
Healthcare Policy
Abstract
Background: Extracorporeal shock wave lithotripsy (ESWL) is a definitive, ambulatory and non-invasive modality for treating kidney stones. ESWL is not available in all urban centres and many Canadians must either travel, sometimes out of province, or wait to have this procedure performed. We sought to evaluate the variability in access to ESWL treatment.
Method: We compiled a comprehensive list of ESWL centres in Canada and contacted all centres in 2011 to assess their wait times, out-of-province patient fees, and roles and responsibilities of the referring physician.
Results: We contacted all 23 ESWL facilities across Canada (100% response rate). Wait times for elective ESWL procedures ranged from one day to over one year, with a mean of 8.4 weeks (SD, 16.76 weeks). No centres refused out-of-province patients, although five discouraged travel to their centre owing to their prolonged wait times. No facilities charged extra fees for out-of-province patients. Ten (43%) facilities required a secondary consultation by a urologist at the centre before booking. Twelve (52%) of the centres indicated the waiting time could be shortened if the referring physician were to advocate on the patient's behalf. Contact was repeated one year later in 2012 with five centres, and the results were similar.
Interpretation: There is marked variation in wait times across Canada for ESWL but there are few barriers to care. Patients' waits may be shortened by physician advocacy.
The incidence and prevalence of nephrolithiasis in canadians are high, with a lifetime risk of 10% and a recurrence risk approaching 75% at 20 years (Moe 2006). One of the mainstays of therapy for kidney stones is extracorporeal shock wave lithotripsy (ESWL). Its use is also determined by stone type, location and composition (Auge 2002). ESWL offers definitive treatment that is non-invasive, fast and most often performed as an outpatient procedure (Nabi et al. 2007; Srisubat et al. 2009). Further, ESWL offers high success rates (Nabi et al. 2007) and lower rates of hospital stay, treatment duration and complications, and it is less invasive (Srisubat et al. 2009).
Anecdotal reports describe long waits for ESWL at many centres. Indeed, lithotripsy is widely indicated, and is often the management of choice for both patients and physicians (Karlsen et al. 2007). However, the Canadian Coordinating Office for Health Technology Assessment formally documented only 13 lithotripters in Canada (CCOHTA 2001), associated with long patient waits and travel to gain access. As a result, patients may opt for more invasive surgical treatment (Mahoney 2001). The small number of ESWL treatment facilities – there are now 23 centres – may not have kept pace with Canada's growing and aging population. Moreover, there remains considerable inequality in access to this therapy (Fergusson 2002).
Timely access to care is a major component in reducing morbidity. If patients experience significant barriers in receiving medical treatment, they may suffer a lower quality of life (CSDH 2008). When technological resources are limited, unavailable or substantially delayed, patients may choose more invasive treatments, or suffer pain and anxiety while on a lengthy wait list. We sought to evaluate the variability in access to timely ESWL treatment for Canadians.
Methods
The study population included all publicly funded centres in Canada that own or operate a lithotripter machine, with no exclusions. We did not identify any privately operating machines. As there was no current, comprehensive inventory of all lithotripters in Canada, these centres were preliminarily identified using the CCOHTA 2001 inventory and Internet searches. The Canadian Institute for Health Information reported no freestanding lithotripters at the start of this study (CIHI 2006). These data were confirmed by inquiries at neighbouring centres.
Telephone surveys were conducted between February and May 2011, from two perspectives: one from the perspective of an in-province patient, and another from that of an out-of-province patient. A template was used to guide the interviewer, and to standardize the telephone interviews (Appendix 1 available online at longwoods.com/content/23605). During these conversations, the interviewer asked to speak with a clinic employee who could best answer administrative questions over the phone about the process involved in obtaining ESWL (i.e., consultation, patient selection, procedure and follow-up). All qualitative interview comments were transcribed and categorized into thematic groups for qualitative data analysis, including steps to book a lithotripsy appointment, the need for a second referral to the urologist in consideration, and whether there was any room for advocacy on the part of the referring physician. Generally, provinces cover out-of-province fees for emergency care, but often pre-approval is required for out-of-province elective care. In this study, centres were not questioned further on the procedure for obtaining insurance from the patient's home province prior to receiving treatment out of province, or on the possibility of out-of-pocket payment and subsequent reimbursement. We did not inquire about private access to ESWL. Quantitative data included the wait time until the patient could receive therapeutic ESWL. Data were standardized by measuring the wait, in weeks, to the time of earliest possible treatment.
Interviews were conducted during business hours. The primary booking agent and/or nursing staff provided responses. We did not disclose our research intent, because this may have reduced our response rate. To avoid inadvertently cueing individual respondents, each hospital was contacted only once or as minimally as necessary to obtain survey responses, with sufficient time between contacts to avoid carry-over effects.
The investigators anticipated this study to be ethical and feasible in a broad capacity. The phone interviews were kept to 10 minutes or less in order to consume only a brief amount of time on the part of lithotripsy staff and reduce the impact of the research on the productivity of lithotripsy clinics. The nature of the survey process, which is crucial to the study's method, did involve mild deception as the research intent was not disclosed; however, it was felt that this would not cause undue harm to the respondent. The interviews were conducted from the perspective of the patient rather than a physician, administrative staff, lawyer or technician, in part to illustrate the patient experience in navigating the healthcare system, and further not to impose any pressure or obligation for the respondent to divulge information that would otherwise be inappropriate to disclose. Ethics approval was obtained from the St. Michael's Hospital Research Ethics Board.
Data were tabulated, and we analyzed numeric data for significant differences among wait times across Canada. The mean, standard deviation, median and interquartile range were evaluated. The midpoints of estimates were counted as responses (e.g., "one to two weeks" was noted as 1.5 weeks). Qualitative data were collected on the process of obtaining lithotripsy out of province, including whether a referral, imaging and a second consult were required, as well as whether there was an opportunity for patient advocacy on the part of the referring physician.
We repeated phone interviews in July 2012 with five (22%) randomly chosen facilities to assess the reproducibility of our results. We did not make any reference to our original conversation when calling for a repeat estimate.
Results
We contacted all 23 publicly funded centres in Canada that perform ESWL (Table 1). No institution was lost to follow-up or declined to answer (100% response rate). In large part, the lithotripsy machinery was located at one health centre. However, in the Maritimes, one single, travelling lithotripter serviced seven different hospitals (Charlottetown, Prince Edward Island; Fredericton, New Brunswick; Mirimichi, New Brunswick; Bathurst, New Brunswick; Edmundston, New Brunswick; and two facilities in Moncton, New Brunswick) on a rotating basis (UMS 2010). These centres were counted individually in this study, as the machine did not spend equal amounts of time at each centre, and their wait times varied.
| Table 1. Quantity and location of lithotripters in Canada, by province | ||
| Province/Territory | No. of Lithotripters | Location |
| British Columbia | 3 | Vancouver General Hospital (Vancouver), Royal Jubilee Hospital (Victoria), Prince George Regional Hospital (Prince George) |
| Alberta | 2 | Misericordia Community Hospital (Edmonton), Rockyview General Hospital (Calgary) |
| Saskatchewan | 1 | St. Paul's Hospital (Saskatoon) |
| Manitoba | 1 | Health Sciences Centre (Winnipeg) |
| Ontario | 3 | St. Michael's Hospital (Toronto), Ottawa Hospital Riverside Campus (Ottawa), St. Joseph's Healthcare (London) |
| Quebec | 3 | CHUM – St. Luc Hospital (Montreal), MUHC – Royal Victoria Hospital (Montreal), St. François d'Assise (Quebec City) |
| Nova Scotia | 1 | Victoria General Hospital (Halifax) |
| New Brunswick | Travelling (6) | Dr. Everett Chalmers Hospital (Fredericton), Moncton Hospital (Moncton), GeorgesDumont Hospital (Moncton), Miramichi Regional Hospital (Miramichi), Chaleur Regional Hospital (Bathurst), Edmundston Regional Hospital (Edmundston), |
| New Brunswick | 1 | St. Joseph's Hospital (St. John) |
| PEI | Travelling (1) | Queen Elizabeth Hospital (Charlottetown) |
| Newfoundland & Labrador | 1 | Health Sciences Centre (St. John's) |
| Yukon | 0 | N/A |
| NWT | 0 | N/A |
| Nunavut | 0 | N/A |
The mean wait time for ESWL was 8.4 weeks but varied greatly (SD, 16.76 weeks; range, 0–78 weeks). The median wait time was 5 weeks (interquartile range, 1–12 weeks) (Figure 1).
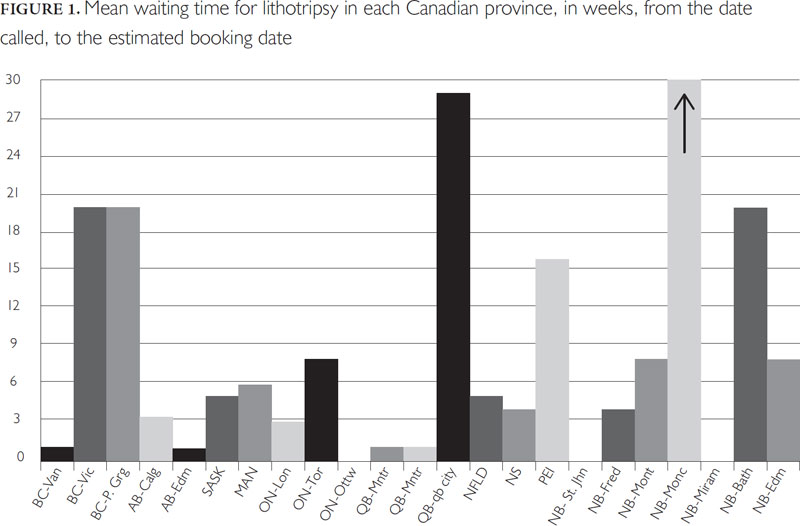
No lithotripsy centre refused out-of-province patients. The majority (19/23) were willing to accept out-of-province patients readily. Five centres, however, did indicate that it would be inadvisable for patients to seek lithotripsy at their centre, as the wait lists were "far too long" and it would "not be worth the travel."
There were no supplemental fees imposed on out-of-province patients. However, travel costs, food and accommodation while on medical leave, and any additional services were not compensated by any party.
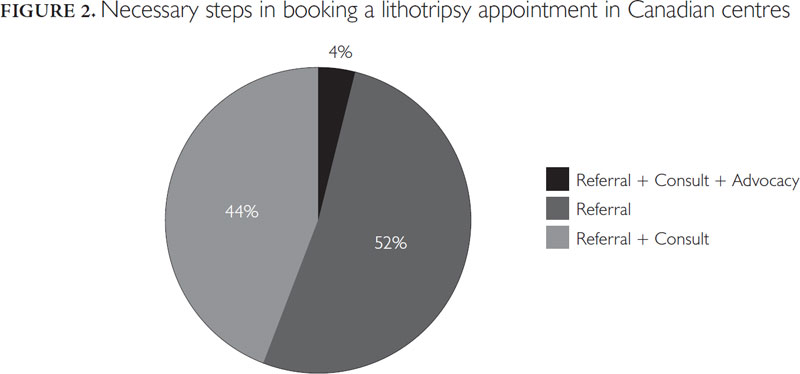
Twelve (52%) of 23 centres required only a referral from the patient's current urologist or family doctor to book an appointment. Ten (43%) required a secondary consultation by a urologist at the centre before booking. This step often involved repeat diagnostic imaging. One centre (4%) indicated that the referring physician would be expected to contact the urologist and give an explanation for the need to have the patient receive ESWL at their centre given the long wait time (Figure 2).
All centres were surveyed on whether lithotripsy could be booked at an earlier date. Booking staff were specifically asked if there was anything the referring physician could do to "get the appointment made sooner" than the previously quoted wait time. Eleven (48%) declined on account of their long waits. The other 12 (52%) centres indicated that if the referring physician were to lobby on the patient's behalf, waits could be shortened.
For the five repeat interviews, one of the repeat estimates was identical to the original. For the remaining four, the mean difference between original and repeat wait time was two weeks (range, 0.5–4 weeks). All of these four centres had longer waits than the original estimate.
Discussion
We believe we identified all 23 facilities in Canada that offer ESWL for kidney stones. Our study found a mean wait time of approximately eight weeks for the procedure, but marked variation in wait times across Canada. We found few other notable barriers to care. With respect to the steps to secure an out-of-province ESWL appointment, in many cases, patients' waits could be shortened by advocacy on the part of the referring physician. Each centre's wait time was measured from the time of approval that the patient was a suitable candidate for ESWL by the centre's urologist to the time of treatment, not from the time of referral from the home-province physician. The display in variation in the steps to securing the first appointment identifies a possible mechanism for delay that may be unknown to the patient and referring physician.
Our study is unique because we solicited wait times for ESWL from a patient perspective. Our simple telephone interviews helped us to achieve a 100% response rate. Further, we reduced potential bias by not disclosing our research intent, because this may have reduced our response rate or modified our estimates. The estimates are accurate as evidenced by our repeat subsequent survey. As well, there has been little empiric study of wait times for ESWL in Canada or elsewhere.
Lithotripsy is a medically indicated technology that can both enhance the quality of patients' lives while saving considerable costs when compared to more invasive methods (Rublee 1989). The results of this study, however, illustrate long wait times in Canada, particularly in the Maritime provinces compared to Western and Central Canada. This cross-Canada trend is in keeping with other observed waits for specialists (Barua et al. 2011). Further, an asymmetrical distribution in wait times for ESWL exists within the provinces themselves. For example, in Ontario, patients in Ottawa may be booked for ESWL within days, while those in Toronto might wait as long as eight weeks. By international comparison, Australian urological data show similar regional variation in wait times, although not as marked as in our findings (AIHW 2010). Thus, variation in access for Canadians with kidney stones exists at the inter- and intraprovincial levels. These patients may ultimately resort to more invasive surgical procedures when they are not informed that a centre nearby may have shorter waits. Indeed, at least 10% of Canadians who wait for elective surgery are significantly affected by worry, anxiety, stress and pain (Sanmartin et al. 2004).
Our findings bring ESWL wait times in Canada to light. Despite many recent improvements, patients have little access – online or otherwise – to this information, despite well-publicized provincial campaigns such as the Ontario Wait Time Strategy (MOHLTC 2011) and the federal Health Services Access Survey (Sanmartin et al. 2004). These programs have made progress on this front and host a website for the Ontario Wait Time Strategy, allowing patients to search for the wait times of various procedures. However, this tool does not differentiate between the various treatment modalities for kidney stones, nor is it specific for surgeon or centre. Similarly, Australia's National Partnership Agreement on the Elective Surgery Waiting List Reduction Plan tells patients little about the wait times for individual urological procedures (SCRGSP 2011). Currently, Ontario, Alberta, British Columbia and Saskatchewan report the greatest amount of wait-time information, including and beyond the five priority areas of the Canadian Wait Time Alliance (diagnostic imaging, joint replacement, cancer care, sight restoration and cardiac care) (WTA 2011). But even these improvements are not unanimously reported across the country, and access to this information for Canadians is variable at best (CIHI 2006). There is great variability in information-sharing across the country and within provinces.
Canadian wait times and access to other high-demand procedures and technologies are equally varied across the country and in comparison to other countries (Esmail and Walker 2008). A nationwide survey of MRI facilities in 2007 demonstrated that the wait times were highly variable from province to province, and that 22% of centres imposed barriers for out-of-province patients to access care (Revah and Bell 2007).
The Organisation for Economic Co-operation and Development has generated the most comprehensive study of lithotripsy availability, among other medical technologies. Reports from 2002 and 2008 placed Canada second last in lithotripters per million population and near the bottom in absolute numbers of machines (Esmail and Walker 2008; Harriman et al. 1999; OECD 2011). Still, the OECD's most contemporary reports do not include centre-specific wait-time data. Further, not only is Canada's lithotripsy care in short supply, but at the start of 2007 nearly 34% of Canada's 19 lithotripters were more than 10 years old, with the oldest at 26 years (CIHI 2008; Esmail 2008). Further, the Canadian Association of Radiologists regards lithotripsy equipment as outdated after seven years of life, dating Canada's equipment even further compared to countries like Japan (CAR 2000; Otsubo et al. 2011).
Limitations and strengths
Our study has some limitations. First, there may be temporal fluctuations in wait times based on seasonal variation and vacation times. However, the study was conducted within a short and finite amount of time, which reduced variability. Moreover, a sample of the estimates was similar to those obtained at a later date. Second, it is conceivable that the interviewees were reluctant to provide answers, given that the researchers were not introduced as physicians but as patients, and it is not customary for some facilities to disclose this information directly to a patient. However, this approach allowed us to assess accessibility to lithotripsy from a patient's perspective. Further, the findings illustrate both the variability in wait times as well as the transparency of this information for patients navigating the system. By surveying lithotripsy centres in this fashion, we also illustrate the degree of information available to patients who are willing and able to travel for earlier treatment.
Our study has important relevance to clinicians and policy makers. First, it is encouraging that the barriers to care in other provinces are minor. Although access is guaranteed in the Canada Health Act, other studies have documented significant barriers to intraprovincial care in Canada (Revah and Bell 2007). As well, the qualitative results of our research demonstrate an opportunity for referring clinicians to advocate on behalf of their patients to shorten waits and for patients (and clinicians) to shop around for shorter waits.
Second, our findings suggest that provincial funding to evidence-based, non-invasive procedures like ESWL should be re-evaluated. This was not our a priori objective, but it did become clear through this study's surveys that some lithotripters across Canada are not running at full capacity, and that this is largely due to a provincial government cap on how frequently hospitals may bill for the use of a lithotripter. Stringent hospital budgets, which preclude around-the-clock machine staffing, have led to underutilized capital equipment. Indeed, substantial cost savings could materialize by offering lithotripsy to just 250 patients per year versus more invasive procedures (Mahoney 2001).
Interestingly, a retrospective evaluation of Ontario's Wait Time Strategy by the Institute for Clinical Evaluative Sciences (ICES) showed that while targeting and improving wait times for key therapies showed moderate success, the wait times of other elective surgeries were also not negatively affected (Paterson et al. 2007). Further, the Cardiac Care Network of Ontario – a provincewide registry that identifies regional disparities in access to cardiac care – has since 2005 decreased wait times for cardiac bypass and catheterization by up to 32%, by coordinating provincewide care and making it easier for patients who face longer waits to get care outside their local region (CIHI 2006). The federal and provincial governments must consider supporting patients who are willing to travel to other provinces for timely healthcare.
Third, it is notable that the data collected in this study were challenging to obtain from ESWL facilities and healthcare organizations. Without easily accessible wait-time information, patients lack the opportunity to decide whether they can travel for more timely treatment. Only a patchwork of information is available to Canadians regarding wait times. In fact, the vast majority of citizens and physicians would value "an interprovincial fund that would pay for patients to be sent to different Canadian jurisdictions for care when the wait in their home jurisdiction exceeds the benchmark for their procedure" (Sylvain 2006), and at least 20% of the population reports a willingness to travel for expedited waits (Geddes 2005). Coordinating care across and between provinces may help decrease wait times.
Conclusion
The process of shortening wait times is unavailing until it is publicly reported and on the political agenda. From a national perspective, the five priority areas of Canada's Wait Time Alliance must be expanded to include highly indicated, morbidity-reducing procedures for which there are often long waits, like ESWL. Within publicly funded healthcare systems, where wait times for elective surgery are a matter of morbidity, patients need access to this information so that they may make informed decisions about their healthcare.
Besoin de lithotritie : accessibilité et portabilité des services de santé au Canada
Résumé
Contexte : La lithotritie à ondes de choc électrohydraulique (LOCE) constitue une modalité de traitement indiquée, ambulatoire et non invasive pour les calculs rénaux. La LOCE n'est pas disponible dans tous les centres urbains et plusieurs Canadiens doivent soit se déplacer, parfois hors de leur province, soit attendre pour recevoir le traitement. Nous avons voulu évaluer la variabilité de l'accès au traitement par LOCE.
Méthode : Nous avons établi la liste complète des centres de LOCE au Canada et nous avons communiqué avec chacun d'eux, en 2011, pour savoir quel était le temps d'attente, les frais pour les patients qui venaient d'une autre province ainsi que le rôle et les responsabilités du médecin orienteur.
Résultats : Nous avons communiqué avec les 23 centres de LOCE au Canada (un taux de réponse de 100 %). Le temps d'attente pour les procédures de LOCE non urgentes variait d'un jour à plus d'un an, la moyenne étant de 8,4 semaines (avec un écart type de 16,76 semaines). Aucun centre ne refusait les patients d'autres provinces, cependant cinq d'entre eux déconseillaient les déplacements vers leurs installations en raison de longs temps d'attente. Aucun centre n'exigeait de frais supplémentaires pour les patients d'autres provinces. Dix installations (43 %) exigeaient une consultation supplémentaire auprès d'un de leurs urologues avant d'accorder un rendez-vous. Douze centres (52 %) ont indiqué que le temps d'attente pouvait être réduit si le médecin orienteur intervenait au nom du patient. Nous avons communiqué de nouveau avec cinq centres un an plus tard, soit en 2012, et les résultats étaient similaires.
Interprétation : Au Canada, il y a une variation marquée dans les temps d'attente pour la LOCE, mais il y a peu d'obstacle pour obtenir les soins. L'intervention des médecins pourrait aider à réduire l'attente des patients.
Appendix A
Telephone Interview Script
SCENARIO A/PATIENT LIVES INSIDE THE PROVINCE
Hi there, I have kidney stones, and my doctor has indicated that I need lithotripsy for them. I have a number of questions that I would like to ask.
- When is the earliest you can book me for a treatment?
- What do I need my doctor to do to book the appointment?
- Is there anything he can to do get my lithotripsy appointment sooner?
I need to confirm with my family and work schedule before I can book an appointment. But thank you very much for your time, have a nice day.
SCENARIO B/PATIENT LIVES OUTSIDE THE PROVINCE
Hi there, I have kidney stones, and my doctor has indicated that I need lithotripsy for them. I have a number of questions that I would like to ask.
1. Although I live outside your province, the waiting list is very long here. My sister lives near your centre and has agreed to let me stay with her. Can I come to your centre for lithotripsy? Y/N
2. If N:
Why not? Is it a policy that you don't take people from outside the province? What would I need to do to get lithotripsy in your province?
3. Is there anything he can to do get my lithotripsy appointment sooner?
I need to confirm with my family and work schedule before I can book an appointment. But thank you very much for your time, have a nice day.
About the Author(s)
Katrina L. Piggott, BHSc, MD, Resident, Department of Medicine, McMaster University, Hamilton, ON
Chaim M. Bell, MD, PhD, Department of Medicine, Mount Sinai Hospital, Faculty of Medicine and Institute of Health Policy, Management and Evaluation, University of Toronto, Toronto, ON
Correspondence may be directed to: Chaim M. Bell, MD, PhD, Mount Sinai Hospital, 600 University Ave., Ste. 433, Toronto, ON M5G 1X5; tel.: 416-586-4800, ext. 2583; e-mail: cbell@mtsinai.on.ca.
References
Auge, B.K. 2002. "Surgical Management of Urolithiasis." Endocrinology and Metabolism Clinics of North America 31: 1065–82.
Australian Institute of Health and Welfare (AIHW). 2010. "Australian Hospital Statistics 2008–2009 at a Glance." Health Service Series no. 37. Cat. no. HSE 89. Canberra: Author.
Barua, B., M. Rovere and B.J. Skinner. 2011. "Waiting Your Turn: Wait Times for Health Care in Canada." Studies in Health Policy. Vancouver: Fraser Institute.
Canadian Association of Radiologists (CAR). 2000. "Outdated Radiology Equipment: A Diagnostic Crisis." Special ministerial briefing. St-Laurent, QC: Author.
Canadian Coordinating Office for Health Technology Assessment (CCOHTA). 2001. "Lithotriper Machines in Canadian Hospitals." Ottawa: Canadian Agency for Drugs and Technologies in Health. Retrieved October 1, 2013. <http://www.cadth.ca/media/pdf/litho_report_01.pdf>.
Canadian Institute for Health Information (CIHI). 2006. "Waiting for Health Care in Canada: What We Know and What We Don't Know." Retrieved October 1, 2013. <https://secure.cihi.ca/estore/productSeries.htm?pc=PCC311>.
Canadian Institute for Health Information (CIHI). 2008. Medical Imaging in Canada, 2007. Retrieved October 1, 2013. <https://secure.cihi.ca/free_products/MIT_2007_e.pdf>.
Commission on Social Determinants of Health (CSDH). 2008. Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health. Final Report. Geneva: World Health Organization. Retrieved October 1, 2013. <http://www.who.int/social_determinants/thecommission/finalreport/en/index.html>.
Esmail, N. 2008. "How Good Is Canada's Medical Technology Inventory?" Fraser Alert. Vancouver: Fraser Institute. Retrieved October 1, 2013. <http://www.fraserinstitute.org/research-news/display.aspx?id=13098>.
Esmail, N., and M. Walker. 2008. How Good Is Canadian Health Care? Vancouver: Fraser Institute. Retrieved October 1, 2013. <http://www.fraserinstitute.org/research-news/display.aspx?id=13104>.
Fergusson, K. 2002. "Medical High Tech Inventory Increased 45% Since 1997." Ottawa: Canadian Agency for Drugs and Technologies in Health. Retrieved October 1, 2013. <http://www.cadth.ca/en/media-centre/2002/medical-high-tech-inventory-increased-45-since-1997>.
Geddes, J. 2005. "Bypassing Your Doctor: Can the Web Fix the Wait-Time Crisis, and Ultimately Even Save Medicare?" Maclean's. Retrieved October 1, 2013. <http://www.macleans.ca/science/health/article.jsp?content=20051017_113453_113453>.
Harriman, D., W. McArthur, M. Zelder and J. Alexander. 1999. The Availability of Medical Technology in Canada: An International Comparative Study. Vancouver: Fraser Institute. Retrieved October 1, 2013. <http://www.fraserinstitute.org/research-news/research/display.aspx?id=13484>.
Karlsen, S.J., J. Renkel, A.R. Tahir and A. Angelsen. 2007. "Extracorporeal Shockwave Lithotripsy versus Ureteroscopy for 5- to 10-mm Stones in the Proximal Ureter. Prospective Effectiveness Patient-Preference Trial." Journal of Endourology 21(1): 28–33. doi: 10.1089/end.2006.0153.
Mahoney, J.E. 2001. "Lithotripsy Comes to Ottawa… at Last." Letter. Canadian Medical Association Journal 164(13). Retrieved October 1, 2013. <http://www.cmaj.ca/cgi/content/full/164/13/1833>.
Ministry of Health and Long-Term Care (MOHLTC). 2011. "Ontario Wait Time Strategy." Retrieved October 1, 2013. <http://www.health.gov.on.ca/en/public/programs/waittimes/>.
Moe, O.W. 2006. "Kidney Stones: Pathophysiology and Medical Management." Lancet 367(9507): 333–44.
Nabi, G., P. Downey, F. Keeley, G. Watson and S. McClinton. 2007. "Extra-Corporeal Shock Wave Lithotripsy (ESWL) versus Ureteroscopic Management for Ureteri Calculi." Cochrane Database of Systematic Reviews 1. Art. no.: CD006029. doi: 10.1002/14651858.CD006029.pub2.
Organisation for Economic Co-operation and Development (OECD). 2011. "Health Care Resources: Medical Technology." Retrieved October 1, 2013. <http://stats.oecd.org/index.aspx?DataSetCode=HEALTH_STAT>.
Otsubo, T., Y. Imanaka, J. Lee and K. Hayashida. 2011. "Evaluation of Resource Allocation and Supply–Demand Balance in Clinical Practice with High-Cost Technologies." Journal of Evaluation in Clinical Practice 17(6): 1114–21. doi: 10.1111/j.1365-2753.2010.01484x.
Paterson, J.M., J.E. Hux, J.V. Tu and A. Laupacis. 2007. The Ontario Wait Time Strategy: No Evidence of an Adverse Impact on Other Surgeries. Investigative report. Toronto: Institute for Clinical Evaluative Sciences. Retrieved October 1, 2013. <http://www.ices.on.ca/webpage.cfm?site_id=1&org_id=31&morg_id=0&gsec_id=0&item_id=4185>.
Revah, G. and C. Bell. 2007. "Shopping for High Technology Treatment in Another Province." Healthcare Policy 2(4): 49–55.
Rublee, D.A. 1989. "Medical Technology in Canada, Germany and the United States." Health Affairs 8(3): 178–81. doi: 10.1377/hlthaff.8.3.178.
Sanmartin, C., F. Gendron, J.-M. Berthelot and K. Murphy. 2004. "Access to Health Care Services in Canada, 2003." Ottawa: Statistics Canada. Retrieved October 1, 2013. <http://publications.gc.ca/Collection/Statcan/82-575-X/82-575-XIE2003001.pdf>.
Srisubat, A., S. Potisat, B. Lojanapiwat, V. Setthawong and M. Laopaiboon. 2009. "Extracorporeal Shock Wave Lithotripsy (ESWL) versus Percutaneous Nephrolithotomy (PCNL) or Retrograde Intrarenal Surgery (RIRS) for Kidney Stones." Cochrane Database of Systematic Reviews 4. Art. no.: CD007044. doi: 10.1002/14651858.CD007044.pub2.
Steering Committee for the Review of Government Service Provision (SCRGSP). 2011. National Partnership Agreement on the Elective Surgery Waiting List Reduction Plan: Period 3 Performance Report. Canberra: Australian Government Productivity Commission. Retrieved October 1, 2013. <http://www.pc.gov.au/gsp/national-partnership/elective-surgery>.
Sylvain, M. 2006 (August 22). "MDs Want Wait-Time Talk Translated into Action: Survey." Medical Post.
United Medical Systems (UMS). 2010. "Advanced Mobile Lithotripsy Services." Retrieved October 1, 2013. <http://www.ums-usa.com/uroLitho.html>.
Wait Time Alliance (WTA). 2011. "Time Out! Report Card on Wait Times in Canada June 2011." Wait Time Alliance Report Card. Retrieved October 1, 2013. <http://www.waittimealliance.ca/media/2011reportcard/WTA2011-reportcard_e.pdf>.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed