
ElectronicHealthcare
Improve Office Efficiency by Putting Your Patients to Work: The Financial Viability of an Online Self-Service Appointment Scheduling System in Family Practice (Part 2 of 3)
Abstract
This case study is the second part of a three-part study examining the impact of an online appointment scheduling system on physician office scheduling. The purpose of this case study was to develop a method for determining the financial viability of the self-serve appointment scheduling system. Pay mechanisms for selling software were examined in other industries to offer insight into a financial model used to calculate viability. The analysis produced a financial model to help physicians determine if their practice would benefit from an online scheduling system. Viability was assessed first by ensuring the physician office is busy enough to justify the ongoing costs of system operation. The model then determined the period over which savings resulting from using the system will pay back capital costs. The model compared the costs avoided to the costs incurred in implementing the system. The main costs avoided by the system are receptionist's pay. The financial model showed that an online booking system implemented in a physician office was paid off by the 6th month—significantly sooner than many other health information technology interventions.
Introduction
Many industries are saving human resource costs and providing more convenience by delegating administrative duties to their customers. The banking industry has several decades of experience with automated teller machines. The airline industry has reduced expenses in a highly unionized environment by offering customer self-service kiosks for check-in (Aerospace & Defence Network 2009). The grocery industry, where cashiers make up roughly one third of staff (United States Department of Labor 2008), is saving labour costs by using automated systems to delegate check-out to their customers. Growing internet penetration, trends in patient empowerment, and electronic medical records provide opportunities for physicians to mitigate the rising cost of overhead by delegating basic administrative tasks to patients.
A solo family physician in Sherwood Park, Alberta, a community of 60,000 residents, recently implemented a simple online patient self-service appointment scheduling system. This case study evaluates the implementation, and assesses it as an alternative to conventional scheduling methods in the context of family practice. The purpose of the study was to determine if such a system could be financially viable.
Physician Office Practice and Online System Description
The study focuses on a solo family physician practicing for almost 30 years in Sherwood Park, Alberta, Canada, a community of 60,000 residents. The busy physician office has 2.5 full-time support staff equivalents (FTEs), five examination rooms, and a patient panel size of 2,993 patients. The physician had been using an EMR system for almost 10 years. The practice receives 60 to 90 calls per day for appointments. In the summer of 2008, the physician decided to pilot an online booking system. The vendor hosted, self-service system, uses a virtual private network (VPN) tunnel to send plain HTML GET and POST methods over TCP/IP. The vendor hosted site retrieves patient and schedule data from the physician office hosted EMR scheduling module for presentation to the patient. The system is integrated with the physician's EMR so that patient bookings are automatically inserted in the EMR's schedule. Figure 1 illustrates the architecture of the online booking system.

The physician limited the number of appointments available for online booking during a week. Of the 175 appointments available during a week, 39 appointments were available in the early part of the study for online booking (August 8 to Dec 31, 2008). In the second part of the study, 57 appointments were designated for online booking (January 1 to February 28, 2009). The total number of appointments that were available for online booking during this study was 592, after accounting for time that the office was closed. The rest of the appointment slots were available for booking by telephone, although, the receptionist was empowered to book a calling patient into an open self-booking slot if needed. To discourage patients from abusing the system by booking multiple appointments, the physician implemented a $50 surcharge for no-shows, which he could forgive at his discretion. To use the system, patients logged on to a website and identified themselves to the system by providing their provincial health number (PHN) and their name. Once the system matched them to a client listed in the physician's EMR, the next eight available appointments designated for online scheduling were presented to the patient, who then selected a preferred appointment time. The patient selected one of five appointment types (illness, injury, personal, follow-up, annual physical) from a drop-down list so that the physician can anticipate the nature of the visit. Patients can enter their email address to receive a reminder email. The system is defaulted to send the reminder the day before, but can be adjusted by office staff.
Methods
A financial analysis was used to assess the financial viability of the pilot self-service system. The financial analysis was embodied in a mathematical model that could be used by physicians interested in considering an online appointment scheduling system for their office. The financial model was developed by considering the various costs and benefits of a self-service appointment scheduling system. The model compared the costs avoided (receptionist wages) to the costs incurred (capital costs and periodic maintenance costs) in implementing the system. Other operational factors, such as the number of appointments the physician made available for online booking, the number of calls received during the day, and appointment capacity were also factored into the model. Pricing mechanisms and marketing approaches used to sell software in other industries informed this model.
Results
The cost structure of the online booking system was compared to other software financing models to develop a method for determining the viability of the self-serve appointment scheduling system. Software can be sold on an "out-right" purchase approach, when users simply purchase a box of software for their use in-perpetuity. Alternatively, users may choose to purchase software on a subscription basis, effectively renting or leasing the software from its manufacturer for a period of time. The model proposed here considers both purchase models and is also flexible enough to permit physicians to limit the number of appointments made available for online booking.
The EMR vendor's cost structure consisted of an upfront capital charge to make the necessary software upgrades to allow the physician's EMR system to integrate with the online scheduling system. The vendor's cost model also included a monthly subscription fee to compensate the vendor for maintaining the online booking interface on behalf of the physician. Other charges, such as internet service provider charges, hardware, and software charges must be incurred by the business, regardless of whether an online booking system was used, so these were ignored.
Those patients who booked through the online system did not talk to the receptionist, and thus, costs avoided include the receptionist's costs. Avoided receptionist costs were resolved down to a cost per call for purposes of the financial analysis. The receptionist's fully loaded hourly wage rate (hourly rate plus charges for employee benefits), an average number of calls taken per hour, and an online appointment ratio (which acknowledged that only a portion of appointments are available for booking via the online system) provided for a flexible financial model suitable for evaluation of a online system in several physician office circumstances.
Discussion
A financial model can be developed by comparing the costs avoided to the costs incurred in implementing the system. Physicians would not choose to operate an online booking system if it were more expensive than their receptionist. The main costs avoided by the system are receptionist's pay. For calculation purposes, this wage cost was resolved to a cost avoided per call (Equation 1). This assumes that the receptionist spends most of their time taking calls for appointments. While this was substantially the case in the physician's office, some receptionists also handle other tasks. The model below may be adjusted to accommodate for other tasks. A ratio called the Online Appointment Ratio (Equation 2) allows flexibility should the physician only wish to make a portion of his available appointments available for online booking during the week. The receptionist's appointment ratio is thus Online Appointment Ratio subtracted from 1.


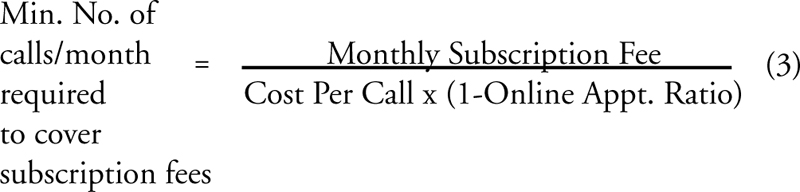
Physicians can determine if the online appointment scheduling system is financially viable by first calculating the minimum call volume they should regularly receive to warrant the monthly subscription costs of the online system (Equation 3). The equation is derived by setting the variable cost of the online system against the variable cost of the receptionist. Clearly, this benchmark is lowered with a high cost per call or when the monthly subscription fee is relatively low. If the physician office's actual number of calls typically received per month falls below this benchmark, then there will not be enough savings to justify the monthly subscription fees. The physician should continue to task the receptionist with the clinic's appointment scheduling function.
If the physician office's call volume is greater than the minimum calculated above, then the next part of the financial model can determine how long it will take to pay back the system. As in Equation 4, the higher the initial capital cost, the longer it will take to justify the investment. Intuitively, the greater the cost savings between receptionist wages and the monthly subscription fee, the sooner the system is justified. The more expensive the staff is and the more calls that are made available for booking through the online system, the sooner the system is paid back.

The case study showed that the physician's online booking system was paid off by the 6th month; significantly sooner than other physician office infrastructure.
The financial model assumes that the receptionist spends most of the time taking calls for appointments, which may not be the case in all physician offices. Receptionists' tasks may be indistinguishable from other administrative duties in the office. Furthermore, receptionists regularly receive phone calls for matters unrelated to appointment scheduling. The implications of these other calls are not considered in this model. Online booking for a sole practitioner is inherently simpler than online booking for a multi-physician clinic; thus, the model presented above may not be applicable to group practice. Appointment scheduling should not be conducted exclusively through online self-service scheduling systems.
Lessons Learned
The above financial model can determine if online self-service appointment scheduling is financially viable. The model suggests that receptionist wages, the capital cost of the system, and ongoing subscription fees are significant factors in assessing viability. Viability is assessed first by ensuring that the ongoing costs of the online system (subscription fees) are less than the ongoing costs of the receptionist (wages). Then, the physician can calculate the length of time it will take for the incremental monthly savings to pay back the capital cost of the system. An online scheduling system may be financially viable if the vendor's pricing structure adequately offsets receptionist costs and achieves payback within an acceptable time period.
About the Author(s)
D.A. Ludwick, PEng., MBA, PMP, PhD is from the Department of Mechanical Engineering, University of Alberta, and General Manager of Sherwood Park – Strathcona County Primary Care Network, Sherwood Park, Alberta. He can be reached at: dave_ludwick@shaw.ca.
John Doucette, PEng., PhD, is from the Department of Mechanical Engineering, University of Alberta, and TRLabs, Edmonton, Alberta.
References
Aerospace & Defence Network. 2009. Aerospace, Defence, Aviation, Security & Space Editorials. "E-ticket Revolution." Retrieved May 25, 2009. <http://www.asd-network.com/editorial_detail/15/E-ticket_revolution.htm>.
United States Department of Labor. 2008. "Career Guide to Industries – Grocery Stores." Retrieved May 25, 2009. <https://www.bls.gov/ooh/>.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Note: Please enter a display name. Your email address will not be publically displayed