
HealthcarePapers
Relational Work Is the Work: Virtual Healthcare Transformation for Rural, Remote and First Nations Communities in British Columbia
Abstract
The healthcare crisis across unceded First Nations' territories in rural, remote and Indigenous communities in British Columbia (BC) is marked by persistent barriers to accessing care and support close to home. This commentary describes an exceptional story of how technology, trusted partnerships and relationships came together to create an innovative suite of virtual care programs called “Real-Time Virtual Support” (RTVS). We describe key approaches, learnings and future considerations to improve the equity of healthcare delivery for rural, remote and First Nations communities. The key lessons include the following: (1) moving beyond a biomedical model – the collaboration framework for health service design incorporated First Nations' perspective on health and wellness; (2) relational work is the work – the RTVS collaboration was grounded in building connections and relationships to prioritize cultivating trust in the partnership over specific outputs; and (3) aligning to the core values of co-creation – working from a commitment to do things differently and applying an inclusive approach of engagement to integrate perspectives across different sectors and interest groups.
Contextualizing the Healthcare Crisis
Canada is in the midst of a healthcare crisis, which is exacerbated in populations living in rural, remote and First Nations communities (Greenwood et al. 2018; Sibley and Weiner 2011; Wilkinson et al. 2015). There are well-documented disparities between rural and urban populations when it comes to access to health services and overall health outcomes, which are influenced by the determinants of health and a number of other factors, including expansive geography, transportation, climate hazards and provider recruitment and retention (Hanlon and Halseth 2005; Smith et al. 2019a, 2019b). These factors are often more prevalent in First Nations communities and combined with unique challenges with respect to the health system and accessing health services, including impacts of colonialism (historical and current day), systemic racism, remoteness, jurisdictional gaps and a lack of cultural safety integration from providers and the broader health system. First Nations leaders have been calling for the delivery of culturally safe health services closer to home for years (FNHA n.d.c).
Virtual health provides an opportunity to improve access to healthcare across time and/or distance. Several smaller-scale virtual health initiatives have been implemented in British Columbia over the past 10 years, such as the Carrier Sekani Family Services Primary Care model (Holyk et al. 2017), CODI (BC Rural Centre 2023), Robson Valley Virtual Care Pilot project (UBC Digital Emergency Medicine 2018) and telemedicine for thoracic oncology care (Humer and Campling 2017). Despite the growing evidence of their effectiveness in improving access and reducing health disparities, wider-scale implementation and spread has been slow.
This commentary describes a remarkable story of how technology, trusted partnerships and relationships came together to create the fertile ground to operationalize an innovative suite of virtual care programs called “Real-Time Virtual Support” (RTVS). RTVS is a suite of patient-facing and peer-to-peer virtual physician services focused on addressing the health equity gaps in rural, remote and First Nations communities. We will discuss approaches, key learnings and future directions for translating similar work in other rural, remote and First Nations communities across Canada.
Defining “Edge” Communities
The healthcare crisis in rural, remote and First Nations communities in British Columbia (BC) is marked by a lack of doctors, culturally unsafe care for Indigenous Peoples and persistent barriers in accessing care and support close to home, especially for client-patients and providers living and working on the edges of the healthcare system. The BC Ministry of Health released the Rural, Remote, First Nations and Indigenous COVID-19 Response Framework that identified 147 high-priority communities characterized by their geographic rurality, isolation from regular service centres, need for reliable access to physicians, cost of transportation and governance in health service delivery (BC Ministry of Health 2020). In this paper, “edge” communities refer to communities that have systematically been pushed to the edges of healthcare through policies and decision making that do not adequately assess or support the needs of their populations, creating conditions that allow these communities to experience poor health outcomes. This paper focuses on those pushed to the edges of healthcare based on being a rural, remote or Indigenous community.
It is important to note that, in many cases, the edges of healthcare in Canada are a legacy of the larger colonial process that has created ongoing inequities in access to care and related health outcomes. While many First Nations communities are on the edges of healthcare, their people and territories have been, are and always will be the centres for their un-extinguishable rights and title, as well as their distinct Indigenous ancestry, language, culture and heritage. In our experience of developing a virtual health program, we challenge the notion that the edge is a place of marginalization and instead reposition the edge as a place of creativity, vibrancy and innovation where strong, relational partnerships are fostered.
Access for First Nations People
As highlighted in the introduction, while rural, remote and First Nations communities experience many similar barriers to health equity, First Nations people experience additional and unique barriers to accessing healthcare. As expressed by the First Nations Health Council, “since time immemorial, the Indigenous Peoples of the territories currently known as British Columbia, knew how to live in healthy ways” (First Nations Health Council 2023: 15). Among the many atrocities, settler colonialism separated people from the land, undermined the governance and self-determination of First Nations people and weaponized sites of learning and healthcare in the form of residential schools and Indian hospitals. While these schools and hospitals have closed, the legacies of systemic racism, inaccessible and unsafe care and the dismissal of cultural practices and holistic approaches to wellness are persistent and well documented throughout the healthcare system in BC (Turpel-Lafond 2020).
The Truth and Reconciliation Calls to Action (Truth and Reconciliation Commission of Canada 2015), the United Nations Declaration on the Rights of Indigenous Peoples (United Nations 2007) and the In Plain Sight report (Turpel-Lafond 2020) – all outline in detail specific actions required to address the harms of systemic racism and colonialism. At the core of many of these calls to action is the need for First Nations to be supported in leading and determining their health needs, policies, service designs and service delivery. It is essential to ensure that care at all levels of acuity is rooted in traditional wellness, designed through the lenses of health equity and founded on systemic cross-cutting supports such as quality, cultural safety and trauma-informed care (First Nations Health Council 2023).
One way that First Nations people in BC have reclaimed governance over their health systems is through the establishment of the First Nations Health Authority (FNHA), which serves as the health and wellness partner to over 200 diverse First Nations communities and citizens across BC. It is important to note that the work of the FNHA does not replace the role or services of the Ministry of Health and regional health authorities. The BC Ministry of Health remains responsible for ensuring that appropriate, cost-effective, timely and high-quality health services are available for all British Columbians, including Indigenous Peoples. In 2013, the FNHA took on the responsibility for the programs and services formerly delivered by Health Canada and has been working to address service gaps and enhance cultural safety through new partnerships, collaborations, health systems innovation and the reform and redesign of health programs and services (FNHA n.d.a.).
Essential Partnerships
One of the FNHA's key partners to help move this forward in the rural and remote context has been the Rural Coordination Centre of BC (RCCbc). The RCCbc is a network organization of hundreds of people – rural physicians and other healthcare providers, healthcare administrators, community members, policy makers, educators, researchers and non-profit and business leaders – guided by the principles of cultural safety and humility that aim to improve healthcare outcomes in rural, remote and First Nations communities. The RCCbc and the FNHA have developed a strong, collaborative relationship over time. In 2019, they co-coordinated and co-hosted the Provincial Health Care Partners Retreat, which focused on how all healthcare partners can enable system transformation in a culturally safe and inclusive way (Markham et al. 2021). When partners identified rural patient transportation, virtual health and cultural safety as areas of interest for system transformation, the RCCbc and the FNHA worked in coordination to bring multiple stakeholders together to address these key issues. As the two organizations began to work more closely and align their work on numerous fronts, they formalized their partnership by signing a memorandum of understanding in 2019 that recognized the commonalities and distinctions in serving the healthcare needs of First Nations and rural and remote communities (FNHA 2019).
RTVS: Implementation to Impact
The close relationship between the FHNA and the RCCbc worked to the advantage of all when the COVID-19 pandemic started. The trusted partnership allowed for the rapid coordination, development and deployment of net-new patient-facing and provider-facing virtual supports, collectively known as RTVS. Other founding RTVS collaborative organizations include the BC Ministry of Health, Provincial Health Services Authority, Providence Health Care, BC Emergency Medicine Network and the UBC Department of Emergency Services.
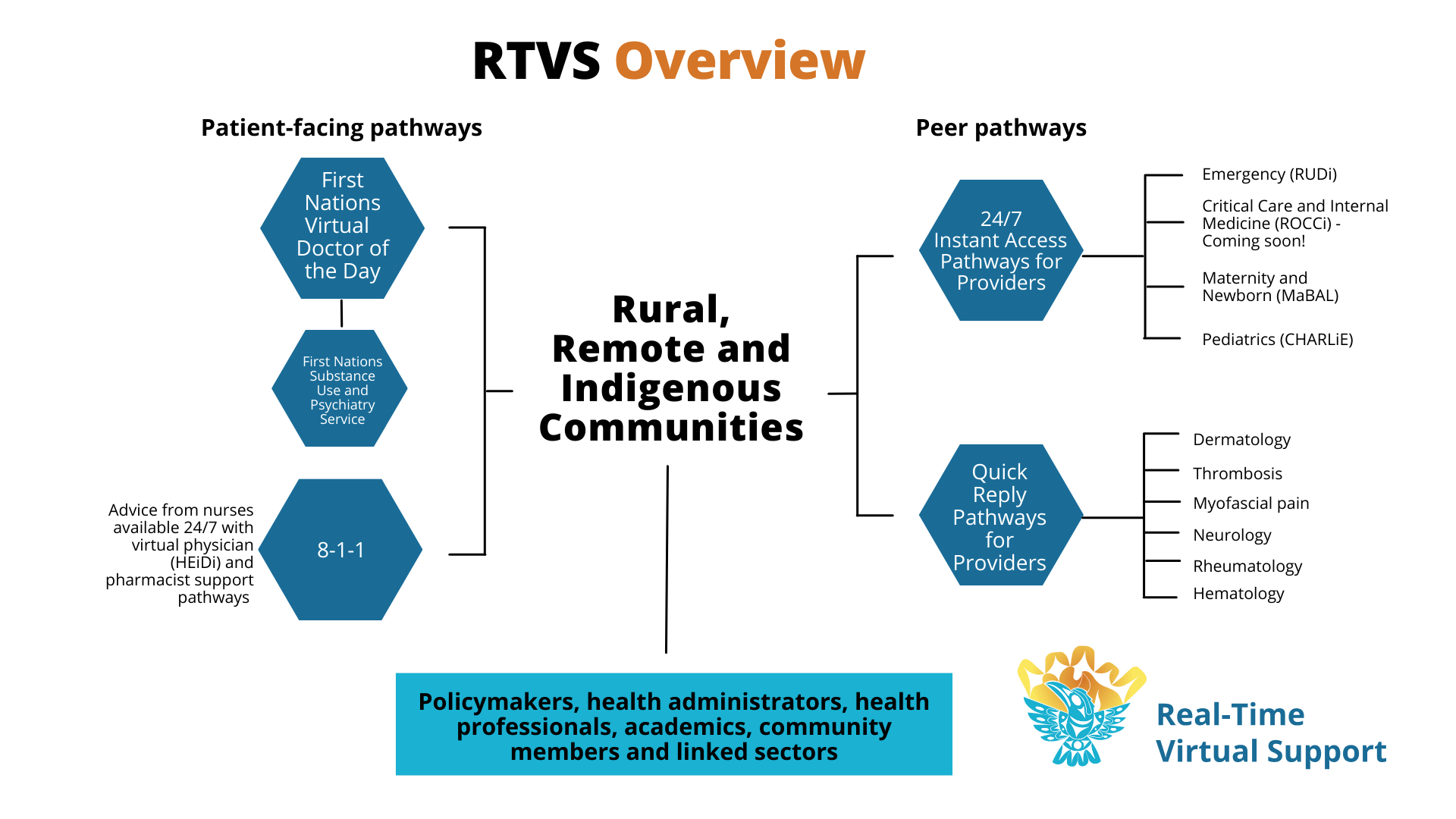
RTVS has been described previously in published literature (Novak Lauscher et al. 2023a; 2023b) and on the RCCbc's (n.d.) website. In brief, RTVS has two main types of services: (1) peer-to-peer support for urgent and non-urgent situations, including case consultations, second opinions, ongoing patient management, transport coordination, point-of-care ultrasound and simulation-based training; and (2) direct-to-patient care that offers BC citizens and First Nations community members direct virtual access to health professionals. RTVS utilizes simple and accessible technology – such as Zoom and phone – to connect patients and providers to virtual physicians. Figure 1 outlines the three patient-facing, four instant access and six quick-reply peer-to-peer pathways.
{kind=link}

There are now over 250 healthcare providers within the RTVS network, with more than 15 medical disciplines. Providers within the network are supported and connected with their peers, receive cultural safety training and further contribute to accessible healthcare by ensuring that patients feel respected in their consultations and community environments. Collectively, the RTVS pathways have served over 50,000 clients, expanding the reach of physician services across the province to serve 57% of the initially identified edge communities while addressing some of the most pressing needs in the BC health system, specifically the need for access to family physicians and substance use and psychiatry services (S. Cressman, personal communication, September 26, 2023). The First Nations Virtual Doctor of the Day and Substance Use and Psychiatry Service (https://www.fnha.ca/what-we-do/ehealth/virtual-substance-use-and-psychiatry-service) has had high usage with high rates of clients reporting that the services feel culturally safe. The peer-to-peer pathways show promise of reversing inequities in access to care by primarily serving patients in the lowest-income groupings. For more information on program impacts, The Edge of Care, a short film, tells the story of RTVS from the perspective of client-patients, rural providers and supporting physicians (Rothman 2023).
Through the dedication and innovative thinking of the group of partners, RTVS has become a beacon of hope in the landscape of healthcare transformation, presenting both the capacity to offer culturally safe care closer to home and in a way that is meaningful to both patients and the healthcare system. However, virtual services on their own are not sufficient to adequately close equity gaps. While investments in virtual tools, technology and infrastructure are essential, true transformation requires a paradigm shift that commits to doing things differently to reposition edge communities as the centre from which our solutions flow. Included below are our reflections on what enabled this paradigm-shifting transformation for RTVS collaborative partners.
Lessons Learned and Recommendations
The three lessons learned reflect some of these core values and commitments and are what, we believe, were the foundational elements that enabled the successful leveraging of digital tools to close equity gaps at the edges of the healthcare system.
Moving beyond a biomedical model: First Nations' perspective on health and wellness
Figure 2 represents the First Nations' perspective on health and wellness. The original image was created based on research, feedback and ideas gathered from BC First Nations over the past few years and from traditional teachings and approaches shared by BC First Nations healers and Elders at gatherings convened by the FNHA and its predecessor, the First Nations Health Society (FNHA n.d.b.). Cultural and traditional healing and wellness approaches are at the foundation of health transformation work with First Nations people.

One framework for facilitating this kind of thinking that has resonated with RTVS collaborators is that of “two-eyed seeing,” a theoretical framework first coined by Mi'kmaw Elder Albert Marshall (Bartlett et al. 2012). In the context of health systems, this means shifting from a western, biomedical approach as the default to a “two-eyed seeing” approach that brings together the best of western and traditional perspectives and makes space for grounding the work within the specific context of the First Nations community that one is working with (Bartlett et al. 2012).
Relational work is the work
RTVS collaborative relationships are guided by the value and importance of connection and relationship building to cultivate trust in the partnership, in alignment with First Nations' perspective on health and wellness. While trust building takes time and commitment, when it is established and maintained it acts as an enabler for successful long-term planning and rapid response in times of crisis. In the case of RTVS collaborators, the pre-existing relationships allowed for the rapid development and deployment of the RTVS pathways that addressed acute and long-standing healthcare gaps for rural, remote and First Nations people. Furthermore, maintaining strong relational partnerships creates conditions that allow for the sometimes-difficult conversations required to enable cultural safety within healthcare services. Some common practices in the RTVS collaborative at meetings and gatherings big and small is taking time to connect as human beings before entering our work as human doings (the roles and titles we take on in our work) and grounding in gratitude even as we continually assess what needs to be improved. Simple practices like these, when combined with strong commitments to improve cultural safety and humility, foster trust so that when mistakes are made the group feels empowered and supported to name them and address them.
Aligning with the core values of co-creation
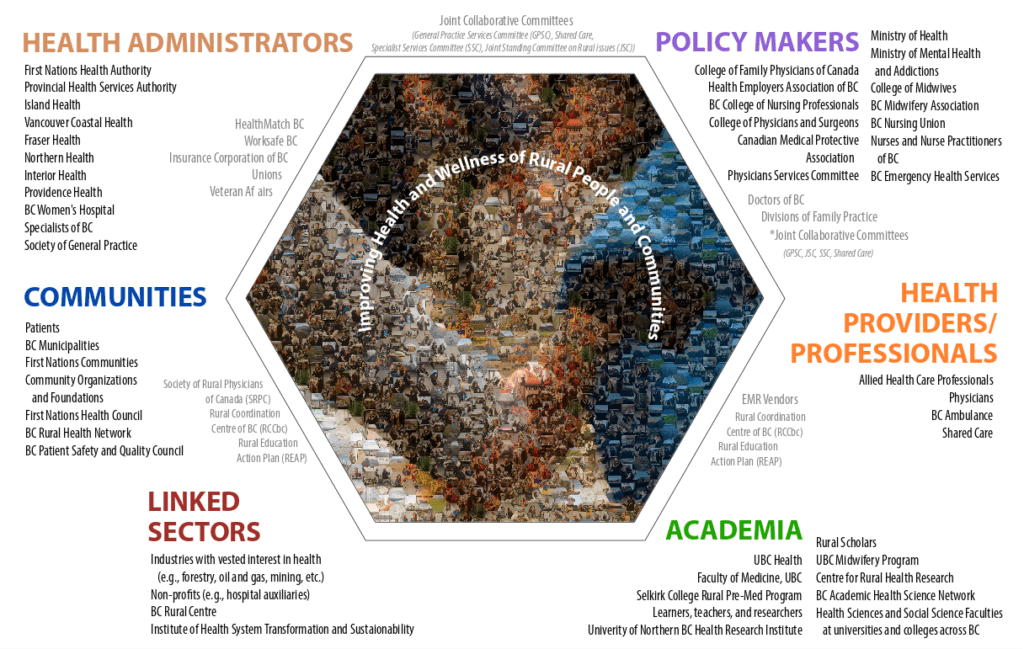
Working from a commitment to do things differently and a foundation of trust that acknowledged both the shared challenges of rural, remote and First Nations communities and the distinct challenges faced by First Nations people also created conditions that allowed for strong co-creation. Using the Partnership Pentagram Plus framework and inclusive facilitation approaches such as appreciative inquiry (Markham et al. 2021), the RTVS collaborative has been able to engage and integrate perspectives across sectors and interest groups (see Figure 3). One example of this in action was the provincial gathering co-hosted by the FNHA and the RCCbc. As described by Markham et al. (2021, 2022), participants were asked to contribute from their perspective rather than being asked to be representative of any particular group. By deep listening and valuing the person and perspective over position and privilege, a positive and inspiring approach to change resulted. As a result, a strong community voice was heard in dialogue with provincial healthcare leaders, resulting in co-created and practical solutions and next steps.

In the words of a patient partner, the meaning of “co-creation” is as follows:
Co-creation involves First Nations, rural and remote patients collaborating as equal partners with healthcare providers from the start, identifying challenges and jointly developing strategies for equitable and improved health outcomes. (John Grogan)
While there are many factors that led to the creation and success of RTVS, we believe, the following three elements were the biggest facilitators of tangible change. We share these reflections in the hope of inspiring other healthcare professionals and policy makers to delve into the many possibilities of what it can look like to pursue transformative virtual healthcare. Given that the healthcare system has not served First Nations people and rural and remote communities adequately, there remains a need to do things differently to address the systemic barriers that created and maintain edge communities. To this end, we are guided by several strategic questions for ourselves and others to continue further efforts to address these equity gaps:
- Growth and governance: RTVS needs to be fused to the priorities of First Nations communities, leadership and the FNHA partner teams moving forward. Simultaneously, rural non-Indigenous partners, such as the RCCbc, need to be strong co-designers/creators and managers moving into the future. How can the future governance and operational structures and functions of RTVS be shaped to meet these needs in a sustainable way?
- Succession and continuity planning: RTVS is a strong living example of doing things differently to address equity, cultural safety and access issues in a substantive way. How can the next chapter of RTVS ensure relational continuity and value alignment that will allow for the continued leveraging of its historic successes while evolving to continue to address the remaining and long-standing inequities?
- Maintaining strong patient engagement: Client-patient involvement in health system transformation is critical to successful initiatives. We need to continue to embrace the paradigm of community members as co-creators/designers and leaders in the RTVS story. In what other ways can patients be involved in future RTVS developments to ensure that new innovative care provision is carried out alongside and with client-patients?
Conclusion
If the context in which new tools are being applied remains the same, those tools are likely to reproduce the same conditions that perpetuate inequity. The RTVS story is fundamentally about people and relationships and not technology. It is a story about equity and the thoughtful and safe support of client-patients and providers, regardless of geographic location. Moving forward, our lessons learned indicate that this type of transformational work must remain focused and founded on authentic, trusting relationships that prioritize equity and cultural safety to enhance access to high-quality care and professional support. For RTVS, this means the program must remain attentive and true to the core values that were the genesis of the program while strengthening existing support pathways that serve First Nations, rural and remote communities. This will take us closer to the paradigm of a virtual hospital, which could open up whole new innovations and possibilities that must take into consideration the context of First Nations, rural and remote communities.
About the Author(s)
John Mah, BSc Pharm, MBA, Vice-President, First Nations Health Authority, Vancouver, BC
John Pawlovich, MD, UBC Chair in Rural Health, University of British Columbia, Vancouver, BC
Terri Aldred, BSc, MD, Executive Medical Director, First Nations Health Authority, Family Physician, Carrier Sekani Family Services, Vancouver, BC
Scott Graham, BEd, MA, Director of Operations and Planning, First Nations Health Authority, Vancouver, BC
Ray Markham, MB ChB, Executive Director, Rural Coordination Centre of BC, Vancouver, BC
Kim Williams, BScN, MScN, Networks Director, Rural Coordination Centre of BC, Vancouver, BC
Bob Woollard, MD, Professor, University of British Columbia, Associate Director, Rural Coordination Centre of BC, Vancouver, BC
John Grogan, Patient Partner, Valemount, BC
Dee Taylor, PhD, Corporate Director, Research, Interior Health, Eagle Bay, BC, Scientific Director, Rural Coordination Centre of BC, Vancouver, BC
Nelly D. Oelke, BScN, MN, PhD, Associate Professor, School of Nursing, UBC Okanagan, Kelowna, BC, Scientific Director, Rural Coordination Centre of BC, Vancouver, BC
Alison James, BSsH, MSc, Project Coordinator, Rural Coordination Centre of BC, Vancouver, BC
Melissa Stewart, BScH, MA, Senior Planning Lead, First Nations Health Authority, Vancouver, BC
Sonya Cressman, BSc, PhD, MBA, Evaluation Lead, Department of Emergency Medicine, University of British Columbia, Vancouver, BC
Arianna Hogan, BA, Executive Assistant, Rural Coordination Centre of BC, Vancouver, BC
Daniel Harper, BA, MA, Strategic Initiatives Lead, Rural Coordination Centre of BC, Vancouver, BC
References
Bartlett, C., M. Marshall and A. Marshall. 2012. Two-Eyed Seeing and Other Lessons Learned within a Co-Learning Journey of Bringing Together Indigenous and Mainstream Knowledges and Ways of Knowing. Journal of Environmental Studies and Sciences 2(4): 331–40. doi:10.1007/s13412-012-0086-8.
BC Ministry of Health. 2020, May 26. Rural, Remote, First Nations and Indigenous COVID-19 Response Framework. Retrieved September 26, 2023. <https://www2.gov.bc.ca/assets/gov/public-safety-and-emergency-services/emergency-preparedness-response-recovery/gdx/rural-and-remote-covid-19-response-framework.pdf>.
BC Rural Centre. 2023. CODI – New Rural BC Healthcare App. Retrieved September 26, 2023. <https://bcruralcentre.org/codi-new-rural-bc-healthcare-app/>.
First Nations Health Authority (FNHA). n.d.a. FNHA Overview. Retrieved September 26, 2023. <https://www.fnha.ca/about/fnha-overview>.
First Nations Health Authority (FNHA). n.d.b. First Nations Perspective on Health and Wellness. Retrieved September 26, 2023. <https://www.fnha.ca/Documents/FNHA_Our_Story.pdf>.
First Nations Health Authority (FNHA). n.d.c. Our Story. Retrieved February 6, 2024. <https://www.fnha.ca/what-we-do/medical-affairs-and-wellness-office/our-primary-care-programs>.
First Nations Health Authority (FNHA). 2019, Novmeber 14. FNHA Signs MOU With RCCbc to Promote Rural Health Collaboration. Retrieved September 26, 2023. <https://www.fnha.ca/about/news-and-events/news/fnha-signs-mou-with-rccbc-to-promote-rural-health-collaboration>.
First Nations Health Council. 2023. 10-Year Strategy on the Social Determinants of Health: A Framework for the Future: Reclaiming our Wellness. Remembering our Future. Retrieved September 26, 2023. <https://fnhc.ca/wp-content/uploads/2023/04/GWXII_Online_FINAL.pdf>.
Greenwood, M., S. De Leeuw and N. Lindsay. 2018. Challenges in Health Equity for Indigenous Peoples in Canada. The Lancet 391(10131): 1645–48. doi:10.1016/S0140-6736(18)30177-6.
Hanlon, N. and G. Halseth. 2005. The Greying of Resource Communities in Northern British Columbia: Implications for Health Care Delivery in Already-Underserviced Communities. The Canadian Geographer/Le Géographe Canadien 49(1): 1–24. doi:10.1111/j.0008-3658.2005.00077.x.
Holyk, T., J. Pawlovich, C. Ross and A. Hooper. 2017. The Role of Telehealth in Improving Continuity of Care: The Carrier Sekani Family Services Primary Care Model. British Columbia Medical Journal 59(9): 459–64.
Humer, M.F. and B.G. Campling. 2017. The Role of Telemedicine in Providing Thoracic Oncology Care to Remote Areas of British Columbia. Current Oncology Reports 19(8): 52. doi:10.1007/s11912-017-0612-7.
Markham, R., S. Graham, M. Hunt, G. Betkus, K. Williams, B. Woollard et al. 2022. Social Accountability in Practice: Breathing and Weaving Together to Build Relationships and Transform Rural Health Services. Social Innovations Journal 14(4).
Markham, R., M. Hunt, R. Woollard, N. Oelke, D. Snadden, R. Strasser et al. 2021. Addressing Rural and Indigenous Health Inequities in Canada through Socially Accountable Health Partnerships. BMJ Open 11(11): e048053. doi:10.1136/bmjopen-2020-048053.
Novak Lauscher, H., B. Blacklaws, E. Pritchard, E.J. Wang, K. Stewart, J. Beselt et al. 2023a. Real-Time Virtual Support as an Emergency Department Strategy for Rural, Remote, and Indigenous Communities in British Columbia: Descriptive Case Study. Journal of Medical Internet Research 25: e45451. doi:10.2196/preprints.45451.
Novak Lauscher, H., K. Stewart, R. Markham, J. Pawlovich, J. Mah, M. Hunt et al. 2023b. Real-Time Virtual Supports Improving Health Equity and Access in British Columbia. Healthcare Management Forum 36(5): 285–92. doi:10.1177/08404704231183177.
Rothman, Z. 2023. The Edge of Care [Film]. UBC Faculty of Medicine – Digital Solutions: Education – EdTech. Retrieved September 25, 2023. <https://www.youtube.com/watch?v=0YYMNtnBkis>.
Rural Coordination Centre of BC (RCCbc). n.d. Real-Time Virtual Support. Retrieved September 26, 2023. <https://rccbc.ca/initiatives/rtvs/>.
Rural Coordination Centre of BC (RCCbc). 2023a. RTVS Overview. Retrieved January 24, 2024. <http://rccbc.ca/wp-content/uploads/2023/12/RTVS-overview-diagram.png>.
{kind=link}
Rural Coordination Centre of BC (RCCbc). 2023b. Partnership Pentagram Plus. Retrieved January 24, 2024. <https://rccbc.ca/wp-content/uploads/2022/10/PPP-Mosaic-Graphic-1024x649-1.png>.
{kind=link}
Sibley, L.M. and J.P. Weiner. 2011. An Evaluation of Access to Health Care Services along the Rural-Urban Continuum in Canada. BMC Health Services Research 11(1): 20. doi:10.1186/1472-6963-11-20.
Smith, J.G., C.M. Plover, M.C. McChesney and E.T. Lake. 2019a. Isolated, Small, and Large Hospitals Have Fewer Nursing Resources than Urban Hospitals: Implications for Rural Health Policy. Public Health Nursing 36(4): 469–77. doi:10.1111/phn.12612.
Smith, S., J. Sim and E. Halcomb. 2019b. Nurses' Experiences of Working in Rural Hospitals: An Integrative Review. Journal of Nursing Management 27(3): 482–90. doi:10.1111/jonm.12716.
Truth and Reconciliation Commission of Canada. 2015. Truth and Reconciliation Commission of Canada: Calls to Action. Retrieved January 16, 2024. <https://www2.gov.bc.ca/assets/gov/british-columbians-our-governments/indigenous-people/aboriginal-peoples-documents/calls_to_action_english2.pdf>.
Turpel-Lafond M.E. 2020. In Plain Sight: Addressing Indigenous-Specific Racism and Discrimination in B.C. Health Care. Retrieved September 26, 2023. <https://engage.gov.bc.ca/app/uploads/sites/613/2020/11/In-Plain-Sight-Summary-Report.pdf>.
UBC Digital Emergency Medicine. 2018, April. Robson Valley Virtual Care Pilot Evaluation Report. Retrieved September 26, 2023. <https://emergencycarebc.ca/wp-content/uploads/2018/12/Robson-Valley-Virtual-Medicine-Evaluation-Report_Final-April-2018.pdf>.
United Nations. 2007. United Nations Declaration on the Rights of Indigenous Peoples. Retrieved September 26, 2023. <https://social.desa.un.org/sites/default/files/migrated/19/2018/11/UNDRIP_E_web.pdf>.
Wilkinson, T., B. Bluman, A. Keesey, A. Kolhatkar, G. Grewal, A. Hatry et al. 2015. Rural Emergency Medicine Needs Assessment. British Columbia, Canada, 2014–2015 Final Report. Retrieved September 26, 2023. <https://ubccpd.ca/sites/default/files/documents/Full%20Report_BC%20Rural%20EM%20Study_Mar%2026%202015.pdf>.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed