
Insights
Taking an aggressive stance on EMRs: lessons from the US and UK
The US has an aggressive approach to ‘meaningful use’ of electronic medical record (EMR) technology to deliver better patient outcomes. The UK takes it a step further. Should Canada follow suit?
Canada has spent over $10 billion towards the implementation of electronic health record (EHR) technology, according to the Auditor General’s report in 20101. Much of this money has been spent on developing the infrastructure to store, retrieve, and share health information across the country. However, considerably less government funds have been used to incentivize the use of advanced electronic medical records (EMRs) by primary care providers.
Canada ranked second-last among 10 developed countries in EMR use in a 2012 survey by the Commonwealth Report2. Only 10% of physicians in Canada said they used EMRs with multifunctional health information technology (HIT) capacity (“multifunctional HIT capacity” is defined for the purpose of the Commonwealth Report survey as at least two electronic functions for each of order entry management, generating patient information, generating panel information, and routine clinical decision support).
Figure 1:
Doctors with Electronic Medical Records and Multifunctional Health IT Capacity

Source: Commonwealth Report, 2012
Canada’s low EMR adoption rate may in part be related to the past focus on subsidizing the purchase and implementation of EMR technology typically with a one-time payment of incentive dollars. Healthcare providers were encouraged to implement EMR technology; however the meaningful use of technology or improved patient outcomes as a result of technology were not linked to incentive dollars in most provinces.
In contrast, the United States has taken an aggressive and standardized approach towards the meaningful use of EMR technology: incentives and penalties are significant, adoption is mandatory, and payments are tied to the meaningful use of technology. A three-stage Meaningful Use incentive program, with increasing levels of HIT functionality and increasing emphasis on patient outcomes, was established at the federal level and put into effect in 2011.
To be considered a “meaningful user”, physicians and hospitals must consistently use a growing list of advanced HIT functions such as e-prescribing, generating patient reminders for preventative care, allowing patients to access their health information electronically, and using specific clinical decision support functions. Over $18 billion in financial incentives were set aside and all eligible providers and hospitals across the US were then given advanced notice (up to four years) to prepare for the impending changes3.
In another notable contrast to Canada, the financial incentives for US physicians and hospitals are significant over the 6 year program: an average physician can receive up to $44,000 in incentives for Medicare patients or up to $63,750 in incentives for Medicaid patients, and hospitals can potentially receive millions of dollars4.
Furthermore, the financial incentives were accompanied by an announcement that failure to meet the Meaningful Use requirements would result in reductions in fee for service remuneration rates starting in 2015. The payment adjustment is 1% and is cumulative for every consecutive year the physician fails to meet the requirements of Meaningful Use. These reductions would have an ongoing impact on physician incomes, making adoption of technology a very compelling investment. Implicit in these rate reductions is recognition that care delivered without information tools is no longer the standard of practice and hence is not as valuable to the public payer.
The US has experienced a significant increase in EMR use since the Meaningful Use program began in 2011. In 2012, 69% of US primary care physicians reported using EMRs (compared to 56% of Canadian physicians) and 27% of US physicians reported using EMRs with multifunctional HIT capacity (compared to 10% of Canadian physicians)2.
Figure 2:
Percentage of office-based physicians with any EHR system
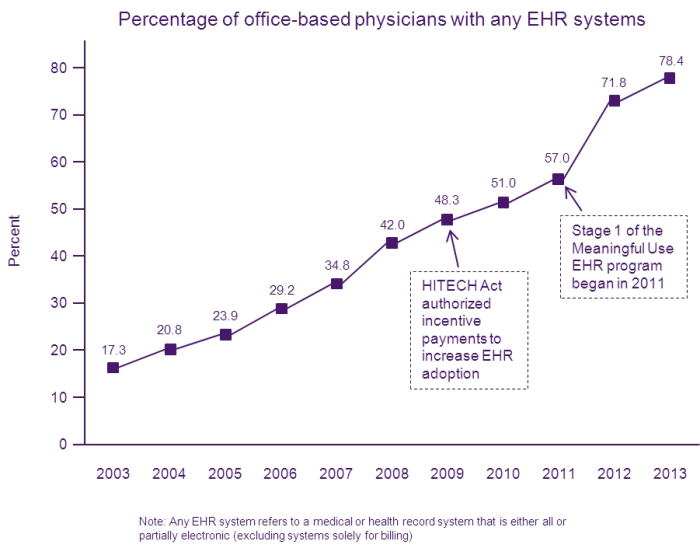
Source: NCHS Data Brief, No. 143, January 20145
In the United Kingdom, 97% of physicians reported using EMRs in their practice in 2012 and the UK had among the highest EMR adoption rates out of the 10 countries surveyed in the Commonwealth Report2. The UK has gone a step further than the US by linking incentive payments to quality metrics (that require advanced EMR functionality to generate and report the metrics). The payments tied to the Quality and Outcomes Framework (QOF) established in 2004 now account for more than 20% of a family practitioners’ income. Moreover, England can deny payment to primary care providers that do not meet EMR technology standards.
Given the experience of the US and UK, Canada should consider moving away from subsidizing the purchase of EMR systems, and instead focus more on incentives for the advanced use of multifunctional EMRs and improved patient outcomes. Providers who are unable to electronically capture and report patient outcomes should be ineligible for incentives or subject to reduced remuneration similar to the US model. This shift is likely to increase adoption rates and the use of advanced multifunctional capacity of EMRs.
Such incentives are an opportunity to focus providers on priority areas, such as diabetes management, supported by national performance targets. Successful implementation would require significant advance notice to give providers enough time to change their practice to meet performance requirements. Studies, such as Cebul et al. (2011), have demonstrated the benefits of meaningful EMR use on patient outcomes for diabetes measures6. Conversely, studies such as Crosson et al. (2012), have shown that superficial use of an EMR, without adjusting work processes and utilizing advanced functions such as clinical decision support, does not lead to better care7.
Broad adoption and clinical use of advanced EMR functions is a key driver of improved delivery of primary care and better patient outcomes. Closing the adoption gap with other developed nations is key to maintaining a world class health system in Canada.
- Electronic Health Records in Canada, An Overview Of Federal and Provincial Audit Reports, April 2010. Office of the Auditor General of Canada. Retrieved , from https://www.oag-bvg.gc.ca/internet/docs/parl_oag_201004_07_e.pdf
- Schoen, C., & Osborn, R. The Commonwealth Fund 2012 International Health Policy Survey of Primary Care Physicians Chartpack. 2012 International Symposium on Health Care Policy.
- About the HITECH Act. Retrieved from https://www.hitechanswers.net/about/about-the-hitech-act-of-2009/
- Schilling, B. The Federal Government Has Put Billions into Promoting Electronic Health Record Use: How Is It Going?. Commonwealth Fund: Quality Matters, June/July 2011. Retrieved , fromhttps://www.commonwealthfund.org/Newsletters/Quality-Matters/2011/June-July-2011/In-Focus.aspx
- Hsiao, C., & Hing, E. Use and Characteristics of Electronic Health Record Systems Among Office-based Physician Practices: United States, 2001–2013. NCHS Data Brief, 143. Retrieved , from https://www.cdc.gov/nchs/data/databriefs/db143.pdf
- Cebul, R., T.E. Love, A.K. Jain and C.J. Hebert. 2011. “Electronic Health Records and Quality of Diabetes Care”. New England Journal of Medicine 365:9.
- Crosson, J., Ohman-Strickland, P., Cohen, D., Clark, E., & Crabtree, B. Typical Electronic Health Record Use in Primary Care Practices and the Quality of Diabetes Care. Annals of Family Medicine, 10. Retrieved , fromhttps://www.annfammed.org/content/10/3/221.full
About the Author(s)
Dr. Michael Guerriere is Chief medical officer, TELUS Health, Justin Kim is Senior consultant, TELUS HealthAcknowledgment
Reprinted with permission from from IV Newsletter Spring 2014
Comments
Hitesh wrote:
Posted 2019/11/24 at 03:03 PM EST
Great article. Rightly said - Incentivising and penalties are the way forward.
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed