
Healthcare Quarterly
Assessing Primary Healthcare Using pan-Canadian Indicators of Health and Health System Performance
Michael Terner, Jennifer D'Silva, Brenda Tipper, Olga Krylova and Greg Webster
Abstract
Updated primary healthcare (PHC) indicators are now available for use across Canada. The Canadian Institute for Health Information identified and updated two sets of priority indicators – a policy set to meet the needs of policy makers and a provider set to meet the needs of providers of PHC at the practice and organization levels. A total of 51 indicator definitions were updated to ensure that they are measurable and operational, align with clinical practice guidelines and available data sources and reflect important dimensions of PHC performance in Canada.
Standardized performance measures are a key aspect of any performance improvement process. They help us understand where we are doing well, what could be improved and if initiatives and interventions are having the desired effect. Measuring performance of primary healthcare (PHC) systems in Canada poses a number of challenges. There is limited availability of high-quality PHC data (Broemeling et al. 2009), and regional differences in indicator methodology limit comparisons of performance across jurisdictions (Health Council of Canada 2012). Nevertheless, standardized data and indicator reporting across jurisdictions are vital for continual assessment of the PHC system in Canada (Canadian Health Services Research Foundation 2012).
In 2006, the Canadian Institute for Health Information (CIHI) released a set of 105 pan-Canadian PHC indicators that were developed to measure and compare PHC performance at multiple levels within and across jurisdictions in Canada (CIHI 2006). Since 2006, clinical practice guidelines have been updated, and new PHC data sources and standards are developing that fill data gaps. As a result, CIHI identified a need to update these original indicators. The goals of the update were to ensure that the indicators:
- are measurable and operational across Canada,
- align with clinical practice guidelines,
- align with available data sources and
- reflect key dimensions of PHC performance in Canada.
An advantage of developing indicators for pan-Canadian use is that these indicators can be employed for comparison across regions, provinces and organizations as well as to measure trends over time. By using a single indicator methodology, stakeholders can compare performance and benchmark against peers; that can facilitate the sharing of effective quality improvement programs and initiatives.
Process for Identifying and Updating Priority Indicators
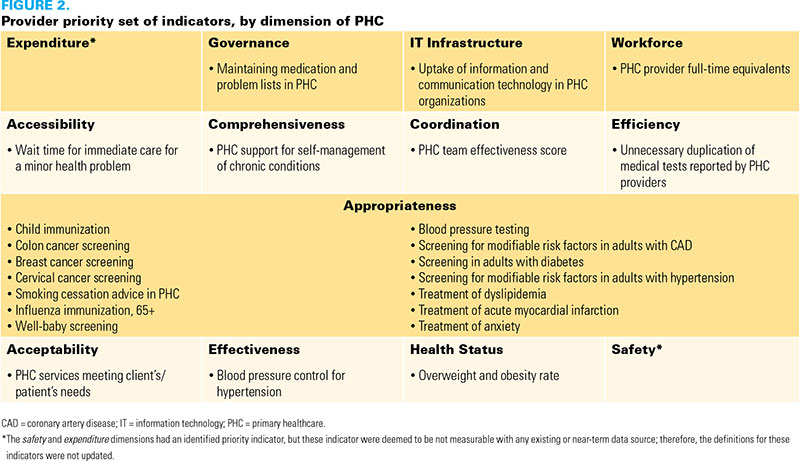
CIHI reviewed established PHC frameworks and definitions of dimensions of PHC in order to develop a conceptual organization (see Figures 1 and 2) for the 105 PHC indicators (Haggerty et al. 2007; Hogg et al. 2008; Kringos et al. 2010; Watson et al. 2004). CIHI used this conceptual organization to ensure that both the policy and provider sets of indicators would have at least one indicator from key dimensions of PHC.

The next step CIHI took in updating priority sets of PHC indicators was to identify which indicators from the list of 105 PHC indicators were a priority for measurement. CIHI surveyed stakeholders of PHC from across Canada to rate the importance of the 105 indicators from a policy (health-system level) perspective and from a provider (practice/organization level) perspective. Using the results of these surveys, CIHI selected the highest-rated indicator within each PHC dimension and then completed each set selecting the overall highest-rated indicators, up to 30 indicators per set.
CIHI established working groups to review and update the definitions of the priority indicators. The working groups were composed of members from all Canadian provinces and territories and included representatives of or those affiliated with ministries of health, health quality councils and research organizations and academic research institutions as well as subject matter experts and clinicians.
The first step in the review by working groups was to determine whether the indicators within each priority set were feasible for measurement. Considerations for a preferred data source included the degree of coverage, accessibility of the data and how frequently the data are updated. Once potential data sources were identified, the working groups completed the updating of indicator definitions in three rounds of engagement:
- Round one – Working group members reviewed background material – including a clinical evidence review and an existing environmental scan – on each of the priority indicators and raised issues with the indicator definitions.
- Round two – Working group members discussed the issues with the indicator definitions and selected the preferred data source from which each indicator could be calculated.
- Round three – Working group members voted on revised indicator definitions that were drafted by CIHI using input from round two.
Participation in the various stages of the project was strong and is summarized in Table 1.
| TABLE 1. Response rates by project stage | ||
| Project Stage | Number of Participants | Response Rate (%) |
| Policy survey | 25 of 42 surveys were returned | 60 |
| Provider survey | 42 of 56 surveys were returned | 75 |
| Working group – round 1 (review) | 45 of 49 members participated | 92 |
| Working group – round 2 (discussion) | 38 of 50 members participated | 76 |
| Working group – round 3 (consensus voting) | 41 of 51 voting members participated | 80 |
Updated PHC Indicators
Between the two priority sets, a total of 51 indicators (out of 60 identified priority indicators) had definitions that were updated. Nine of the identified priority indicators were deemed not measurable across Canada with any existing or developing data source; therefore, the definitions were not updated. Indicators were grouped within the conceptual organization so that users could search through available indicators by dimension of PHC and indicators covering similar topics could be grouped together (for example, cancer screenings). Technical specifications were updated for each of the 51 indicators, which included the following information: indicator definition, numerator and denominator, inclusion and exclusion criteria, data source, notes and rationale.
Listings of updated indicators for the policy and provider priority sets are presented in Figures 1 and 2, respectively. Complete technical specifications are included in a report available on CIHI's website at www.cihi.ca/phc (CIHI 2012).
Discussion
CIHI updated the pan-Canadian PHC indicators to promote and increase the capacity for standardized PHC measurement across Canada. The consensus-driven approach was designed to ensure that there was representation from jurisdictions across Canada, from different users of PHC indicators and from subject matter experts.
Within the technical specifications for each of the indicators, a potential pan-Canadian data source is listed. This does not preclude adapting these indicators to established, high-quality local data sources, which can result in more accurate results for intra-jurisdictional reporting. Some examples of regional data include Manitoba Health's Physician Integrated Network and the 2011 Primary Health Care Survey, conducted by the New Brunswick Health Council.
The priority sets of indicators were designed to be versatile and support a multitude of potential uses. The indicators within the policy set can be used to support population-based policy development and planning by assessing and monitoring the performance of the PHC system across healthcare regions. The indicators within this set can also be used to support funding decisions and to identify gaps in the health of a population or community. The indicators within the provider set can be used both within and among practices, organizations and health regions to assess and compare performance among organizations and providers of PHC. The indicators within this set can be used to inform quality improvement programs, support program sharing and identify opportunities for improvements in the health of a practice population.
This indicator update project is an important part of CIHI's PHC Data and Information program, which also involves developing standard PHC survey tools, data standards for electronic medical records as well as the Voluntary Reporting System. CIHI will continue to lead the development and support of pan-Canadian standards for measurement of the PHC system in Canada. Together, both sets of indicators are intended to improve PHC performance by increasing the ability of decision-makers to measure and compare PHC performance across Canada.
About the Author(s)
Michael Terner, MSc, is a program lead with the Primary Health Care (PHC) Information and Clinical Registries branch at the Canadian Institute for Health Information (CIHI). He has previously worked as a medical writer in the clinical research industry and as a researcher at several federal government agencies.
Jennifer D'Silva, MSc, is a project lead with the Health System Research team at CIHI. She has over nine years of experience in health services research and performance measurement.
Brenda Tipper, MHSc, is the senior program consultant with Health System Performance at CIHI. She has worked on health system performance assessments as a consultant to the World Health Organization. Previous consulting work with the Ontario Ministry of Health and Long-Term Care included development of a primary healthcare scorecard for Ontario.
Olga Krylova, PhD, is a senior analyst with the Health System Research team at CIHI. She has extensive experience in epidemiological research and health data analysis.
Greg Webster, MSc, is the director of PHC Information and Clinical Registries at CIHI. He has 20 years of experience using health data, information and evidence to improve health and healthcare. He also has extensive experience leading and achieving results through networks and partnerships.
References
Broemeling, A.M., D.E. Watson, C. Black and S.T. Wong. 2009. "Measuring the Performance of Primary Healthcare: Existing Capacity and Potential Information to Support Population-Based Analyses." Healthcare Policy 5(Special Issue): 47–64.
Canadian Health Services Research Foundation. 2012. The Economic Impact of Improvements in Primary Healthcare Performance. Ottawa, ON: Author.
Canadian Institute for Health Information. 2006. Pan-Canadian Primary Health Care Indicators: Report 1, Volumes 1 and 2. Ottawa, ON: Author.
Canadian Institute for Health Information. 2012. Pan-Canadian Primary Health Care Indicator Update Report. Ottawa, ON: Author.
Haggerty, J., F. Burge, J.F. Levesque, D. Gass, R. Pineault, M.D. Beaulieu et al. 2007. "Operational Definitions of Attributes of Primary Health Care: Consensus among Canadian Experts." Annals of Family Medicine 5(4): 336–44.
Health Council of Canada. 2012. Measuring and Reporting on Health System Performance in Canada: Opportunities for Improvement. Toronto, ON: Author.
Hogg, W., M. Rowan, G. Russell, R. Geneau and L. Muldoon. 2008. "Framework for Primary Care Organizations: The Importance of a Structural Domain." International Journal for Quality in Health Care 20(5): 308–13.
Kringos, D.S., W.G.W. Boerma, Y. Bourgueil, T. Cartier, T. Hasvold, A. Hutchinson et al. 2010. "The European Primary Care Monitor: Structure, Process and Outcome Indicators." BMC Family Practice 11: 81.
Watson D.E., A. Broemeling, R.J. Reid and C. Black. 2004. A Results-Based Logic Model for Primary Health Care. Laying an Evidence-Based Foundation to Guide Performance Measurement, Monitoring and Evaluation. Vancouver, BC: Centre for Health Services and Policy Research.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed