
Healthcare Policy
Income and Regional Gradients in Being without a Regular Doctor: Does the Slope of Gradients Decrease for Those with Greater Health Needs?
Abstract
Objective: Income and regional gradients in being without a regular family doctor have been reported. The study objective was to assess the extent to which the slopes of both income and regional gradients vary by individuals' health needs.
Method: Using the Canadian Community Health Survey and multivariate regression analyses, the study examined the income and interprovincial variations in potential access among the healthy and less healthy populations.
Results: The presence of chronic conditions was associated with lower variations in income-related potential access, with the income gradient flattening at the second-lowest income category. Similarly, the presence of two or more chronic conditions flattened interprovincial variations in potential access.
Conclusions: The results suggest a greater equity in having a regular doctor on the basis of need. Systemic changes might be needed to enhance potential access among the vulnerable segment of the population.
Introduction
Benefits of having an established physician–patient relationship have been documented extensively. Having a regular doctor contributes to better continuity and improved patient satisfaction, improves the timeliness and comprehensiveness of preventive care, enhances adherence to treatment and averts inappropriate use of emergency departments for non-urgent conditions (Bindman et al. 1996; Ettner 1999; Gill et al. 2000; Hjortdahl and Laerum 1992; Schoen et al. 2004). By ensuring continuity of care, having a primary care provider is also associated with better management of chronic disease, better population health, fewer physician visits and hospitalizations, lower medical costs during hospitalization and lower total healthcare costs (DeVoe et al. 2003; Engstrom et al. 2001; Gill and Mainous 1998; Lambrew et al. 1996; McIsaac et al. 2001; Saultz and Lochner 2005; Xu 2002).
There is a small but growing empirical literature on the socio-demographic covariates associated with having no regular doctor (Hay et al. 2010; McIsaac et al. 2001; Nabalamba and Millar 2007; Reid et al. 2009; Talbot et al. 2001; Viera et al. 2006). Being male, a young adult, single, healthy, a recent immigrant and poor are associated with higher odds of being without a regular doctor. Regional differences are also found to be the most powerful predictors of reporting no regular physician (Talbot et al. 2001). Implicit in these studies is the assumption that the healthy and less healthy populations are homogeneous in terms of the association between socio-demographic characteristics and not having a regular doctor. More specifically, it is assumed that the slope of income gradient in lacking a regular doctor does not vary by individual health needs, i.e., patients with greater health needs are assumed to be equally less likely to have no regular doctor than the healthy subpopulation, regardless of whether these individuals are poor or non-poor. Similarly, the association between the province of residence and being without a regular doctor is assumed to be invariant to individual health needs, with the less healthy being equally less likely to have no regular doctor than the healthy patients, regardless of the province in which they reside. Such assumptions may not hold if the perceived need for having a regular doctor varies by household income and if the delivery of healthcare services varies across provinces. Healthcare delivery and planning in Canada occur largely at the provincial level, and supply-side barriers (e.g., wait times, geographic location and hours of operation) continue to shape access to care (Sibley and Glazier 2009; Wellstood et al. 2006).
Using the 2010 Canadian Community Health Survey and an appropriate multivariate regression model, this study assessed the extent to which the strength of association between having no regular doctor, household income and province of residence was influenced by individual health needs, as measured by the number of chronic conditions while controlling for a wide range of individual-, household- and community-level factors. An examination of the income and interprovincial variations in access to physicians by the healthy and less healthy populations provides health researchers and policy makers with a more accurate picture of the population lacking a regular doctor. It also highlights the extent to which Canada's universal public health insurance system has been successful in achieving vertical equity, with those with greater health needs having greater potential access to regular primary care providers.
Methods
Data
This study utilized the Canadian Community Health Survey (CCHS 2010) data set conducted by Statistics Canada (2011a). The CCHS is a comprehensive national population survey with a cross-sectional design covering the household population aged 12 or older who lived in private dwellings in the 10 provinces and three territories, except individuals living on Indian reserves and on Crown lands, institutional residents, full-time members of the Canadian forces and residents of certain remote regions (Bland 2002). Details about the design and methods of the CCHS can be found elsewhere (Statistics Canada 2011b).
Analysis
Being without a regular doctor is influenced by a wide range of individual-, household- and community-specific factors related to (potential) access to healthcare services in the categories of contextual characteristics, needs and predisposing and enabling factors (Andersen 1995; Hay et al. 2010; Lambrew et al. 1996; Talbot et al. 2001). A multivariate logistic regression model was used as a base model to assess the association between socio-demographic and health profiles of individuals and their being without a regular physician. To assess whether income and interprovincial variations in lacking a regular doctor vary in strength across the less healthy and healthy subpopulations, the base model was extended by including two sets of interaction terms: one between income and health needs markers, and one between the province of residence and health needs markers. Taking advantage of the comprehensive information collected by the CCHS on chronic conditions, we chose to use the number of chronic conditions rather than self-reported general health status or body mass index (BMI) as a health needs marker in our extended models. To test for the robustness of our results, BMI and self-reported health status were also correlated with income and the province of residence. Differences between point estimates on the interaction terms were tested using chi-square tests. Inserting the province of residence and shortages of physicians as region- and subregion-specific variables, respectively, into the analysis is equivalent to using a fixed-effects model, with region- and subregion-specific variables capturing variations in healthcare utilization across provinces as well as across health regions (Gravelle et al. 2003). The analysis focused on Canada's 10 provinces.
To account for the complex sampling design, data were weighted using weights constructed by the CCHS to adjust for the unequal probabilities of selection. Although the reported standard errors were estimated with robust methods, they do not fully account for the complex sampling design. The public-use version of the CCHS does not contain the information necessary to obtain bootstrapped standard error. All analyses were conducted using the statistical software Stata (version 12.0).
Measures
Access (the dependent variable) is measured by the variable "being without a family doctor." Consistent with the previous literature on the determinants of access to healthcare services, the main predictors of being without a regular doctor were identified as components of needs, predisposing characteristics and enabling factors (Andersen 1995). Three measures of needs in this study were the presence of chronic conditions, self-reported BMI and self-rated general health status. Predisposing characteristics include demographic factors such as sex, marital status, age, educational attainment and ethnic origin. Enabling factors include household income, as reported by the most knowledgeable household member, employment status and the availability of physicians. Because of the small number of observations, Canada's four Atlantic provinces were grouped into one category. Total number of individuals reported as having no regular doctor varies from as low as 72 in Prince Edward Island and 136 in Nova Scotia to as high as 235 in Newfoundland and Labrador. Because the CCHS does not provide information on resources or organization of health services systems across provinces, we used two sets of proxies for inter- and intraprovincial variations in services delivery: one for the respondent's province of residence, and one for the shortage of physicians at a health region within each province. The latter was constructed by the author from the responses given by the respondents without a regular doctor to the question of "Why no regular doctor?": "no one available in area," "not taking new patients," "doctor left or retired" or "not looked for one." Because each province is divided into health regions for administrative purposes, taking the mean of the respondents' responses to the first three parts of the question at a health region provided us with a proxy for the unavailability of physicians in health regions.
Table 1 describes and presents the summary statistics of dependent and independent variables used in the study (see Table 1 at www.longwoods.com/content/23783).
Incomplete responses, "do not know" or "refused to answer" were excluded from the analysis, reducing the sample size to 47,118. These missing observations accounted for less than 6% of the responses for each item with the exception of household income, where missing observations accounted for 17% of the sample population. A comparison of the cases included in the analysis with those excluded cases revealed few differences between the two groups in terms of their socio-demographic and health profiles in most cases. However, age differences were more noticeable for the missing data on income, with younger respondents (aged 12–19 years) being more likely to have missing data. Excluding these missing observations from the analysis is likely to bias our results if these cases are not missing randomly. To test for the robustness of our results, an additional missing category for household income was also created for respondents who did not report their household income, and it was used in the analysis.
Results
Descriptive analysis
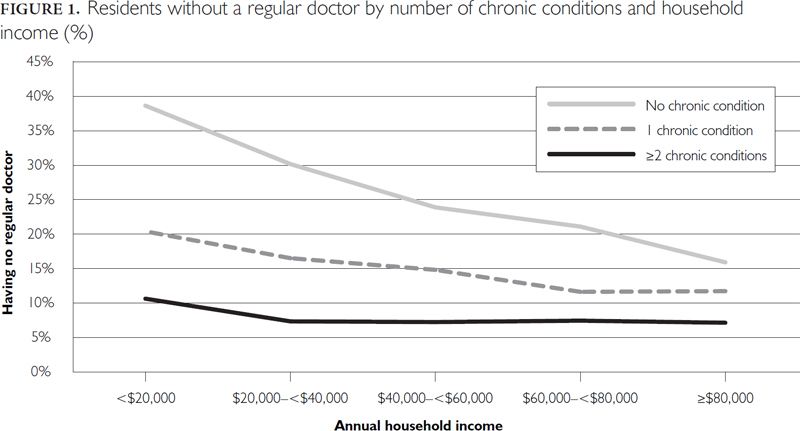
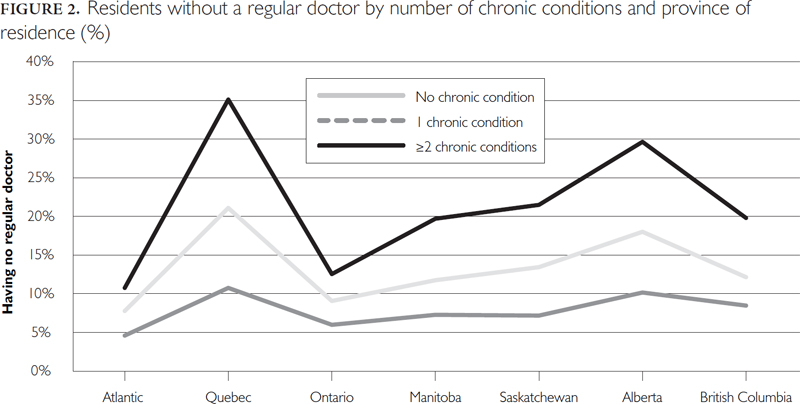
The presence of chronic conditions was associated with variations in access related to lower income (Figure 1). For individuals reporting two or more chronic conditions, the income gradient flattened at the second-lowest income category ($20,000–<$40,000). The difference in the proportion of residents without a regular doctor between the lowest and second income categories was statistically significant at the level of 1%, using chi-square tests. The presence of chronic conditions was also associated with lower interprovincial variations in the proportion of residents without a regular doctor (Figure 2). The reduction in the likelihood of being without a regular doctor was particularly pronounced for residents of Quebec and Alberta who reported two or more chronic conditions. Residents of Ontario with two or more chronic conditions were less likely to report having no regular doctor than residents of Quebec and Alberta. Similarly, residents of the Atlantic provinces were less likely to be without a regular doctor than those in Quebec, Alberta and British Columbia. These interprovincial differences were all statistically significant at the 1% level.
Econometric results
The regression results for having no regular doctor are presented in Table 2 (see Table 2 at www.longwoods.com/content/23783).
Being male, a young adult, single, employed, healthy and a recent immigrant increased the odds of being without a regular doctor. Larger household size and the presence of young children (aged six and younger) reduced the odds of being without a regular doctor. The estimated coefficients for household annual income and the province of residence indicated a strong income and regional gradient. The odds of reporting no regular doctor were 2.2 and 1.7 times, respectively, greater for those in the lowest and second-lowest income categories than those in the richest income category. The odds of having no regular doctor were more pronounced for Alberta, with the residents of Alberta twice as likely to be without a regular doctor than the residents of Ontario.
The results for the interaction terms are reported in Table 3. (Detailed results are available from the author upon request.)
| Table 3. Results for interaction terms between the number of chronic conditions and income and between the number of chronic conditions and provinces | ||||||
| No. chronic conditions | One chronic condition | Two or more chronic conditions | ||||
| Odds ratios | 95% CI | Odds ratios | 95% CI | Odds ratios | 95% CI | |
| No. of chronic conditions* income (ref category: ≥$80,000) | ||||||
| Income | ||||||
| <$20,000 | 2.43** | 1.79, 3.29 | 1.90** | 1.22, 2.96 | 1.66* | 1.13, 2.45 |
| $20,000–<$40,000 | 1.94** | 1.56, 2.41 | 1.55** | 1.14, 2.10 | 1.23 | 0.87, 1.74 |
| $40,000–<$60,000 | 1.50** | 1.25, 1.80 | 1.26 | 0.94, 1.70 | 1.03 | 0.71, 1.48 |
| $60,000–<$80,000 | 1.26* | 1.04, 1.53 | 0.95 | 0.70, 1.29 | 1.06 | 0.72, 1.55 |
| No. of chronic conditions* province (ref category: Ontario) | ||||||
| Province of residence | ||||||
| Atlantic | 0.86 | 0.68, 1.103 | 0.88 | 0.57, 1.34 | 0.74 | 0.52, 1.04 |
| Quebec | 1.98** | 1.62, 2.42 | 1.43* | 1.06, 1.92 | 0.89 | 0.65, 1.21 |
| Manitoba | 1.74** | 1.27, 2.39 | 1.20 | 0.77, 1.87 | 1.00 | 0.61, 1.66 |
| Saskatchewan | 1.61** | 1.17, 2.24 | 1.31 | 0.84, 2.04 | 1.01 | 0.67, 1.51 |
| Alberta | 2.41** | 1.88, 3.09 | 1.92** | 1.35, 2.73 | 1.35 | 0.93, 1.94 |
| British Columbia | 1.54** | 1.22, 1.93 | 1.42 | 1.00, 2.00 | 1.30 | 0.89, 1.92 |
| * Significant at p<0.05 **Significant at p<0.01 |
||||||
The upper panel of Table 3 presents the estimated odds ratios for the interaction terms between household annual income and the number of chronic conditions while using the highest income group (≥$80,000) as a reference category. The results for the interaction terms between household income and no chronic condition (column 1) indicated a negative and steep income gradient, with the healthy individuals in the lowest and second-lowest income categories 2.4 and 1.9 times more likely to be without a regular doctor, respectively, than those in the highest income category. The results for the less healthy subpopulations, i.e., those with one chronic condition and those with two or more chronic conditions (columns 2 and 3), indicated that the negative association between income and being without a regular doctor became less pronounced and statistically insignificant for individuals in the middle and upper-middle income categories ($40,000–<$60,000; $60,000–<$80,000). By contrast, the estimated odds ratios remained statistically significant for those in the lowest income category, with those reporting one chronic and those reporting two or more chronic conditions 1.9 and 1.7 times, respectively, more likely to have no regular doctor than their counterparts in the richest income category. When we tested the hypothesis of the equality of the interaction terms involving no chronic condition and two or more chronic conditions, we found the differences in estimates to be statistically significant for those in the middle income categories, suggesting that the reduction in the likelihood of being without a regular doctor is greater for the residents in the middle income categories than those in the lowest income category.
The results for the interaction terms between the province of residence and the number of chronic conditions are presented in the lower panel of Table 3. The estimated odds ratios of the interaction terms between no chronic conditions and the province of residence (column 1) were statistically significant for all but the Atlantic provinces, with the residents of Alberta more than twice as likely to report having no regular doctor compared to their counterparts in Ontario (reference category). By contrast, none of the estimated odds ratios for those reporting two or more chronic conditions were statistically significant. Differences in estimates for the interaction terms involving no chronic conditions and two or more chronic conditions were statistically significant for the residents of Quebec and Alberta at the 1% level. The results were found to be robust to the use of alternative measures of health needs (self-rated BMI or general health status). All analyses were also run with the full sample using an additional income category for missing observations, and the results were all substantially the same (results available from the author upon request).
Discussion and Conclusion
This study assessed the relationship between socio-demographic and health status profiles and being without a regular doctor in Canada. Consistent with previous findings, econometric results suggest that individuals with no regular doctor were more likely to be male, younger, poor, a recent immigrant and healthy (Hay et al. 2010; McIsaac et al. 2001; Nabalamba and Millar 2007; Reid et al. 2009; Sibley and Weiner 2011; Talbot et al. 2001; Viera et al. 2006). The presence of chronic conditions reduced the odds of having no regular doctor by 32% for those with one chronic condition and by as much as 53% for those with two or more chronic conditions.
Province of residence was also a strong predictor of having no regular doctor, with the odds being particularly pronounced for residents of Alberta and Quebec. This result is also consistent with previous studies (Sanmartin et al. 2004; Sibley and Weiner 2011; Talbot et al. 2001).
However, the results for the interaction terms suggest that estimated income and regional gradients mask wide variations in these factors across the healthy and less healthy subpopulations. The presence of chronic conditions lowered considerably the slope of the income gradient in having no regular doctor, with the income gradient flattened at the second-lowest income category for those reporting two or more chronic conditions. Similarly, the slope of the regional gradient flattened for those reporting two or more chronic conditions.
These findings suggest a greater equity in having a regular doctor on the basis of the need for healthcare. However, the differential lack of potential access by those in the lowest income group suggests that universal public health insurance may not be sufficient to eliminate the gaps related to socio-economic status in potential access to healthcare. A study in the United Kingdom found that individuals in the lower income bracket were more likely to lack a regular doctor (Sweeney and Gray 1995). Socio-economic differentials in access were also reported for the use of physician services in Canada (Asada and Kephart 2007; Dunlop et al. 2000; McIsaac et al. 2001; Sanmartin et al. 2004). A multitude of financial and non-financial barriers, such as rigid work schedules and lack of child care or transportation, may inhibit access to and use of health services by lower-income families and encourage them to turn to walk-in clinics or emergency departments (Dunlop et al. 2000; Talbot et al. 2001). Given the higher prevalence of multiple chronic conditions among lower-income individuals (46% of the respondents in the lowest income group reported two or more chronic conditions versus 21% for those in the highest income group), further research is needed to examine the precise nature of barriers to access to physicians by this vulnerable population.
Some caveats are in order. The regression models do not adequately control for the supply of providers and their density, although inclusion of the province of residence and the proportion of the respondents who reported the unavailability of family physicians in the health region as a main reason for not having a regular doctor may act as a proxy for the availability of family physicians. The cross-section survey data do not allow us to control for unobserved individual heterogeneity, nor do they allow causal relationships between variables to be inferred. Finally, the outcome variable was derived from the question, "Do you have a regular medical doctor?" Some respondents with a regular site of care where they see various providers might have reported being without a regular doctor. For example, it has been suggested that residents of Quebec, where community health movements are more prevalent than in other jurisdictions, receive more care from community health clinics and so do not report having a regular doctor (Talbot et al. 2001). Similarly, some of the rural residents of the Prairie provinces who reported having no regular doctor might use small cottage hospitals and community health centres as a regular site of care (Talbot et al. 2001).
In conclusion, the results of this study provide valuable insights into income and interprovincial variations in lacking a regular doctor across the healthy and less healthy subpopulations. The observed variations across income groups and provinces become less pronounced once health needs are taken into account. However, the finding that low-income individuals with chronic conditions are less likely to have a regular doctor than their counterparts in the richest income category suggests that future primary care programs could be targeted to enhance potential access to primary care providers, particularly for vulnerable segments of the population. Some jurisdictions, such as Ontario, have already taken measures to address timely access to primary care by shifting the policy emphasis from physician supply to strategies for shared care or flexible hours, and helping those with no regular doctor to find healthcare providers (Hay et al. 2010).
Gradient des revenus et gradient régional liés au fait de ne pas avoir de médecin régulier: la pente des gradients est-elle moins inclinée pour ceux qui ont le plus besoin de services de santé?
Résumé
Objectif: Le gradient des revenus et le gradient régional liés au fait de ne pas avoir de médecin de famille régulier ont été documentés. L'objectif de l'étude était d'évaluer à quel point la pente de ces deux gradients varie selon les besoins en services de santé des individus.
Méthode: L'Enquête sur la santé dans les collectivités canadiennes et des analyses de régression multivariable ont servi à étudier les variations de revenu et interprovinciales dans le potentiel d'accès pour des populations saines et moins saines.
Résultats: La présence d'état chronique était associée à de plus faibles variations du potentiel d'accès en fonction du revenu; le gradient des revenus est moins accentué dès la deuxième plus basse catégorie de revenus. Semblablement, la présence de deux états chroniques ou plus réduit les variations interprovinciales quant au potentiel d'accès.
Conclusions: Les résultats font voir qu'il y a plus d'équité liée au fait d'avoir un médecin régulier en fonction des besoins. Des changements systémiques pourraient être nécessaires pour accroître le potentiel d'accès parmi les segments vulnérables de la population.
About the Author(s)
Ardeshir Sepehri, PhD, Professor, Department of Economics, University of Manitoba, Winnipeg, MB
Correspondence may be directed to: Ardeshir Sepehri, PhD, Professor, Department of Economics, University of Manitoba, Winnipeg, MB R3T 5V5; tel.: 204- 474-6241; fax: 204-474-7681; e-mail: sepehri@cc.umanitoba.ca.
References
Andersen, R.M. 1995. "Revisiting the Behavioral Model and Access to Medical Care: Does It Matter?" Journal of Health and Social Behavior 36(1): 1–10.
Asada, Y. and G. Kephart. 2007. "Equity in Health Service Use and Intensity of Use in Canada." BMC Health Services Research 7: 41.
Bindman, A.B., K. Grumbach, D. Osmond, K. Vranizan and A.L. Stewart. 1996. "Primary Care and Receipt of Preventive Services." Journal of General Internal Medicine 11(5): 269–76.
Bland, Y. 2002. "Canadian Community Health Survey – Methodological Overview." Health Reports 13(3): 9–14.
DeVoe, J.E., G.E. Fryer, R. Phillips and L. Green. 2003. "Receipt of Preventative Care among Adults: Insurance Status and Usual Source of Care." American Journal of Public Health 93: 786–91.
Dunlop, S., P. Coyte and W. Mclsaac. 2000. "Socio-Economic Status and the Utilisation of Physicians' Services: Results from the Canadian National Population Health Survey." Social Science and Medicine 51(1): 123–33.
Engstrom, S., M. Foldevi and L. Borgquist. 2001. "Is General Practice Effective? A Systematic Literature Review." Scandinavian Journal of Primary Health Care 19(2): 131–44.
Ettner, S. 1999. "The Relationship between Continuity of Care and the Health Behaviors of Patients: Does Having a Usual Physician Make a Difference?" Medical Care 37(6): 547–55.
Gill, J.M. and A.G. Mainous. 1998. "The Role of Provider Continuity in Preventing Hospitalizations." Archives of Family Medicine 7(4): 352–57.
Gill, J.M., A.G. Mainous and M. Nsereko. 2000. "The Effect of Continuity of Care on Emergency Department Use." Archives of Family Medicine 9(4): 333–38.
Gravelle, H., M. Sutton, S. Morris, F. Windmeijer, A. Leylan, C. Dibben et al. 2003. "Modelling Supply and Demand Influences on the Use of Health Care: Implications for Deriving a Needs-Based Capitation Formula." Health Economics 12(2): 985–1004.
Hay, C., M. Pacey and N. Bains. 2010. "Understanding the Unattached Population in Ontario: Evidence from the Primary Care Access Survey (PCAS)." Healthcare Policy 6(2): 34–47.
Hjortdahl, P. and E. Laerum. 1992. "Continuity of Care in General Practice: Effect on Patient Satisfaction." British Medical Journal 304: 1287–90.
Lambrew, J.M., G.H. DeFriese, T.S. Carey, T.C. Ricketts and A.K. Biddle. 1996. "The Effects of Having a Regular Doctor on Access to Primary Care." Medical Care 34(2): 138–51.
McIsaac, W.J., E. Fuller-Thomson and Y. Talbot. 2001. "Does Having Regular Care by a Family Physician Improve Preventive Care?" Canadian Family Physician 47: 70–76.
Nabalamba, A. and W.J. Millar. 2007. "Going to the Doctor." Health Reports 18(1): 23–35.
Reid, G.J., T.R. Freeman and A. Thind. 2009. "Access to Family Physicians in Southwestern Ontario." Healthcare Policy 5(2): 187–206.
Sanmartin, C., F. Gendron, J.M. Berthelot and K. Murphy. 2004. "Access to Health Care Services in Canada, 2003." Cat. no. 82-575-XIE. Ottawa: Statistics Canada. Retrieved April 4, 2014. <http://publications.gc.ca/Collection/Statcan/82-575-X/82-575-XIE2003001.pdf>.
Saultz, J.W. and J. Lochner. 2005. "Interpersonal Continuity of Care and Care Outcomes: A Critical Review." Annals of Family Medicine 3(2): 159–66.
Schoen, C., R. Osborn, P.T. Huynh, M. Doty, K. Davis, K. Zapert et al. 2004. "Primary Care and Health System Performance: Adults' Experience in Five Countries." Health Affairs (Suppl. Web Exclusives): W4-487–503.
Sibley, L.M. and R.H. Glazier. 2009. "Reasons for Self-Reported Unmet Healthcare Needs in Canada: A Population-Based Provincial Comparison." Healthcare Policy 5(1): 87–101.
Sibley, L.M. and J.P. Weiner. 2011. "An Evaluation of Access to Healthcare Services along the Rural–Urban Continuum in Canada." BMC Health Services Research 11: 20.
Statistics Canada. 2011a. Canadian Community Health Survey 2010: User Guide for the Public Use Microdata File. Ottawa: Author.
Statistics Canada. 2011b. Canadian Community Health Survey – Annual Component. User Guide 2010 and 2009/2010 Microdata Files. Ottawa: Author. Retrieved April 4, 2014. <http://www23.statcan.gc.ca/imdb-bmdi/document/3226_D7_T9_V8-eng.pdf>.
Sweeney, K.G. and D.P. Gray. 1995. "Patients Who Do Not Receive Continuity of Care from their General Practitioner – Are They a Vulnerable Group?" British Journal of General Practice 45: 133–35.
Talbot, Y., E. Fuller-Thomson, F. Tudiver, Y. Habib and W.J. McIsaac. 2001. "Canadians without a Medical Doctor: Who Are They?" Canadian Family Physician 47: 58–64.
Viera, A.J., D.E. Pathman and J.M. Garrett. 2006. "Adults' Lack of a Usual Source of Care: A Matter of Preference?" Annals of Family Medicine 4(4): 359–65.
Wellstood, K., K. Wilson and J. Eyles. 2006. "'Reasonable Access' to Primary Care: Assessing the Role of Individual and System Characteristics." Health and Place 12(2): 121–30.
Xu, K.T. 2002. "Usual Source of Care in Preventive Service Use: A Regular Doctor versus a Regular Site." Health Services Research 37(6): 1509–29.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed