
Healthcare Policy
Efficiency Through Equity: Prioritizing Gynecologic Surgery to Improve Health System Performance
Abstract
Gynecologic surgery is underserved in Canada, despite its volume and impact on health system performance, including the experiences of women surgeons and patients. Structural gender biases in reimbursement, scheduling and innovation contribute to long wait times, reduced surgical throughput and diminished quality of care. This editorial outlines five strategies to improve system efficiency: formal recognition of gynecologic surgery, compensation and scheduling reform, investment in inclusive surgical tools and infrastructure, primary care integration and public advocacy. Prioritizing gynecologic surgery is essential to achieving a high-performing, equitable Canadian health system.
Introduction
Gynecology is the discipline that provides specialized care for the female reproductive tract. The vast majority of women in developed countries will see a gynecologist at least once in their lifetime (Gomez et al. 2025). Due to population growth and increasing life expectancy of women, demand for women's health services such as Gynecology is projected to increase.Despite this, Gynecology is one of the most underserved surgical specialties in Canada. An estimated national median waiting time from primary care referral to gynecologic surgery – including hysterectomy, pelvic floor repair, oophorectomy, dilation and curettage and endometrial ablation – was 41.3 weeks in 2024 (Moir and Barua 2024). This is longer than surgical disciplines with similar case complexity such as urology (27.4 weeks) and general surgery (22.3 weeks) (Moir and Barua 2024). Wait times vary across the country and by procedure. For example, the weighted median patient wait time for gynecologic surgery after an appointment with a gynecologist is 12.9 weeks in Ontario but 77.9 weeks in New Brunswick (Moir and Barau 2024). Granular comparisons of provincial wait times can be difficult, as not all provinces separate benign versus cancerous gynecologic surgeries, and some provinces, such as Alberta, do not even include gynecologic surgery in their public reporting. The province of Ontario is able to provide insight, with contemporary public waitlist data revealing that hysterectomy for benign disease has a wait time of 71 days and pelvic organ prolapse (POP) surgery of 149 days; in comparison, benign prostate surgery, analogous in complexity (Chaikof et al. 2023) and for conditions with comparable symptom burden, only has a median wait of 33 days (Ontario Health 2025). As with other surgical specialties, differences in wait times for gynecologic surgery are worse for patients from more marginalized neighbourhoods and those in rural areas and are driven by both surgeon-level and hospital-level factors, which implies that system or organizational changes are necessary to reduce wait times (de Jager et al. 2023, 2024).
Despite impacting the quality of life of half the population, these surgeries are not prioritized by health systems, resulting in long wait times, limited innovation and diminished healthcare experiences of both patients and providers. To address this gender bias, we examine its causes and consequences, and we propose targeted solutions to elevate gynecologic surgery within Canada's healthcare system. Because of our focus on both sex and gender bias, we use gender additive language (Brotto and Galea 2022), with both terms of woman/women and female throughout. Woman/women is used with respect to gender, recognizing that the majority of patients and surgeons in Gynecology (also commonly referred to as “women's health”) identify as women. When referring to matters of biological sex and the reproductive tract, the word female is used, holding space for gender diversity in this area of healthcare delivery.
Causes of Gender Bias in Surgery and Gynecologic Surgery
Women surgeons are underrepresented across surgical specialties. In Canada, women make up 58% of medical students but only 33% of surgeons (Schneidman et al. 2025). Gender bias in surgery is influenced by complex structural and cultural factors, including sexism, patient and hospital staff expectations of surgeons, referral patterns, operating room scheduling, the size and design of surgical equipment and unequal pay (Schneidman et al. 2025). For example, women surgeons are paid 24% less per hour than their male colleagues, most likely because women have unequal access to more lucrative surgeries due to men's referral and scheduling advantages (Dossa et al. 2019, 2022; Munir et al. 2024).
Compared with other surgical specialties, gynecologic surgery is unique because most surgeons are women and it addresses conditions that only affect people with a female reproductive tract. While it may seem like the dominance of women surgeons and patients would reduce gender bias, it exacerbates it. Three challenges that exaggerate the gender bias in gynecologic surgery are: (1) lower reimbursement rates for procedures done on women, (2) surgical scheduling and (3) surgical technology. First, in eight of 11 provinces and territories examined, the mean billing fee for procedures on the female reproductive tract was 28.1% (standard deviation 11.1%) lower than the fee for similar procedures performed on the male reproductive tract (Chaikof et al. 2023). Chaikof et al.'s (2023) study compared 22 commonly performed procedures comparable between males and females, finding that in almost 70% of cases, reimbursement was higher for procedures on male patients. The lower reimbursement rates for procedures on female patients discriminate against gynecologic surgery because all patients have female reproductive tracts, reducing the earning potential of gynecologists.
Second, surgeon gender is associated with surgery scheduling (Wright et al. 2024). Compared with women surgeons, men were significantly more likely to have overlapping cases (adjusted odds ratio [OR]: 1.66, 95% confidence interval [CI]: 1.41, 1.95), consecutively run cases (adjusted OR: 1.47, 95% CI: 1.24, 1.74), a greater number of cases per day (adjusted RR: 1.09, 95% CI: 1.07, 1.12) and shorter turnover times (adjusted RR: 1.10, 95% CI: 1.06, 1.14) (Wright et al. 2024). This scheduling and operational bias may reduce women surgeons' productivity and job satisfaction (Wright et al. 2024). Furthermore, women surgeons in Alberta were found to be more likely to have their surgeries cancelled or postponed to accommodate an emergency case compared with men surgeons (OR: 1.21, 95% CI: 1.05, 1.38) (Ruzycki et al. 2026). Given that Gynecology in Canada has an increasingly female workforce, gender issues with scheduling are disproportionately felt in this discipline.
Third, gender bias in surgical innovation is evident in multiple ways. One example is in the design of surgical instruments and the lack of technical investment (Schneidman et al. 2025). Many surgical tools are standardized for larger hands, typically those of men surgeons, leaving women surgeons – who often have smaller hands – at a disadvantage. This mismatch leads to higher rates of musculoskeletal injuries, fatigue and discomfort among women surgeons (Mesiti and Yeo 2023). For instance, women surgeons frequently need to use two hands to operate instruments designed for larger hands, which increases strain and reduces efficiency (Mesiti and Yeo 2023). Beyond ergonomics, innovation in gynecologic surgery has also lagged behind other specialties. Despite advancements such as robotic-assisted surgeries, there remains an unmet demand for safe, effective devices tailored to address complex conditions such as endometriosis and POP. These disparities are compounded by the under-representation of women in surgical leadership roles, which not only limits the uptake of female-inclusive tools (Sylla and Uzor 2023) but also affects what conditions and surgeries are prioritized by systems. These challenges in payment, scheduling and innovation contribute to Gynecology having some of the lowest earnings among surgical specialties (Dossa et al. 2019). This impacts the well-being of gynecologists, their patients and the recognition of the discipline itself.
Consequences for Patients and the Discipline
In Canada, women face prolonged suffering while waiting for gynecologic surgeries. One recent patient of this paper's author, a woman in her early 30s, endured severe POP following a difficult labor. Despite her infant being born healthy, she was left with debilitating urinary and fecal incontinence and a uterus that protruded through her vagina due to pelvic floor damage from her complicated vaginal delivery. Her condition led to the breakdown of her marriage and years of living in diapers. After years of healthcare providers repeatedly dismissing her concerns, she was finally referred for pelvic floor surgery with a urogynecologist – only to wait two and a half years for a consultation and another six months for surgery. Her story is not unique; it exemplifies the systemic disregard for gynecologic surgical needs in Canada.
One institution in Ontario identified a mean wait time of 210 days for pelvic floor surgery for POP compared with 98 days for hip or knee replacement (Leong et al. 2017); with wait times climbing to 255 days in recent years (Ontario Health 2025). Despite less physical debilitation and pain, POP patients showed similar emotional and mental distress compared with orthopaedic patients (Leong et al. 2017). As women continue to wait for gynecologic surgeries, they experience elevated levels of pain, reduced quality of life and higher mortality (Sutherland et al. 2016). Waiting for surgeries is not only a health problem; it is also a productivity problem. Women with endometriosis report reduced hours of paid work and reduced presence in household labour, which is significantly greater with increasing symptom severity (mild vs. severe: 1.9 vs 15.8 total employment hours lost and 2.5 vs 10.1 total household hours lost; p < 0.0001) (Soliman et al. 2017). Furthermore, women living with endometriosis must consider their health-related limitations when making career decisions to a much greater degree than matched women without the condition, reducing their ability to pursue their preferred career paths (OR: 4.79, 2.30, 9.96) (Sperschneider et al. 2019).
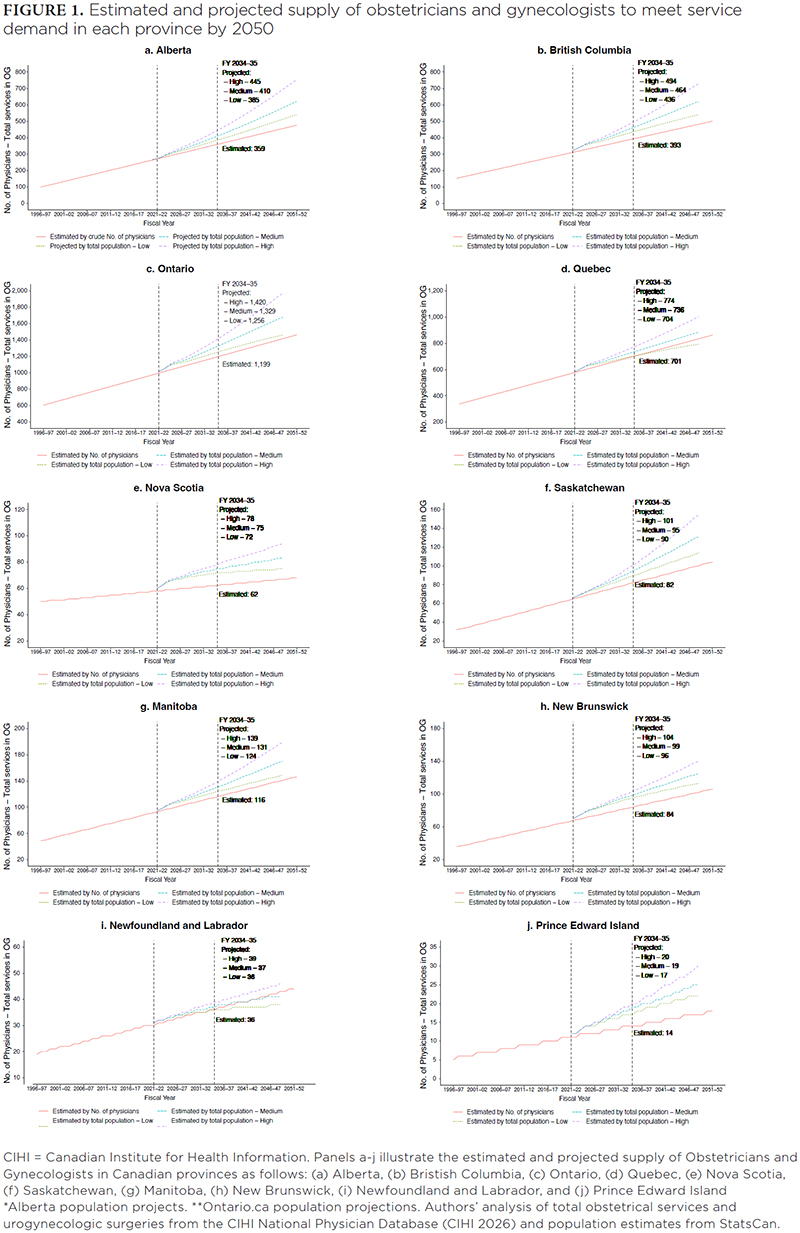
Canadian gynecologists perceive their field is not considered a “real” surgical discipline, which can further exaggerate patient wait times and recovery times due to lack of investment and interest in gynecology (Schneidman et al. 2025). Many hospital boards do not include representation from medical leaders in Gynecology on surgical decision-making committees. Gynecology often struggles to obtain investment in cutting-edge technologies, such as robotics, single-port laparoscopy and SMART operating rooms. Use of older laparoscopic equipment including towers causes wear and tear on the surgeon due to poor ergonomics, reducing the surgeon's capacity and earnings (Ghomi et al. 2022). Use of this older technology also means that an opportunity is missed for faster recovery time, less pain and fewer complications (Shahid 2024). While other surgical specialties may experience similar challenges, a mix of economic incentives, historical underinvestment in women's health and institutional decision making favours higher revenue and more prestigious procedures. The challenges surgeons and patients face may signal to medical students that the specialty is not valued, leading to reduced interest in Obstetrics and Gynecology as a specialty. Across Canada, there are already not enough obstetricians and gynecologists to meet the growing needs of the Canadian population (see Figure 1).
Potential Solutions
To address systemic gender inequities in gynecologic surgical care, we propose several evidence-based policy interventions designed for implementation by provincial health authorities, medical institutions – such as hospitals and medical schools – and surgical planning bodies.
1. Formally recognize gynecologic surgery as a core surgical discipline
Provincial ministries of health and surgical planning organizations should formally designate gynecologic surgery as a distinct surgical specialty. This recognition should be reflected in strategic plans, funding frameworks and workforce initiatives. Including gynecologic surgeons in surgical governance bodies will ensure their representation in decisions on operating room allocation, technology investment and innovation. This recognition incurs minimal direct costs but enables more equitable resource distribution, facilitates planning for gynecologic surgeon recruitment and retention and helps address workforce shortages – ultimately reducing long-term strain on the health system.
2. Reform surgical compensation and scheduling structures
Provincial health systems should begin audits of surgical fee schedules to identify and correct gender-based reimbursement disparities. Health systems should pilot equity-focused operating room scheduling approaches to reduce sex and gender-based disparities in case volume, turnover time and cancellation rates. For example, single entry models are being tested in a team-based virtual clinic to triage endometriosis referrals in the Greater Toronto Area (Shapiro et al. 2023). Although fee restructuring may increase short-term expenditures, improved parity can enhance surgeon productivity and retention – particularly among women surgeons – leading to optimized operating room efficiency.
3. Invest in inclusive surgical technology and infrastructure
Health systems should allocate funding for ergonomic surgical instruments designed for female surgeons. This will optimize patient access by avoiding ergonomic workplace injury causing days away from work, and provide an opportunity to invest in innovative technology, tools and devices to manage complex gynecologic conditions such as endometriosis and prolapse (Mesiti and Yeo 2023). Healthcare systems should also expand dedicated minor procedural suites for low-resource gynecologic surgeries (e.g., hysteroscopy, dilation and curettage), freeing traditional operating rooms for higher-complexity cases, such as endometriosis, reproductive tract cancers and pelvic floor disorders, and providing higher quality of care at a lower cost. Minor procedure suites can reduce costs by thousands of dollars per case through lower staffing requirements, shorter turnover times and elimination of anesthesia-related costs (Childers and Maggard-Gibbons 2018).
4. Strengthen primary care integration
Primary care physicians can support Gynecology by providing upstream care capable of preventing surgeries. For example, hormone-releasing intra-uterine devices (IUDs), which can be inserted in-office by primary care physicians, can reduce heavy bleeding and improve menstruation complications to delay or altogether avoid hysterectomies. Despite this potential, only 40-60% of primary care physicians are trained to insert them (Rezaiefar et al. 2025). A recent survey of 1,200 Canadian family physicians revealed that only 38% felt confident in counselling patients about IUDs, and just 42% routinely offered them as a treatment option (Rezaiefar et al. 2025). Family medicine residency programs should incorporate mandatory training in female reproductive tract procedures, including IUD insertion, endometrial biopsy and pessary care. Continuing professional development should be developed for practising primary care providers to strengthen clinical competence in women's healthcare across their lifespan. Collaborative care pathways between primary care and Gynecology should be established to facilitate early intervention and reduce demand for surgical treatment. This early intervention can reduce health system costs, wait times and improve patient outcomes.
5. Mobilize public engagement and advocacy
Patient advocacy organizations should implement public awareness campaigns highlighting the consequences of surgical neglect for women and gender-diverse populations. These campaigns could use patient narratives and data-driven messaging to shape public understanding and garner support. Participatory policy making should include patients and community stakeholders in health system governance. Women must be made aware of the quality of care they receive, empowering them to demand better from elected officials and decision makers – those with the power to shift priorities and fund infrastructure that directly benefits them.
Conclusion
Improving health system performance in Canada requires confronting the structural inequities that undermine gynecologic surgical care. The evidence is clear: delayed access to gynecologic surgery leads to avoidable suffering, economic loss and inefficiencies in surgical resource use that disproportionately affect women surgeons and patients. By formally recognizing gynecologic surgery as a core discipline, reforming compensation and scheduling, investing in inclusive technologies and new procedural spaces and strengthening primary care pathways, policy makers can unlock significant gains in system efficiency and equity. These changes will not only improve outcomes for patients seeking female reproductive healthcare but also enhance workforce sustainability and optimize operating room utilization for gynecologic surgeons. Health systems must act now – because equitable surgical care is not just a matter of performance, it is a matter of justice.
Correspondence may be directed to Amity E. Quinn by e-mail at amity.quinn@ucalgary.ca.
L'efficacité au moyen de l'équité : prioriser la chirurgie gynécologique pour améliorer la performance du système de santé
Résumé
La chirurgie gynécologique est mal desservie au Canada, malgré son volume et son impact sur le rendement du système de santé, notamment l'expérience des chirurgiennes et des patientes. Les biais structurels liés au genre dans le remboursement, la planification et l'innovation contribuent aux longs temps d'attente, à la réduction du rendement chirurgical et à une qualité réduite des soins. Cet éditorial décrit cinq stratégies pour améliorer l'efficacité du système : une reconnaissance officielle de la chirurgie gynécologique, une réforme de la rémunération et des horaires, un investissement dans des outils et infrastructures chirurgicaux inclusifs, l'intégration des soins primaires et la défense des droits publics. Donner la priorité à la chirurgie gynécologique est essentiel pour atteindre un système de santé canadien équitable et hautement performant.
About the Author(s)
Amity E. Quinn, Phd, Assistant Professor, Department of Obstetrics and Gynecology, Cumming School of Medicine, University of Calgary, Member, Sex, Gender, and Women's Health Research Hub, O'Brien Institute for Public Health, Cumming School of Medicine, University of Calgary, Calgary, AB
Erin A. Brennand, MD, MSC, Professor, Department of Obstetrics and Gynecology, Cumming School of Medicine, University of Calgary, Lead, Sex, Gender, and Women's Health Research Hub, O'Brien Institute for Public Health, Cumming School of Medicine, University of Calgary, Calgary, AB
References
Brotto, L.A. and L.A.M. Galea. 2022. Gender Inclusivity in Women's Health Research. BJOG 129(12): 1950–52. doi:10.1111/1471-0528.17231.
Canadian Institute for Health Information (CIHI). 2026. National Physician Database metadata. Accessed March 19, 2026. <https://www.cihi.ca/en/national-physician-database-metadata>.
Chaikof, M., G.W. Cundiff, F. Mohtashami, A. Millman, M. Larouche, M. Pierce et al. 2023. Surgical Sexism in Canada: Structural Bias in Reimbursement of Surgical Care for Women. Canadian Journal of Surgery 66(4): E341–47. doi:10.1503/cjs.022121.
Childers, C.P. and M. Maggard-Gibbons. 2018. Understanding Costs of Care in the Operating Room. JAMA Surgery 153(4): e176233. doi:10.1001/jamasurg.2017.6233.
de Jager, P., D. Aleman, N. Baxter, C. Bell, M. Bodur, A. Calzavara et al. 2023. Social Determinants of Access to Timely Elective Surgery in Ontario, Canada: A Cross-Sectional Population Level Study. CMAJ Open 11(6): E1164–80. doi:10.9778/cmajo.20230001.
de Jager, P., D. Aleman, N. Baxter, C. Bell, M. Bodur, A. Calzavara et al. 2024. Surgeon- and Hospital-Level Variation in Wait Times for Scheduled Non-Urgent Surgery in Ontario, Canada: A Cross-Sectional Population-Based Study. PLoS ONE 19(8): e0307845. doi:10.1371/journal.pone.0307845.
Dossa, F., A.N. Simpson, R. Sutradhar, D.R. Urbach, G. Tomlinson, A.S. Detsky et al. 2019. Sex-Based Disparities in the Hourly Earnings of Surgeons in the Fee-for-Service System in Ontario, Canada. JAMA Surgery 154(12): 1134–42. doi:10.1001/jamasurg.2019.3769.
Dossa, F., D. Zeltzer, R. Sutradhar, A.N. Simpson and N.N. Baxter. 2022. Sex Differences in the Pattern of Patient Referrals to Male and Female Surgeons. JAMA Surgery 157(2): 95–103. doi:10.1001/jamasurg.2021.5784.
Ghomi, A., W. Nolan, D.J. Sanderson, R. Sanderson, B. Schwander and J. Feldstein. 2022. Robotic Hysterectomy Compared With Laparoscopic Hysterectomy: Is It Still More Costly to Perform? Journal of Robotic Surgery 16(3): 537–41. doi:10.1007/s11701-021-01273-w.
Gomez, I., B. Frederiksen and A. Salganicoff. 2025, March 12. Women's Experiences With Preventive and Health Care Services: Findings From the 2024 KFF Women's Health Survey. Retrieved March 19, 2026. <https://www.kff.org/womens-health-policy/womens-experiences-with-preventive-and-health-care-services-findings-from-the-2024-kff-womens-health-survey/>.
Leong, Y., S. Kotani, C. Best, P. Diamond, D. Lovatsis and H. Drutz. 2017. A Comparison of Health-Related Quality of Life of Women Awaiting Pelvic Organ Prolapse Surgery Versus Hip or Knee Replacement. Journal of Obstetrics and Gynaecology Canada 39(5): 341–46. doi:10.1016/j.jogc.2017.01.005.
Mesiti, A. and H. Yeo. 2023. Surgical Device Design: Do Instruments Fit Today's Surgeons? BMJ Surgery, Interventions, and Health Technologies 5(1): e000159. doi:10.1136/bmjsit-2022-000159.
Moir, M. and B. Barua. 2024. Waiting Your Turn: Wait Times for Health Care in Canada, 2024 Report. Retrieved March 19, 2026. <https://www.fraserinstitute.org/sites/default/files/2024-12/waiting-your-turn-2024.pdf>.
Munir, M.M., M. Dillhoff, S. Tsai, C. Collins, P. Dedhia and T.M. Pawlik. 2024. Gender-Based Variations in Medicare Reimbursements Among Different Surgical Subspecialties. JAMA Surgery 159(9): 1060–70. doi:10.1001/jamasurg.2024.2298.
Ontario Health. 2025. Wait Times. Retrieved November 21, 2025. <https://www.ontariohealth.ca/system/reporting/wait-times>.
Rezaiefar, P., D. Archibald, M. Kabir and S. Humphrey-Murto. 2025. Challenges in Providing Gynecological Procedures in Primary Care: A Survey of Canadian Academic Family Physicians. Women's Health Reports 6(1): 102–12. doi:10.1089/whr.2024.0098.
Ruzycki, S.M., O. Daodu, S. Tang, M. Ejaredar, K. Lithgow, T.G. Harrison et al. 2026. Surgical Cancelations and Postponements by Surgeon and Patient Sex: A Retrospective Cohort Study in Alberta, Canada. Annals of Surgery 283(1): 130–35. doi:10.1097/sla.0000000000006439.
Schneidman, J., K. Rice and N. Armstrong. 2025. Women in Surgery: The Social Construction of Gender in Surgical Practice. The American Journal of Surgery 247: 116343. doi:10.1016/j.amjsurg.2025.116343.
Shahid, R. 2024. Innovations in Minimally Invasive Gynecological Surgery. Gynecology and Obstetrics Case Report 10(3): 26. doi:10.36648/2471-8165.10.03.26.
Shapiro, J., D. Karol, P. Bridge-Cook, C. McCaffrey, A. Murji and J. Kroft. 2023. A Team-Based, Single-Entry Model for Managing Endometriosis Referrals: An Innovative and Equitable Approach. Journal of Obstetrics and Gynaecology Canada 45(6): 393–94. doi:10.1016/j.jogc.2023.03.014.
Soliman, A.M., K.S. Coyne, K. S. Gries, J. Castelli-Haley, M.C. Snabes and E.S. Surrey. 2017. The Effect of Endometriosis Symptoms on Absenteeism and Presenteeism in the Workplace and at Home. Journal of Managed Care and Specialty Pharmacy 23(7): 745–54. doi:10.18553/jmcp.2017.23.7.745.
Sperschneider, M.L., M.P. Hengartner, A. Kohl-Schwartz, K. Geraedts, M. Rauchfuss, M.M. Woelfler et al. 2019. Does Endometriosis Affect Professional Life? A Matched Case-Control Study in Switzerland, Germany and Austria. BMJ Open 9(1): e019570. doi:10.1136/bmjopen-2017-019570.
Sutherland, J.M., R.T. Crump, A. Chan, G. Liu, E. Yue and M. Bair. 2016. Health of Patients on the Waiting List: Opportunity to Improve Health in Canada? Health Policy 120(7): 749–57. doi:10.1016/j.healthpol.2016.04.017.
Sylla, P. and N. Uzor. 2023. Women, Surgeons, and the Innovation Pipeline. Clinics in Colon and Rectal Surgery 36(5): 342–46. doi:10.1055/s-0043-1764238.
Wright, K., K. Hamilton and J. Friedman. 2024. Novel Metrics to Measure Gender Bias in Operating Room Scheduling Priority. American Journal of Obstetrics and Gynecology 230(6): e117–20. doi:10.1016/j.ajog.2024.01.025.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed