
Healthcare Policy
Lessons from Long-Term Care Facilities without COVID-19 Outbreaks
Mélanie Lavoie-Tremblay, Guylaine Cyr, Thalia Aubé and Geneviève Lavigne
Abstract
Background: The COVID-19 crisis in long-term care (LTC) homes was devastating for residents and front-line workers. Recent reports have detailed what went wrong in LTC facilities, including equipment shortages, lack of preparedness, underestimation of COVID-19's virulence and bans on caregiver visits. Less is known about what went well in some facilities.
Purpose: To describe nurses' and other staff members' experiences and lessons learned in two LTC facilities in Quebec that reported no COVID-19 outbreaks during the first wave of the pandemic.
Methods: A case study design guided by appreciative inquiry was conducted, in which a case was defined as a LTC facility without COVID-19 outbreaks; two cases were included. Twenty-three healthcare team members from the two sites were recruited and interviewed between October and November, 2020.
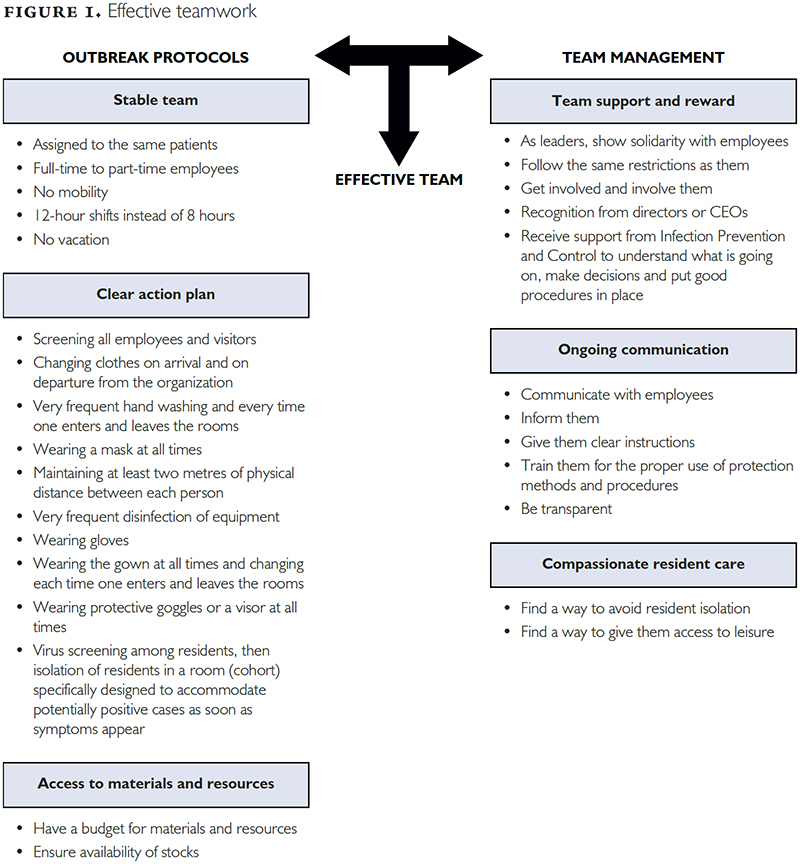
Results: Several common themes were identified: being informed and respecting outbreak protocols; the presence of key outbreak protocols, which allowed for stable teams; a clear action plan; and access to materials and resources. Key management themes included team support and reward, ongoing communication and providing compassionate care to residents.
Conclusion: This study highlights several lessons learned that have the potential to strengthen the LTC health system.
Background and Purpose
In March 2020, the World Health Organization (WHO) declared COVID-19 a global pandemic. By the end of the first wave, over 10 million cases and more than 495,781 mortalities were reported worldwide and 8,504 deaths were reported in Canada (Flood et al. 2020). The case-mortality rate increased vastly by age group: 20.1% for those aged 70 to 79 years and 34.4% for those aged 80 years and older (PHAC et al. 2020).
Long-term care (LTC) facilities provide 24-hour functional support for residents who are frail, require assistance with activities of daily living and often have multiple co-morbidities. Most residents are over the age of 80 and approximately 70% have dementia (Hsu and Lane 2020). These facilities are at the margins of the healthcare system, which is biased toward curative and acute care. Due to decades of chronic underfunding and understaffing, the LTC system was weak and vulnerable leading up to the pandemic (Doucet 2020). Sadly, it is within this context that COVID-19 spread through the vulnerable and weakened LTC facilities.
The first wave of the pandemic corresponds to the first six months, specifically from March 1 to August 31, 2020 (CIHI 2021a). During those first six months, about 69% of COVID-19 deaths nationwide were in LTC and retirement homes (CIHI 2021a). By the end of the first wave, nearly 4,000 residents in Quebec had died, representing about 0.05% of the total provincial population (CIHI 2021a; Institut de la Statistique du Québec [ISQ] 2020). In addition to the highest increase in excess deaths, LTC facilities in Quebec and Ontario had the largest proportion of outbreaks at 44% and 34%, respectively (CIHI 2021a).
In Quebec, as in most provinces, the first wave focused on personal protective equipment (PPE) and shortages of masks, visors and gowns for healthcare workers (Protecteur du Citoyen 2020). Distribution of PPE prioritized the hospital system, with allocation to LTC facilities discordant and uncertain. Management of LTC facilities was censured worldwide. The Quebec Ombudsman conducted an independent investigation of LTC facilities in the province and found several issues (Protecteur du Citoyen 2020). First, facilities were not prepared for the pandemic. Second, the virulence of COVID-19 was underestimated. Third, PPE was insufficient and unequally distributed. Fourth, banning caregiver visitors led to a further decline in LTC residents' physical and mental health and resulted in basic care needs not being met. Fifth, facilities were not prepared to provide the same intensity of care as hospitals but were expected to do so. Sixth, the deployment of relief teams in the form of military personnel was not expeditious. Finally, further challenges were created due to a lack of onsite management and decision-making power.
Internationally, staffing issues related to nurses and other healthcare providers have been cited as a common problem (Abbasi 2020). Before COVID-19, staff-to-resident ratios, employment status and compensation/sick leave were found to be problematic in Ontario LTC homes and were greatly exacerbated during the pandemic (Oldenburger et al. 2022).
While most of the literature has focused on pandemic-related issues and challenges, less is known about what was done well in LTC facilities that avoided outbreaks. To the best of our knowledge, no qualitative study has explored this issue. To address this gap our study aimed to describe nurses' and other staff members' experiences and lessons learned in two LTC facilities in Quebec that reported no COVID-19 outbreaks during the first wave of the pandemic (i.e., during the first 6 months between March 1 and August 31, 2020). An appreciative inquiry approach was used (Bushe 2011; Cooperrider and Whitney 2001). A better understanding of what was done well during the initial contact with the pandemic can help inform LTC practices and inform policy changes not only in Quebec but also throughout Canada.
Methods
A case study design guided by appreciative inquiry was conducted, in which a case was defined as an LTC facility without COVID-19 outbreaks between March 1 and August 31, 2020. Two cases were included. Case studies allow for an in-depth exploration of a select number of cases (Yin 2017). Emphasis was on exploring strengths rather than deficiencies and an appreciative inquiry approach was used to create the semi-structured interview questions (Cooperrider and Whitney 2001). Approval was obtained from the Institutional Ethical Review Committee from each facility and consent for voluntary participation was obtained from the participants. The study reported here is part of a broader Canadian research project dedicated to the study of LTC facilities in the healthcare sector (Baumann et al. 2022). It is important to note that the facilities included in this study are atypical of the majority of facilities in Quebec and Canada.
Participants
A convenience sample was used. We invited all nurses and other healthcare providers from two LTC facilities in Montreal, QC, that remained free of COVID-19 outbreaks despite being in a red zone (i.e., a maximum alert area [Touzin and Duchaine 2020]) during the first wave of the pandemic. Potential participants were invited via an e-mail sent by key contacts (coordinators) at both LTC facilities on behalf of the principal investigator. Interested individuals were invited to contact the research assistant by e-mail to ask for more information, pose questions or indicate their interest in participating in the study. The research assistant contacted interested participants by e-mail or phone to answer any questions, review the consent form and plan the interview.
The first LTC facility, which was established in 1944, has a new building that opened in 1977. Today, this facility is a member of the integrated university health and social services centres. The centre has four units and can accommodate 134 residents. The healthcare team covering the day, evening and night shifts is equivalent to the full-time hours of 11 nurses, 17 licensed practical nurses (LPNs) and 46 resident attendants. The staff team consists of 124 personnel who hold part-time or full-time positions. None of the staff is contracted and there are no professional agency employees.
The second LTC facility, which was established in 1992, is within a hospital that has been part of the University Health Network since 2008. This facility is divided into three floors or units and has 143 single rooms, including 20 beds dedicated to residents who require ventilator support. The healthcare team covering the day, evening and night shifts is equivalent to the full-time hours of 12 nurses, 6 LPNs and 18 patient attendants. The staff team consists of 68 personnel who are mixed into different care teams. They work full time or part time and are all unionized. There are no professional agency employees.
The following types of staff were invited to participate in the study: nurses, LPNs, nurse managers, infection prevention and control (IPAC) personnel, personal support workers (PSWs), housekeeping staff, nursing advisors and rehabilitation personnel. The overarching inclusion criteria were to be a staff member at one of the two LTC facilities, to have been working during the six months of the first wave, to be older than 18 years of age, to be able to speak French or English and to have access to the Internet and a phone.
Data collection and analysis
Data were collected from 22 individual interviews (Site 1: n = 15; Site 2: n = 7) using a semi-structured interview guide. This sample size per site was found sufficient to reach adequate data saturation. All interviews were conducted over the phone between October and November 2020 and were audio-recorded. The interviewer specified that the questions were specifically referring to the period corresponding to the first wave of the pandemic (i.e., from March 1 to August 31, 2020). Sample interview questions included "Describe what you did to face this pandemic?" and "How do you explain that you did not have any residents contract COVID on your site?" Each interview lasted about 30 to 40 minutes. Participants were allowed to respond in either French or English. The interviews were digitally recorded and transcribed verbatim. An audit trail tracked all material and documentation related to the data (Krefting 1991). The interviews were collected by a trained researcher with several years of experience in qualitative data collection and analysis.
Data were analysed using inductive thematic analysis as described by Miles and Huberman (1994). A full cross-sectional analysis of the two cases was then performed (Vallis and Tierney 2000). Theme-based strategies were applied to identify similarities and differences among the cases (Miles and Huberman 1994; Teddlie and Tashakkori 2009). This method of qualitative data analysis involves three concurrent activities: condensing the data, data display and verification of the data. Open coding involves the researchers reviewing the interview transcripts closely, line by line, and extracting sections that met the study objective. Codes are created by condensing the original data and categories are formed by clustering codes referring to similar concepts. As a second step, Miles and Huberman proposed creating data displays (e.g., graphs, charts) to define key concepts embodied in the analysis to illustrate how the concepts are interrelated. Data displays involve the elaboration and verification of the data as a continual process (Miles and Huberman 1994). To enhance confirmability and trustworthiness of interpretation, a subset of the data was coded and analyzed by two researchers with expertise in qualitative data analysis; consensus around the emerging interpretations was reached among researchers through discussions (Polit and Beck 2008). Descriptive statistics were generated through Excel based on demographic information provided by participants.
Results
Several common themes were identified. As illustrated in Figure 1, participants (P1–P23) were able to be effective as a team by being informed and respecting outbreak protocols that were put in place early by their institution. The establishment of the protocols also allowed for a clear action plan and access to materials and resources. Furthermore, COVID-19 outbreak management and the success of the facilities in achieving zero cases were facilitated by team management. This included team support and reward, ongoing communication and the provision of compassionate resident care. Overall, the themes identified were similar in both facilities. However, some nuances were noted. These are detailed below when relevant.
Outbreak protocols
STABLE TEAM
According to participants, a stable team was achieved by ensuring adequate staffing and providing continuity of care to residents by assigning the same employees to the same residents. Part-time employees were offered full-time hours and the practice of employees working in other areas of the facility or in different facilities was eliminated, thereby reducing the risk of viral transmission. Some movement between floors of the facility was still allowed at Site 2 but prohibited at Site 1.
The first thing is to keep our residents safe … the employees who have a part-time position, they have all been upgraded to a full-time position. (P4)
In addition, at both facilities, a stable team was achieved by not allowing any vacation leave. Site 2 also instituted 12-hour shifts instead of 8-hour shifts, which reduced the amount of staff turnover within a day.
CLEAR ACTION PLAN
Participants from both sites highlighted several clear, effective actions. These included screening all employees and visitors for COVID-19 symptoms upon their arrival, requiring employees to change from their civilian clothes to their uniforms upon arrival and departure from the facility and maintaining physical distancing between each person. At Site 1, employees were screened for COVID-19 symptoms daily while at Site 2 they were screened three times per week.
[I]f, for example, we have a symptom, we have to go directly to be tested, not return. Finally, we will get tested and then we basically don't go back to work until we get the result. Then the employees are paid at that point, in COVID mode. (P17)
Rigorous IPAC practices were implemented at the facilities. Employees were required to always wear surgical masks, frequently disinfect equipment, wash hands upon entering and exiting patient rooms, wear PPE and adhere to proper donning and doffing procedures upon entering and exiting patient rooms. Residents were also screened daily. Any residents experiencing one or more COVID-19–like symptoms were immediately isolated to rooms that could accommodate a potentially positive case.
ACCESS TO MATERIALS AND RESOURCES
Participants mentioned how their facilities budgeted and planned to ensure sufficient PPE for their daily use. Readily available stock for the employees ensured they had the proper resources to protect themselves and their residents.
There was no shortage of stock, I mean, the PPE. Our head nurse bought extra in advance. She always made sure we had everything. We didn't lack anything. We had no excuse. (P21)
Furthermore, they were provided with teaching on proper IPAC practices, such as how to don and doff PPE before entering and exiting residents' rooms.
Education was becoming important … The education department was doing practices. Videos have been put in place to show staff how to put on the N95, how to dress. (P3)
TEAM MANAGEMENT
Participants mentioned team support and reward, ongoing communication and the provision of compassionate resident care.
TEAM SUPPORT AND REWARDS
Participants described having team support and rewards, or recognition, for their efforts during the pandemic as key to their success. Support came from their colleagues – from nurses to the housekeeping staff – and from their leaders. The leaders showed their solidarity by following the same restrictions as their employees and by being on the ground and working alongside staff to face the crisis. Team leaders supported participants' involvement in COVID-19 management and encouraged them to share their input and feedback on the issues.
The management are very, very supportive, which makes a big difference like when you see the manager come in at night to give you support … it makes a big difference. (P17)
Because of their teamwork success, participants reported receiving recognition from the director of the facility. Furthermore, they had continuous involvement from the IPAC team who, like their managers, made a collaborative effort to understand the situation at the facility and to ensure properly shared decision making and implementation of good practices. At Site 1, an IPAC team member was always present at the facility while at Site 2 the IPAC team was only contacted if needed.
ONGOING COMMUNICATION
Participants recognized the importance of ongoing communication and transparency with employees. Ongoing communication involved informing all employees about any new decisions or changes to practices, providing them with clear instructions on any new protocols and education and training around proper IPAC practices. Follow-up with communicated directives involved managers inspecting their facilities to ensure the measures were part of the daily practices.
I think communication was a really big key. So the fact that all communication from the top got to the bottom was really important. The way the message was communicated and who was communicating the message was important for me. (P16)
Being transparent involved being open with employees as well as giving them timely and accurate information about the COVID-19 situation and its impact on the facility.
Questions were answered on the intranet. We had our manager who [hosted] webinars every week. Even our director of nursing hosted webinars every week to answer the managers. So everything was transparent. (P1)
COMPASSIONATE RESIDENT CARE
Participants expressed that their primary goal was to ensure a safe environment for the residents. One measure put in place across Quebec was to temporarily restrict visitors to LTC facilities, which greatly diminished residents' social interactions. To mitigate this, the staff tried to maintain their well-being and decrease their isolation by providing access to leisurely activities (e.g., musicotherapy at Site 1), setting up video calls with residents' family members and even designating a staff member to organize activities.
We ma[de] them laugh and we danced. I have seen some of my PABs [préposé aux bénéficiaires]1 just dance around them and they just laughed … because it has been hard on the residents [and] they can't even go outside … It's too much … they're isolated. (P19)
Discussion
The present study sought to identify what enabled the success of two LTC facilities in Quebec that remained free of COVID-19 outbreaks during the first wave. By identifying the measures and practices that proved successful in these facilities, more informed policies could be proposed and implemented throughout the country to protect our vulnerable elderly population.
Overall, the present results suggest that their success could be attributed to better management of movement within the facilities, including who entered and exited; screening of employees and residents for symptoms and their subsequent isolation and testing; the presence of managers on site; and rigorous IPAC policies such as ensuring sufficient stock and use of PPE. Other factors included strong leadership. A stable healthcare team included a larger complement of full-time workers and effective, daily communication that included clear instructions and education on new protocols. Results from the present study highlight the important role played by managers and the significant impact of managerial transparency. It is likewise important to have leaders who show team support, reward, recognition and solidarity. Interestingly, although some minor differences were noted between the two successful facilities, most of the procedures and actions they employed during the first wave of the pandemic were very similar.
A similar study conducted in Ontario (Baumann et al. 2022) also identified key factors such as leadership, clear and effective communication, adequate staffing measures and staff recognition and respect as having been influential in successfully managing LTC homes during the first wave of the pandemic. Other recent studies suggested similar successful strategies, such as the early implementation of policy measures, including adequate staffing, limiting movement of workers between multiple sites and access to and proper use of PPE (Rios et al. 2020). Evidence is growing that LTC facilities that assigned staff to specific zones had fewer outbreaks (Rolland et al. 2020; Viray et al. 2021). Other effective strategies recently identified include sufficient PPE, adequate outbreak preparedness plans, statutory sick pay, sufficient staff-to-bed ratios, early detection and systematic testing, greater funding of LTC facilities and fewer shared rooms (Fernandes et al. 2021; Liu et al. 2020; Viray et al. 2021).
Most Canadian provinces imposed restrictions that prevented family caregivers from visiting and assisting in the care of their loved ones (CIHI 2021b). The International Long Term Care Policy Network published a review of the guidelines and practices regarding visits to residents in LTC facilities during COVID-19 (Low et al. 2021) and made it very clear that a complete visitor and family caregiver ban was detrimental to residents' cognitive and psychological health, but that LTC facilities should be better supported and should receive additional funding to ensure that they were able to implement safe practices around visits to residents. In the present study, it was found that staff went to great lengths to minimize the impact of the lost social connection that residents experienced because of the visitation ban. This was also observed in the LTC homes in Ontario that were successful in protecting their residents from COVID-19 (Baumann et al. 2022). The specific context of LTC necessitates a high degree of compassionate care, especially in difficult times (such as during the lockdowns due to COVID-19). This is an additional reason why LTC facilities need to be sufficiently staffed with individuals who are not overworked and who are treated well by their managers and the organization.
Calls to better prepare LTC facilities for outbreaks and to develop and implement guidance plans and programs for prevention and control have been made in Canada, Europe and the US (Baumann et al. 2022; Blain et al. 2020; Grabowski and Mor 2020; Werner et al. 2020). The results of the present study are in line with several policy changes recommended in recent months. Although the experiences of the two facilities that were included in the present study are atypical compared with those of the majority of facilities in Quebec and Canada, the findings suggest successful strategies that could be deployed if adequate resources are allocated to LTC and relevant policies are implemented. First, adequate staffing and funding measures are of utmost importance (Ducharme 2021). Policy measures need to be implemented specifying adequate staff to patient ratios. Staff must be offered full-time employment with appropriate pay and benefits to ensure proper care as well as to limit multi-site transmission of viruses (Estabrooks et al. 2020; Hsu and Lane 2020). Policy measures regarding staff training and IPAC practices are necessary (CIHI 2021a).
Improved communication within LTC facilities and among parts of the healthcare system would benefit both staff and residents. In addition, access to PPE for all staff must be prioritized going forward. As suggested by Estabrooks and colleagues (2020), national standards regarding staffing, staffing mix, training requirements and protocols for outbreaks in LTC facilities would ensure adequate and uniform care for residents. Funding should be guaranteed to ensure proper inspections of LTC facilities and for the enforcement of these national standards (CIHI 2021a).
Strengths and limitations
This qualitative study presents several strengths; however, some limitations must be highlighted. First, only two LTC facilities were included, which limits the generalizability of the findings. Most themes extracted from the data were common between the two sites, however, suggesting that strategies may be generalizable to other facilities. Second, both LTC facilities were in a large urban centre; more rural centres may have been impacted differently. Third, only qualitative data were collected in the present study and only from nurses and healthcare providers. The perspective of other important actors such as residents and their family members would be highly informative. Finally, the interviews were conducted during the first three months of the second wave, which might have influenced participants' answers. That said, it should be noted that according to the Canadian Institute for Health Information (2021a), the second wave of the pandemic lasted until February 15, 2021. Thus, it is believed that even if the participants' responses were influenced by their experiences after the official end of the first wave, their insights were nonetheless highly relevant to the overall initial response to the pandemic.
Conclusion
Due to COVID-19, the LTC sector has been changed forever. The provincial and federal governments must seriously consider and respond to what the pandemic revealed regarding the fragility of the sector. LTC must be put at the top of the planning process, not neglected at the bottom where it has traditionally been. The impact of COVID-19 worldwide has created many lessons to be learned. Evidence and the present study demonstrate that the proper implementation of IPAC policies was one of the most effective strategies for reducing COVID-19 outbreaks and mortality. The COVID-19 pandemic requires a deep analysis and reflection of how we care for vulnerable people. Lessons learned from this experience must be implemented to strengthen the LTC sector and more effectively protect our elderly population.
Leçons tirées des établissements de soins de longue durée sans éclosion de COVID-19
Résumé
Contexte: La crise de la COVID-19 dans les foyers de soins de longue durée (SLD) a été dévastatrice pour les résidents et les travailleurs de première ligne. De récents rapports ont détaillé ce qui n'allait pas dans les établissements de SLD, notamment les pénuries d'équipement, le manque de préparation, la sous-estimation de la virulence de la COVID-19 et l'interdiction des visites des proches aidants. On en sait moins sur ce qui s'est bien passé dans certains établissements.
Objectif: Décrire les expériences et les leçons apprises des infirmières et des autres membres du personnel dans deux établissements de SLD au Québec qui n'ont signalé aucune éclosion de COVID-19 au cours de la première vague de la pandémie.
Méthode: Nous avons mené une étude de cas guidée par une enquête appréciative, dans laquelle un cas était défini comme un établissement de SLD sans éclosion de COVID-19; deux cas ont été retenus. Vingt-trois membres des équipes soignantes des deux sites ont été recrutés et interviewés entre octobre et novembre 2020.
Résultats: Plusieurs thèmes communs ont été dégagés: être informé et respecter les protocoles en cas d'éclosion; la présence de protocoles clés en cas d'éclosion, qui permettent la stabilité des équipes; un plan d'action clair; et l'accès au matériel et aux ressources. Les principaux thèmes de gestion comprenaient le soutien et la récompense de l'équipe, la communication continue et la compassion envers les résidents.
About the Author(s)
Mélanie Lavoie-Tremblay, Rn, Phd, Professor And Vice Dean Research, Innovation and Entrepreneuriat, Faculty of Nursing, University of Montreal, Montreal, QC
Guylaine Cyr, PhD, Research Assistant, Ingram School of Nursing, McGill University, Montreal, QC
Thalia Aubé, RN, MSc, Research Assistant, Ingram School of Nursing, McGill University, Montreal, QC
GenevièVe Lavigne, PhD, Research Assistant, Ingram School of Nursing, McGill University, Montreal, QC
Correspondence may be directed to: Mélanie Lavoie-Tremblay. Mélanie can be reached by e-mail at melanie.lavoie-tremblay@umontreal.ca.
References
Abbasi, J. 2020. "Abandoned" Nursing Homes Continue to Face Critical Supply and Staff Shortages as COVID-19 Toll has Mounted. JAMA 324(2): 123–25. doi:10.1001/jama.2020.10419.
Baumann, A., M. Crea-Arsenio, M. Lavoie-Tremblay, A. Meershoek, P. Norman and R. Deber. 2022. Exemplars in Long-Term Care during COVID-19: The Importance of Leadership. Healthcare Policy 17(Special Issue): 27–39. doi:10.12927/hcpol.2022.26856.
Blain, H., Y. Rolland, J.M.G.A. Schols, A. Cherubini, S. Miot, D. O'Neill et al. 2020. August 2020 Interim EuGMS Guidance to Prepare European Long-Term Care Facilities for COVID-19. European Geriatric Medicine 11(6): 899–13. doi:10.1007/s41999-020-00405-z.
Bushe, G.R. 2011. Appreciative Inquiry: Theory and Critique. In D. Boje, B. Burnes and J. Hassard, eds., The Routledge Companion to Organizational Change (pp. 87–103). Routledge.
Canadian Institute for Health Information (CIHI). 2021a. The Impact of COVID-19 on Long-Term Care in Canada: Focus on the First 6 Months. Retrieved May 2, 2022. <https://www.cihi.ca/sites/default/files/document/impact-COVID-19-long-term-care-canada-first-6-months-report-en.pdf>.
Canadian Institute for Health Information (CIHI). 2021b. COVID-19 Intervention Scan. Retrieved May 2, 2022. <https://www.cihi.ca/en/COVID-19-intervention-scan>.
Cooperrider, D.L. and D. Whitney. 2001. A Positive Revolution in Change. In D.L. Cooperrider, P. Sorenson, D. Whitney and T. Yeager, eds., Appreciative Inquiry: An Emerging Direction for Organization Development (pp. 9–29). Stipes.
Doucet, H. 2020. « Répondre à la vulnérabilité »: l'éthique et les CHSLD au temps de la COVID-19 ["Responding to Vulnerability": Ethics and CHSLD in the Age of COVID-19]. Éthique & Santé 17(3): 142–46. doi:10.1016/j.etiqe.2020.07.003.
Ducharme F. 2021, June 2. Long-Term Care: Caregivers Are a Key Factor. Policy Options. Retrieved May 2, 2022. <https://policyoptions.irpp.org/magazines/june-2021/soins-de-longue-duree-le-personnel-soignant-est-un-facteur-cle/>.
Estabrooks, C.A., S.E. Straus, C.M. Flood, J. Keefe, P. Armstrong, G.J. Donner et al. 2020. Restoring Trust: COVID-19 and the Future of Long-Term Care in Canada. FACETS 5(1): 651–91. doi:10.1139/facets-2020-0056.
Fernandes, Ó.B., P.L. Julião, N. Klazinga, D. Kringos and N. Marques. 2021. COVID-19 Preparedness and Perceived Safety in Nursing Homes in Southern Portugal: A Cross-Sectional Survey-Based Study in the Initial Phases of the Pandemic. International Journal of Environmental Research and Public Health 18(15): 7983. doi:10.3390/ijerph18157983.
Flood, C., V. MacDonnell, J. Philpott, S. Theriault and S. Venkatapuram, eds. 2020. Vulnerable: The Law, Policy and Ethics of COVID-19. University of Ottawa Press.
Grabowski, D.C. and V. Mor. 2020. Nursing Home Care in Crisis in the Wake of COVID-19. JAMA 324(1): 23–24. doi:10.1001/jama.2020.8524.
Hsu, A.T. and N. Lane. 2020, April 15. Impact of COVID-19 on Residents of Canada's Long-Term Care Homes – Ongoing Challenges and Policy Response. International Long-Term Care and Policy Response. Retrieved May 2, 2022. <https://ltccovid.org/wp-content/uploads/2020/04/LTCcovid-country-reports_Canada_Hsu-et-al_updated-April-14-2020.pdf>.
Institut de la Statistique du Québec (ISQ). 2020, December 9. Record Population Growth in Québec in 2019, but Significant Slowdown in the First Months of 2020 [News release]. Retrieved March 10, 2022. <https://statistique.quebec.ca/en/communique/record-population-growth-quebec-2019-significant-slowdown-first-months-2020>.
Krefting, L. 1991. Rigor in Qualitative Research: The Assessment of Trustworthiness. American Journal of Occupational Therapy 45(3): 214–22. doi:10.5014/ajot.45.3.214.
Liu, M., C.J. Maxwell, P. Armstrong, M. Schwandt, A. Moser, M.J. McGregor et al. 2020. COVID-19 in Long-Term Care Homes in Ontario and British Columbia. CMAJ 192(47) E1540–546. doi:10.1503/cmaj.201860.
Low, L.-F., K. Hinsliff-Smith, S. Sinha, N. Stall, H. Verbeek, J. Siette et al. 2021. Safe Visiting at Care Homes during COVID-19: A Review of International Guidelines and Emerging Practices during the COVID-19 Pandemic. International Long-Term Care Policy Network. Retrieved May 2, 2022. <https://ltccovid.org/wp-content/uploads/2021/01/Care-home-visiting-policies-international-report-19-January-2021-4.pdf>.
Miles, M.B. and A.M. Huberman. 1994. Qualitative Data Analysis: An Expanded Sourcebook. Sage.
Oldenburger, D., A. Baumann, M. Crea-Arsenio, R. Deber and V. Baba. 2022. COVID-19 Issues in Long-Term Care in Ontario: A Document Analysis. Healthcare Policy 17(Special Issue): 53–65. doi:10.12927/hcpol.2022.26854.
Polit, D.F. and C.T. Beck. 2008. Nursing Research: Generating and Assessing Evidence for Nursing Practice (8th ed.). Lippincott Williams & Wilkins.
Protecteur du Citoyen. 2020, December 10. The Quebec Ombudsman's Status Report : COVID-19 in CHSLDs during the First Wave of the Pandemic. Retrieved May 2, 2022. <https://protecteurducitoyen.qc.ca/sites/default/files/pdf/rapports_speciaux/progress-report-chslds-COVID-19.pdf>.
Public Health Agency of Canada (PHAC); Surveillance; Epidemiology Team1. 2020. Descriptive Epidemiology of Deceased Cases of COVID-19 Reported during the Initial Wave of the Epidemic in Canada, January 15 to July 9, 2020. Canada Communicable Disease Report 46(10): 344–48. doi:10.14745/ccdr.v46i10a06.
Rios, P., A. Radhakrishnan, C. Williams, N. Ramkissoon, B. Pham, G.V. Cormack et al. 2020. Preventing the Transmission of COVID-19 and Other Coronaviruses in Older Adults Aged 60 Years and Above Living in Long-Term Care: A Rapid Review. Systematic Reviews 9(1): 218. doi:10.1186/s13643-020-01486-4.
Rolland, Y., M.-H. Lacoste, A. De Mauleon, A. Ghisolfi, P. De Souto Barreto, H. Blain et al. 2020. Guidance for the Prevention of the COVID-19 Epidemic in Long-Term Care Facilities: A Short-Term Prospective Study. The Journal of Nutrition, Health & Aging 24(8): 812–16. doi:10.1007/s12603-020-1440-2.
Teddlie, C. and A. Tashakkori, eds. 2009. Foundations of Mixed Methods Research: Integrating Quantitative and Qualitative Approaches in the Social and Behavioral Sciences. Sage.
Touzin, C. and G. Duchaine. 2020, June 29. CHLSD : La recette pour résister au virus. La Presse. Retrieved May 2, 2022. <https://www.lapresse.ca/COVID-19/2020-06-29/chsld-la-recette-pour-resister-au-virus.php#>.
Vallis, J. and A. Tierney, A. 2000. Issues in Case Study Analysis. Nursing Research 7(2): 19–35. doi:10.7748/nr2000.01.7.2.19.c6111.
Viray, P., Z. Low, R. Sinnappu, P.A. Harvey and S. Brown. 2021. Residential Aged Care Facility COVID-19 Outbreaks and Magnitude of Spread among Residents: Observations from a Victorian Residential In-Reach Service. Internal Medicine Journal 51(1): 99–101. doi:10.1111/imj.15143.
Werner, R. M., A.K. Hoffman and N.B. Coe. 2020. Long-Term Care Policy after COVID-19 – Solving the Nursing Home Crisis. The New England Journal of Medicine 383(10): 903–05. doi:10.1056/NEJMp2014811.
Yin, R.K. 2017. Case Study Research: Design and Methods (6th ed.). Sage.
Footnotes
1. Medical orderlies.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed