
Healthcare Quarterly
ICES Report: Large Bowel Endoscopy in Ontario: Variation by Geographic Region and Hospital Type
Abstract
This article highlights findings from the research atlas with respect to colonoscopy and flexible sigmoidoscopy among the screen-eligible (age 50-74) Ontario population. Both procedures, which at the present time are performed primarily in hospital settings, will play an important role in any future organized screening program.
Methods
Utilization of large bowel endoscopy in Ontario was examined in several ways. Temporal trends were examined for Ontario, as a whole, from 1992 to 2001, and by county, for 2001 only. To explore further the rate variation across the province, hospitals were grouped into four categories: Small (<2,500 Total Weighted Cases, or TWC), Medium (2,500-10,000 TWC), Large (>10,000 TWC) and Teaching, after which the ratio of colonoscopy volume to total hospital volume was calculated for each group. Ontario Hospital Insurance Plan (OHIP) billing data were used for all rates. OHIP endoscopy billing codes are complicated; thus, all billings for endoscopy up to the splenic flexure (codes Z555 or Z555+E740) or using the 60 cm scope (fee code Z580) were considered flexible sigmoidoscopies. Endoscopy to the hepatic flexure or beyond (Z555+E740+E741, with or without E747 and E705) was classified as a colonoscopy.For analysis by hospital type, the institution in which a colonoscopy was performed was identified by matching the OHIP record with the Canadian Institute for Health Information discharge abstract database (inpatient and same-day surgery). TWC volumes, tertiary-care volumes and hospital type for each institution were obtained from the Joint Policy and Planning Commission website at www.jppc.on.ca. Statistics Canada post-censal estimates were used for all population denominators. All rates were standardized to the 1991 Canadian population.
| Table 1: Age- and Sex-Adjusted Endoscopy Utilization Rates1 per 10,000 Ontarians 50-74 Years of Age, by Region and County, 2001 | ||
| Region and County | Colonoscopy | Flexible
Sigmoidoscopy |
| North | 463.1 | 62.7 |
| Cochrane | 641.6 | 64.5 |
| Greater Sudbury | 562.9 | 72.9 |
| Manitoulin | 536.1 | 67.1 |
| Sudbury | 480.2 | 64.4 |
| Parry Sound | 454.3 | 91.0 |
| Muskoka | 447.8 | 94.5 |
| Thunder Bay | 413.8 | 70.5 |
| Algoma | 391.0 | 25.4 |
| Timiskaming | 389.0 | 37.2 |
| Nipissing | 347.5 | 55.1 |
| Central East | 439.2 | 74.0 |
| Durham | 501.9 | 69.7 |
| Simcoe | 455.4 | 66.9 |
| Haliburton | 430.1 | 69.8 |
| York | 428.0 | 74.0 |
| Kawartha Lakes | 396.9 | 95.3 |
| Northumberland | 395.1 | 68.6 |
| Peterborough | 323.6 | 92.9 |
| Toronto | 426.9 | 84.0 |
| Toronto | 426.9 | 84.0 |
| Central West | 373.0 | 80.6 |
| Wellington | 462.8 | 68.8 |
| Halton | 426.0 | 90.6 |
| Waterloo | 380.3 | 71.9 |
| Peel | 331.3 | 78.5 |
| Dufferin | 257.7 | 156.3 |
| South West | 366.4 | 78.9 |
| Huron | 588.8 | 82.5 |
| Lambton | 576.4 | 40.6 |
| Bruce | 493.9 | 65.9 |
| Chatham-Kent | 440.2 | 55.4 |
| Perth | 412.0 | 94.4 |
| Grey | 380.6 | 82.3 |
| Essex | 334.9 | 79.7 |
| Elgin | 278.0 | 102.2 |
| Oxford | 262.6 | 120.3 |
| Middlesex | 259.8 | 82.5 |
| Central South | 322.9 | 60.6 |
| Brant | 342.8 | 99.0 |
| Niagara | 326.1 | 51.6 |
| Hamilton | 319.7 | 57.6 |
| Haldimand-Norfolk | 303.1 | 70.6 |
| East | 286.8 | 89.8 |
| Stormont, Dundas and
Glengarry |
410.0 | 99.0 |
| Hastings | 367.3 | 102.7 |
| Prince Edward | 348.4 | 52.1 |
| Prescott and Russell | 340.6 | 58.4 |
| Lanark | 291.4 | 64.4 |
| Leeds and Grenville | 277.8 | 37.6 |
| Ottawa | 254.8 | 105.0 |
| Renfrew | 233.4 | 87.7 |
| Lennox and Addington | 208.4 | 45.9 |
| Note: Frontenac
County, Rainy River District and Kenora District were excluded from
this analysis because the data for the period were
incomplete. 1Rates standardized to the 1991 Canadian population. Data sources: Ontario Health Insurance Plan; Statistics Canada Population Estimates |
||
Results
Colonoscopy utilization in Ontario has grown significantly since
1992 (Figure 1), more than doubling from 162.3 procedures per
10,000 population to 378.0/10,000 in 2001. In contrast, flexible
sigmoidoscopy rates declined slowly over the same period, from
about 100 procedures per 10,000 to 76. Table 1 shows the wide
variation in rates by county and region. The highest rates are
found in the north, the lowest in the east.
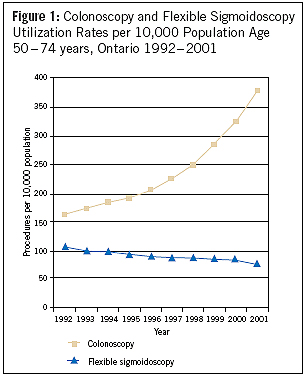
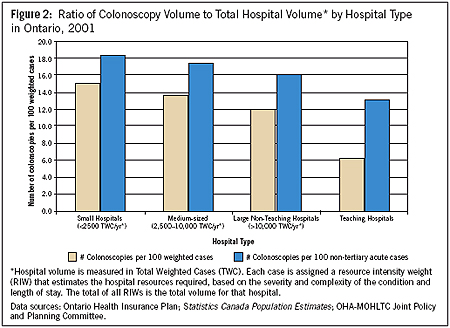
Figure 2 shows a somewhat surprising result from analysis of colonoscopy rates by hospital type in 2001. As the TWC volume of a hospital increased, the colonoscopy : total volume ratio fell. Further, the 67 smallest hospitals in Ontario had a combined total weighted case volume in 2001 of 175,989, nearly identical to the volume of 176,634 weighted cases in the two largest teaching hospitals. However, 25,163 colonoscopies were performed in the small hospitals and only 9,050 in the two largest.
Discussion
Access to large bowel endoscopy is key to any CRC screening program as the initial test or, in the case of colonoscopy, as follow-up to positive screening tests. Several aspects of the results suggest cause for concern, or further investigation of access to large bowel endoscopy.The first of these is the inverse relationship between colonoscopy : total volume ratio and hospital size. Does this mean that people living in communities served primarily by large or teaching hospitals have reduced access to colonoscopy? How do waiting times compare? This has serious implications because colonoscopy is required as follow-up to a positive initial screening test.
A second area of concern is the threefold difference in colonoscopy rates between areas with the highest and lowest rates. Again, does this reflect an access problem, or do physicians prefer other large bowel evaluation techniques in these areas?
Finally, declining rates of flexible sigmoidoscopy indicate underutilization of a procedure that has been endorsed as an initial screening test and can readily be performed in office settings. Several disincentives to performing flexible sigmoidoscopy have been discussed, most notably, the lack of an assigned Resource Intensity Weight, which excludes it from cost allocation or funding equations (Vinden et al. 2004). As well, the low technical or facility fee paid by OHIP for flexible sigmoidoscopy or colonoscopy performed outside hospitals is a barrier to access. All of these issues need to be addressed as Ontario prepares for a province-wide CRC screening program.
About the Author(s)
Susan Schultz is research coordinator at the Institute for Clinical Evaluative Sciences.
Dr. Linda Rabeneck is Professor of Medicine and Director of Gastroenterology at the University of Toronto; Head, Division of Gastroenterology at Sunnybrook and Women's College Health Sciences Centre (SWCHSC); Senior Scientist at the Institute for Clinical Evaluative Sciences.
Dr. Chris Vinden is Assistant Professor of Surgery at the University of Western Ontario and an Adjunct Scientist at the Institute for Clinical Evaluative Sciences.
References
Canadian Task Force on Preventive Health Care (CTFPHC). 2001. "Colorectal Cancer Screening: Recommendation Statement from the Canadian Task Force on Preventive Health Care." Canadian Medical Association Journal 165(2): 206-08.
National Cancer Institute of Canada (NCIC). 2003. Canadian Cancer Statistics, 2003. Toronto, Canada.
Vinden, C., S. Schultz and L. Rabeneck. 2004. ICES Research Atlas: Use of Large Bowel Procedure in Ontario. Toronto: Institute for Clinical Evaluative Sciences.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Note: Please enter a display name. Your email address will not be publically displayed