes that emerged from staff feedback regarding the CQI council model.
| Table 1. Staff feedback regarding the transition towards staff-driven change | |
| Traditional Style Management | LHSC Shared Governance Model |
| Decisions are position-based | Decisions are knowledge-based |
| Limited staff expectation and input | High staff expectation and input |
| Silo mentality ➡ blame mentality | Systems appreciation ➡ integrated partnerships |
| Hierarchical communication | Open communication |
| Implicit value of point-of-care staff | Explicit value of point-of-care staff |
| Extrinsically driven quality | Intrinsically driven quality |
| Change driven top-down | Change driven bottom-up |
| Limited knowledge transfer ➡ isolated pockets of innovations and excellence | Significant increase in knowledge transfer ➡ spread of innovations, excellence and standardization |
| Failures were failures, and to be avoided | Acknowledging "failures" allowed staff to feel disappointment, but also the opportunity to approach problem-solving from a different perspective |
Discussion
Undertaking an organization-wide change to channel decisions driven by agent-specific knowledge required a significant upfront investment and served to solidify the foundation of what defined professional practice at LHSC – every professional is responsible for delivering the highest-quality care to patients and improving the quality of care delivered (Figure 3).

The initial investment to provide the educational and analytical support for all staff is critical, as is the explicit linkages among professional practice, ownership and accountability for delivering and improving the quality and safety of care delivery (Ballard 2010; Golden and Martin 2004; Golden 2006). The primary responsibility for nursing leadership is to create the supportive culture that allows point-of-care staff to experience and lead innovations, which Golden (2006) stated, "simultaneously puts patients first, and makes staff feel accountable for both fiscal and clinical outcomes."
The Institute for Healthcare Improvement concept of the Triple Aim is based on improvements in patient experience, population health and per capita costs (IHI 2012). The Fourth Aim, which to date has received little attention, is the capacity of staff to engage in continuous quality improvement. Building staff capacity and the structures and processes required to foster and sustain a culture of safety, high quality and professional practice maximizes the potential for the first three aims to be achieved.
Implementation of a shared governance model through CQI councils at LHSC elucidated the pivotal role that nurses play in improving organizational quality and safety outcomes, as well as direct patient outcomes. Building staff capacity to lead quality improvement initiatives stimulated the spirit of clinical scientific inquiry and encouraged creativity and innovation. Establishment of CQI councils at the unit level and the integration of supportive structures and processes helped to embed continuous quality improvement in the organization's culture. The value of agent-specific knowledge has been demonstrated in several research and evaluative studies across LHSC that revealed positive patient and organizational outcomes in response to CQI initiatives. These evaluative studies and research findings will be articulated in the papers that follow in this Special Issue of the journal.
Conclusion
As the climate of change and requirement for adaptability continue to increase in healthcare today, organizations will need to recognize the intrinsic value that each professional brings to the organization. Implementation of a shared governance model to facilitate continuous quality improvement by leveraging agent-specific knowledge demonstrated positive outcomes. A greater understanding of the structures and processes necessary to leverage such knowledge can enhance the opportunity for healthcare organizations to achieve continuous quality improvement goals.
About the Author(s)
Vanessa Burkoski, RN, BScN, NP-PHC, MScN, DHA, Vice President/Chief Nursing Executive, Quality, Patient Safety and Professional Scholarly Practice
Jennifer Yoon, RN, BScN, Director, Nursing Professional Scholarly Practice, London Health Sciences Centre
Correspondence may be directed to: Vanessa Burkoski, Vice President/Chief Nursing Executive, Quality, Patient Safety, and Professional Scholarly Practice. London Health Sciences Centre, 800 Commissioners Road East, PO Box 5010, London, Ontario, N6A 5W9; e-mail: Vanessa.burkoski@lhsc.on.ca
Acknowledgment
We wish to thank the following people for their assistance with this study: Lisa Ducharme, Elizabeth McMurray, Jennifer Mellecke, Alison Armstrong, Gail Barbour, Margaret Belliveau, Karen Burnett, Susan Carter, Hazel Celestino, Amy Domingues, Kristen Dove, Diane Edgar, Christina Gavrelets, Michelle Grigg, Janet Groom, Sandra Harwood, Jonathan Hogeterp, Alexandria Houston, Lisa Janisse, Karen Laidlaw, Karilyn Lamers, Cassandra Luyten, Cheryle Anne MacBelford, Betty Malloy-Nantais, Eleanor Marris-Rogers, Rachelle McCready, Allison McLachlan, Anne McVety, Lori O'Brien, Tara Oke, Monica Pint, Donna Pletsch, Lynda Quinn, Lynda Ryall-Henke, Krista Shea, Gina Souliere, Patricia Stalker, Kathryn Walton, Barbara Watson, Debbie Wawryszyn, Debra Wolski, Laurie Young, Minakshi Sharma, Karla Van Kessel, Shauna-Lee Konrad, Sylvia Katzer, Colleen Keeler, Chuck Loblaw, Sylvia Diaz, Rachel Twoey, Michele Martin, Sarah Muto, all CQI Councils, members and chairs.
References
Anderson, E.F. 2011. "A Case for Measuring Governance." Nursing Administration Quarterly 35: 197–203.
Ballard, N. 2010. "Factors Associated with Success and Breakdown of Shared Governance." Journal of Nursing Administration 40: 411–16.
Bamford-Wade, A. and C. Moss. 2010. "Transformational Leadership and Shared Governance: An Action Study." Journal of Nursing Management 18: 815–21.
Baumann, A., L. O'Brien-Pallas and M. Armstrong-Stassen. 2001. Commitment and Care: The Benefits of a Healthy Workplace for Nurses, Their Patients and the System. A Policy Synthesis. Ottawa: Canadian Health Services Research Foundation.
Brody, A.A., K. Barnes, C. Ruble and J. Sakowski. 2012. "Evidence-Based Practice Councils: Potential Path to Staff Nurse Empowerment and Leadership Growth." Journal of Nursing Administration 42: 28–33.
Golden, B. 2006. "Transforming Healthcare Organizations." Healthcare Quarterly 10: 10–19.
Golden, B. and R.L. Martin. 2004. "Aligning the Stars: Using Systems Thinking to (Re)Design Canadian Healthcare." Healthcare Quarterly 4: 34–42.
Institute for Healthcare Improvement (IHI). 2013. IHI Triple Aim Initiative. Retrieved March 25, 2013. <http://www.ihi.org/offerings/Initiatives/TripleAim/Pages/default.aspx>.
Jensen, M.C. and W.H. Meckling. 1992. "Specific and General Knowledge, and Organizational Structure." In L. Werin and H. Wijkander, eds., Contract Economics (pp. 251–74). Oxford: Blackwell.
Jensen, M.C. and W.H. Meckling. 2009. "Specific Knowledge and Divisional Performance Measurement." Journal of Applied Corporate Finance 21(2): 49–57.
Porter-O'Grady, T. 1992. "A Decade of Organizational Change." In T. Porter-O'Grady, ed., Implementing Shared Governance: Creating a Professional Organization (pp. 25–51). St. Louis: Mosby Year Book.
Registered Nurses' Association of Ontario (RNAO). 2008. Healthy Work Environment Best Practice Guidelines: Workplace Health, Safety and Well-Being of the Nurse. Toronto: Author.
Wruck, K.H. and M.C. Jensen. 1994. "Science, Specific Knowledge and Total Quality Management." Journal of Accounting and Economics 18: 248–87.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed