
Healthcare Quarterly
Taking Aim at Fall Injury Adverse Events: Best Practices and Organizational Change
Patricia O'Connor, Joann Creager, Sharon Mooney, Andrea Maria Laizner and Judith A. Ritchie
Abstract
Fall injuries represent a huge healthcare, social and financial burden to the Canadian population. In 2004, the McGill University Health Centre (MUHC) was awarded recognition as a National Spotlight Organization for Implementation of the Registered Nurses Association of Ontario Best Practice Guidelines (BPGs). That same year, the author and co-leader of the Best Practice Guideline Program began the CHSRF Executive Training in Research Application (EXTRA) Program with the goal of reducing falls injuries, one of the most common adverse events in the MUHC and in acute care in Canada. This demonstration project used multiple strategies to strengthen a culture of safety and improve performance relating to adverse events, including: pilot testing several evidence-based falls prevention interventions (autumn 2005), training teams of champions to work across multiple sites, developing an infrastructure to support organizational change, modifying existing quality indicators to become benchmarkable, conducting a cost analysis of falls prevention, evaluating pre- and post-pilot surveys of organizational climate and obtaining initial baseline measures of the safety climate within the organization. Positive patient, practitioner and organizational outcomes suggest that falls safety prevention is feasible in large, complex healthcare organizations - and that safety is both a moral and a financial imperative. Next stages of the BPG program include full rollout, and measuring sustainability via a formal outcome evaluation study.
Background
Falls are the sixth leading cause of death in Canada, account for 20% of all injury-related deaths among seniors in Canada, and add an estimated annual direct cost of $2.4 billion (Canadian Institute for Health Information 2002). The incidence of falls among elderly hospitalized patients is greater than that among older persons living in the community. Several researchers (Morse 2002; Halfon et al. 2001) have reported a range of fall rates (per 1,000 bed days) as 2.2 to 7 in acute care hospitals, 11.0 to 24.9 in long-term-care hospitals, and 8.0 to 19.8 in rehabilitation hospitals. Injury rates have been reported to be 29-48% of falls, with 4-7.5% resulting in serious injuries. Many hospital falls are judged to be preventable: an Australian study found that 62% of hospital falls were preventable (Wilson et al. 1995). Research on falls prevention in acute care is limited, but there is compelling evidence from systematic reviews, meta-analyses and primary research studies in nursing homes and community-dwelling seniors demonstrating that falls can be prevented through timely risk detection and appropriately skilled management (Hanger et al. 1999; Close et al. 1999; Leipzig et al. 1999; Lord et al. 2003; Healey et al. 2004; Hill et al. 2004; Bischoff-Ferrari et al. 2005; Gillespie et al. 2003; McClure et al. 2005). The major fall risk factors are diverse, and many - balance impairment, muscle weakness, excessive or suboptimal medication use and environmental hazards - can be modified.
Falls are the most commonly reported incident at the McGill University Health Centre (MUHC), an organization that is a merger of five acute care teaching hospitals (four adult, one pediatric). Approximately 1,150 falls are reported annually at the MUHC; 33% result in injury causing harm and 1.4% cause permanent injury. There is no information on the annual economic impact of falls at the MUHC, aside from settlement costs. Between 2001 and 2004, settlement costs totalled $4.6 million for 15 cases, and in 2005 there was an accidental death related to a fall. Another indirect fall-related cost involves use of constant observation (about $1.7 million per year at MUHC).
The Issues
While some units had already implemented excellent falls prevention measures, a systematic, evidence-informed organizational approach to falls prevention was lacking at MUHC. This posed important risks related to patient safety, legal liability and financial burden. The size (12,000 staff) and complexity of the merged organization, a history of strong cultural differences between sites, and the lack of benchmarked fall performance indicators were key issues.
In 2003, as part of the quality and safety initiatives of the MUHC Nursing Department, three nurse-sensitive outcome indicators were targeted for improvement: falls, pressure ulcers and pain management. In January 2004, the department was designated as one of nine national spotlight organizations for the implementation of the Registered Nurses Association of Ontario Best Practice Guidelines (RNAO BPGs) (2006). In August 2004, O'Connor began a two-year Fellowship in the Canadian Health Services Research Foundation's EXTRA (Executive Training in Research Application) Program. Her intervention project focused on fall injury reduction and strengthening a culture of safety through collaboration with the newly created Falls Prevention Task Force co-led by Creager and Mooney. The results of these collaborations are reported here.
Goals. The interdisciplinary falls prevention program, begun in autumn 2004 with the launch of a falls prevention task force (FPTF), had two goals: (1) implement a falls prevention best practice guideline in order to achieve a 20% reduction of in-patient fall injuries by 2007 and (2) utilize numerous multilevel strategies to increase organizational awareness of patient safety and adverse events, and strengthen a culture of safety.
Approach
We used the PARIHS conceptual framework to guide our knowledge transfer work. The model, Promoting Action on Research Implementation in Health Services (Kitson et al. 1998; Rycroft-Malone et al. 2004), proposes that three factors influence successful uptake of evidence into practice: the nature of the evidence being used, contexts that are receptive to change and the appropriateness of the facilitation strategies utilized.
Implementing Best Practices
Assessing organizational readiness for change is a first step for successful change management. Feedback during preliminary BPG awareness workshops revealed widespread nurse enthusiasm to improve basic nursing practice. There was multilevel buy-in for falls safety changes from the CEO and board of directors to the managerial ranks and Council of Nurses quality committees. A key resource for facilitating practice changes was the large cohort of nurse educators and clinical nurse specialists who had experience with knowledge transfer. While some units had falls prevention programs, clinicians on many other units had low awareness of the prevalence of falls risk and of appropriate interventions. There was no single tool in wide use for risk assessment or documentation of prevention efforts. As a recently merged institution, leadership had little experience with effectively introducing practice change across multiple sites. These factors indicated the need for a clear, multipronged implementation plan.
Undertaking such large and complex change is impossible without considerable infrastructure support. The RNAO "spotlight" designation provided $100,000 in funding, used primarily to ensure paid release time of unit staff for education, an important condition for manager buy-in. The RNAO falls prevention BPG, based on critical appraisal of existing evidence, provided a "ready to go" product from a credible source. Other supportive features included: (1) executive co-leadership of the BPG Program, and creation of a BPG steering committee, (2) workshops to train facilitators such as our "advocates" (change agents who work across sites providing coaching and guidance) and "unit-based champions," (3) embedding researchers and senior managers on each task force - an innovation that brought rigour and practicality to the teams, (4) linking these efforts with existing quality and practice committees, the nursing Executive and the Council of Nurses and (5) multiple communication strategies.
An interdisciplinary falls prevention task force, developed in 2004, was responsible for: (1) identifying baseline fall rates, (2) selecting performance indicators and targets (autumn 2004), (3) piloting falls prevention interventions on four units for 6-8 weeks (autumn 2005), (4) evaluating and communicating the results and (5) recommending changes for diffusion (winter-spring 2006) and rolling out the implementation across the hospital. The pilot units included two internal medicine units and two long-term-care units.
[Table 1]
The summary of the falls prevention interventions that we promoted and our methods of evaluation are listed in Table 1. The Morse Falls Risk Assessment Tool (1997) was used to provide a simple, valid and reliable measure of fall risk based on specific risk factors. These evidence-based practice changes were promoted through formal, falls prevention interactive learning activities, and use of decision-support pocket tools and posters and other incentives (BPG buttons, bags and lanyards). The task force co-chairs supported the unit-based champions throughout the piloting process via frequent unit meetings to discuss progress and troubleshoot.
Multiple Strategies to Strengthen a Culture of Safety
Improving patient safety is primarily a culture change. Many healthcare organizations are treating adverse events as a technical challenge, but the larger challenge lies in transforming the work and the patterns of behaviour that have developed around the work (Baker 2005). Creating and sustaining a culture of safety occurs when organizations place as high a priority on safety as they do on production (fiscal performance). In addition to implementing best practice guidelines, our strategies were aimed at increasing awareness, developing a falls safety business case and improving corporate monitoring systems.
Increasing Safety Awareness. Several methods were used to increase safety awareness. Surveys pre- and post-implementation of the falls BPG on four pilot units elicited staff perceptions regarding: organizational culture, support for BPGs, safety climate, worth of the BPGs, changes in practice and educational support. Multiple knowledge exchange sessions were held on a range of safety issues (adverse events, falls prevention, sentinel events, root cause analysis, workplace quality indicators). We targeted multiple groups in these sessions: the public, CEO, Board of Directors Quality Committee, executive teams, managers, clinical nurse specialists, educators, practitioners, pharmacy, technical services and groups with quality mandates.
Developing a Business Case for Falls Safety. Another aspect of our falls prevention program included tabling a business case (cost analysis) for falls prevention to senior management and the Board of Directors Quality Committee. Rather than undertaking a lengthy study with matched controls to determine the MUHC fall injury costs, our approach was more pragmatic. We projected costs based on existing evidence about the following factors: physician service costs, average increased length of stay for fall injuries in acute care, average costs for hip fracture injuries, fracture rate within the MUHC, costs for safety equipment and estimated avoidable patient days based on potential rates of fall injury prevention. An audit of falls prevention equipment was also conducted across the five sites to identify and cost needed resources. Multiple external funding sources were sought to support best practice implementation.
Modifying Corporate Reporting of Falls and Fall Injuries. Comparing fall rates among different institutions was difficult because of varying definitions, reporting methods, types of settings and populations and lack of risk adjustment. In 2004, the MUHC was reporting fall occurrences, not fall rate, making external benchmarking comparisons difficult. The most commonly used statistic allowing benchmarking comparisons to measure falls is the "fall rate," the number of falls per 1,000 patient days. Our falls severity measure included categories too numerous and overlapping. In Quebec, incidents are currently reported by means of a single-page provincial reporting tool, which is inadequate for assessing whether falls prevention practices were in place when the fall occurred. Representatives of the falls task force and the MUHC Quality Department together focused on revising internal fall reporting systems, modifying the provincial tool and reducing gaps in accurate identification of fall adverse events.
Results
Piloting Best Practice Guideline
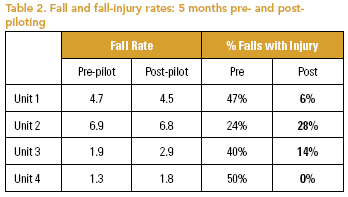
Falls and Fall Injuries. Table 2 shows the results of fall rates and injury rates in the five-month period prior to and after the pilot implementation of the falls prevention BPG. While falls did occur on all four units, the more significant improvement was in the rate of fall injuries. On units 3 and 4, the fall rates increased slightly, but they remained quite low, and there were significant improvements in injury rates. All post-pilot fall injuries on units 1-3 resulted in only minor injuries (bruising/abrasions), and the six falls occurring on unit 4 resulted in no injuries.
Focus Group and Chart Audit Results. Audits showed the Morse tool was usually completed at time of admission and after a transfer. Staff found it easy to complete. There was some variability in scoring during training sessions, resulting in descriptive prompts being added to the charting tool. Feedback from nurses illustrated the usefulness of the Morse tool - for example, "It catches my attention" and "It leads me to see the patient earlier - at the start of the shift." An individualized risk factor documentation tool, designed by the task force to chart fall interventions linked to patient risk factors, was seen as too time-consuming and detailed by practitioners on the acute care units. The reformatted and re-piloted version has received very favourable reviews, and has been prepared for wide implementation. The CATT tool denotes the times for assessment - Change in status, Admission, Transfer or after a Tumble (fall) - and includes a Morse score, risk profile and fall intervention charting. Interdisciplinary debriefings following falls occurred more consistently in the long-term-care areas, and staff on all pilot units indicated they were much more aware of the interventions that needed to be modified. In most cases the appropriate interventions were in place.
Ongoing facilitation provided by the advocates and task force co-chairs and the internal support from the unit-based champions were seen as crucial by staff and managers alike. These interactions, largely informal but frequent, allowed for problem-solving when obstacles were met, ongoing encouragement and high visibility for the project. Given the constant barrage of competing priorities for staff at the unit level, they found the regular positive feedback and communication essential.
Staff Surveys. Survey results are expressed with simple mean score ranges for the four units. Staff perceived a fairly open culture for change (2.7-2.8 /4), the highest ratings being given for: morale, openness of team to try new things and having a feeling of "Let's get things done" and that their manager was an advocate for nursing in the hospital. Lowest scores related to work overload. Organizational support for the BPG was rated slightly higher (2.9-3 /4), the best scores being given for: management support of the BPG, nurses' belief they had the time/training to learn to use the BPG and readily adopting the changes required. Lowest scores related to inadequate supplies/equipment to implement the BPG. Staff perceptions of safety climate were positive, with small increases post-pilot (3.8-4.1 /5). The acute care units had a somewhat more negative perception of worth (6.8-8 /10) and facilitation (2.6-2.9 /4), possibly due to unwieldiness of the original falls risk factor assessment tool designed for the pilot units. Nurses perceived improvements in their ability to assess and manage 13 fall risk factors post-pilot. The units infrequently reviewed medications with pharmacists and physicians - an important target area for interdisciplinary collaboration. Limitations of these results include a lower response rate for two units post-pilot, and nonmatching staff responding pre- vs. post-pilot.
Environmental, Equipment and Medication Audits. Our audits identified faulty equipment/patient furniture posing fall hazards. In long-term-care units, clutter from patients' personal belongings was the most common problem. There was a significant lack of appropriate fall risk reduction equipment on all pilot units - for example, bedrail bumper pads, wedge cushions, bed and chair alarms and nonskid socks. During the pilot we were successful in obtaining funds from the hospital foundation and volunteers to purchase safety devices for these units. Polypharmacy, defined as taking more than five medications, was very common (97% of patients) and there was significant use as well of benzodiazepines and antidepressants (59%).
Results of Strategies to Strengthen Culture of Safety
Knowledge Exchange Sessions. While difficult to fully evaluate the results, the high attendance rate at the many safety sessions was significant and feedback, though informal, was very positive. Another important result was buy-in from the unions, including their financial support for advancing the best practice guideline implementation program and requests to have presentations at their union-management meetings. Sessions held with managers, and the various safety audits in particular, resulted in greater awareness of the potential to reduce falls.
Business Case for Fall Safety. Bates (1995) estimated the cost for falls occurring in acute care as averaging $4,230 (in 1995, in US) for physician services, with lengths of stay extended an average of 12 days. VHA statistics for hip fracture injuries after a fall indicate an average cost of $34,000, and an increased length of stay of 17 days. Assuming approximately 11 MUHC hip fractures/year based on current rates, this represents an annual cost of approximately $374,000. The identified cost for new fall safety equipment is approximately $200,000 ($5,000/unit). It becomes clear that the preventable cost associated with one year of fall injuries exceeds the cost to properly outfit all care units. There are even more important savings vis-à-vis patient days if adverse events such as fall injuries were reduced (improving access for other care). The MUHC's current rate of 33% fall injuries (378 falls) - and potentially lengthened stays of 12 days - represents 4,554 avoidable patient days. Assuming at least half of these falls were preventable, this would mean 2,277 bed days potentially available for other admissions. An important consequence of performing the various audits (environmental, equipment, fall safety devices) and involving many managers was the managers' increased awareness of the potential to reduce falls.
Obtaining adequate resources for falls prevention was a key priority. Funding obtained includes: (1) $75,000 from the Canadian Nurses Foundation and partners for a formal evaluation study of further BPG implementation, (2) $200,000 received from the provincial Ministry of Health for work reorganization relating to best practices and (3) $55,000 from MUHC Foundations for falls safety equipment purchases. These funds allowed the recent hiring of a project manager - a much-needed support. An evaluation of patient beds was also conducted in collaboration with the falls task force, resulting in a long-term replacement plan and partial funding to begin replacement.
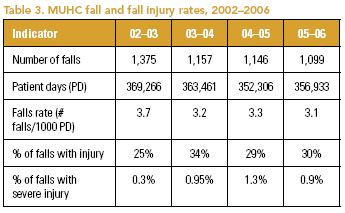
Modified Corporate Reporting of Falls and Fall Injuries. Table 3 illustrates the conversion of fall occurrences into a falls rate and percentage of falls with injury, for the combined adult and pediatric sites. Rate comparisons, internal and with external benchmarks, are now possible. The anticipated fall rate reductions following the introduction of BPGs will only be evident in 2006-2007, when rollout is occurring across many units.
Conclusions
Our experiences confirmed work by others (Bero et al. 1998; Solberg et al. 2000) that effecting organizational changes requires the use of multilevel, bundled interventions - and it is a messy process. Staff indicated falls prevention is a priority in their practice, and that the BPG content and processes used were valuable. The results suggest improvements in practice and in patient outcomes. It is clear that commitment to reducing falls involves: changing staff and client behaviour, systematic organizational changes, coalition-building and closing the gap between corporate safety values and operationalization to the front line. Ultimately, safety is both a moral and a financial imperative, requiring dedicated resources for basic equipment, information systems, learning activities and paid release time of clinically expert change agents who are needed for the ongoing facilitation of practice changes. This is crucial, as competing priorities easily dissipate the focused attention required to sustain such changes. The alignment of this best practices initiative with key corporate safety priorities has encouraged many clinical leaders from different disciplines to begin working in a more systematic and cohesive manner. A systematic review of evidence on sustainability of innovations (NHS Modernization Agency 2002; Greenhalgh et al. 2004) confirms these variables as key to successful change.
Lessons Learned
Factors affecting successful change at MUHC included: extensive stakeholder analysis and engagement including support departments such as finance, technical services/housekeeping, and risk management in addition to the usual frontline clinical disciplines and executive levels; ongoing training of champions at the unit and cross-site level; creating infrastructure to support organizational change; and clear timelines. Manager buy-in was key; it required many rounds of consultation, and flexibility in making adjustments while setting realistic limits. Breakdown in communication in such a large system was common and needed constant attention. Access to resources was an obstacle, and sources both external and internal were still required. Embedding both researchers and senior managers on the falls task force was an innovation that brought rigour and practicality to the teams. Having appropriate systems in place to evaluate the effectiveness of change provides critical feedback throughout the system to support sustainability. Celebrating successes and small, incremental wins at every possible step has been a deliberate strategy, along with continuous communication of results both internally and internationally.
Future Directions
The new corporate monitoring systems will allow for more accurate rate comparisons internally and with external benchmarks. In 2006-2007, pediatric and adult data will be reported separately. Plans are under way to streamline fall injury reporting, noting presence/absence of injury and percentage with severe injury. Recommendations have also been made for improving the provincial incident reporting system. Medication management as it relates to reducing risk of falls is an area requiring further practice review.
Despite the many challenges, we have made remarkable progress, and have concluded that the pilot implementation was successful. We have seen many unanticipated benefits, as new leaders are emerging with stronger skills in project management, flexibility and collaboration, political awareness and public relations, and knowledge transfer. We also are seeing an improvement in the discourse in the organization toward a culture of evidence-based decision-making and patient safety.
About the Author(s)
Patricia O'Connor, RN, MSc(A), CHE, is Associate Director of Nursing, Neurosciences and MUHC Best Practice Guidelines Program Co-Leader, McGill University Health Centre, and Assistant Professor, McGill University School of Nursing.
Joann Creager, RN, MSc(A), is Clinical Nurse Specialist, Geriatrics, MUHC Co-chair Falls Prevention Task Force, McGill University Health Centre, and Lecturer, McGill University School of Nursing.
Sharon Mooney, RN, MA, is Nurse Professional Development Educator, MUHC Co-chair Falls Prevention Task Force, McGill University Health Centre, and Lecturer, McGill University School of Nursing.
Andrea Maria Laizner, RN, PhD, is Nursing Research Consultant, McGill University Health Centre, and Assistant Professor, McGill University School of Nursing.
Judith A. Ritchie, RN, PhD, is Associate Director for Nursing Research, MUHC Best Practice Guidelines Program Co-Leader, McGill University Health Centre, and Associate Professor, McGill University School of Nursing.
Correspondence may be directed to: Patricia O'Connor, Associate Director of Nursing, MUHC, Montreal Neurological Hospital, 3801 University Street, Room 166, Montreal, QC H3A 2B4. Tel: 514-398-1962. Fax: 514-398-8433. E-mail: patty.oconnor@muhc.mcgill.ca
References
Aiken, L., S. Clarke, D. Sloane, J. Solcholski and J. Silber. 2002. "Hospital Nurse Staffing and Patient Mortality, Nurse Burnout, and Job Dissatisfaction." Journal of the American Medical Association 288: 1987-93.
Baker, R. 2005. "EXTRA Program, Module 5." Canadian Health Services Research Foundation. August. Banff, AB.
Baker, R., P. Norton, V. Flintoft, R. Blais, A. Brown, J. Cox, E. Etchells, W. Ghali, P. Hebert, S. Majumdar, M. O'Beirne, L. Palacios-Derflingher, R. Reid, S. Sheps and R. Tamblyn. 2004. "The Canadian Adverse Events Study: The Incidence of Adverse Events among Hospital Patients in Canada." Canadian Medical Association Journal 170(11): 1678-86.
Bates, D., K. Pruess, P. Souney and R. Platt. 1995. "Serious Falls in Hospitalized Patients: Correlates and Resource Utilization." American Journal of Medicine 99: 137-43.
Bero, L.A., R. Grilli, J.M. Grimshaw, E. Harvey, A.D. Oxman and M.A. Thomson. 1998. "Closing the Gap between Research and Practice: An Overview of Systematic Reviews of Interventions to Promote the Implementation of Research Findings." British Medical Journal 317: 465-68.
Bischoff-Ferrari, H.A., W.C. Willet, J.B. Wong, E. Giovannucci, T. Dietrich and B. Dawson-Hughes. 2005. "Fracture Prevention with Vitamin D Supplementation: A Meta-analysis of Randomized Controlled Trials." Journal of the American Medical Association 293: 2257-64.
Canadian Institute for Health Information (CIHI). 2002. "Falls Leading Cause of Injury Admissions to Canada's Acute Care Hospitals." CIHI Report. Retrieved August 18, 2006. http://www.cihi.ca/cihiweb/ dispPage.jsp?cw_page=media_27feb2002_e
Carnino, A. 2004. "Management of Safety, Safety Culture, and Self Assessment. International Atomic Energy Agency site." Retrieved August 18, 2006. http://www-ns.iaea.org/publications/ mng-safety.htm
"Clinical Practice Guideline for the Assessment and Management of Falls in Older People." 2004. National Collaborating Centre for Nursing and Supportive Care. November. London (UK): National Institute for Clinical Excellence.
Close, J.C.T., M. Ellis, R. Hooper, E. Glucksman, S. Jackson and C. Swift. 1999. "Prevention of Falls in the Elderly Trial (PROFET): A Randomised Controlled Trial." Lancet 353: 93-97.
Conn, Joseph. 2005. "Leading Indicator." Modern Healthcare, August 15, pp. 38-39. Retrieved August 18, 2006. http://www.qiproject.org/index.asp?cmd=general_info
Edwards, N., B. Davies, E. Danesco, D. Pharand, L. Brosseau, J. Ploeg and V. Bharti. 2004. "Evaluation of Nursing Best Practice Guidelines: Organizational Characteristics." CHRU Publication No. M04-2.
Gerontological Nursing Interventions Research Center. 2004. "Falls Prevention for Older Adults." University of Iowa College of Nursing site. February. Retrieved August 18, 2006. http://www.nursing.uiowa.edu/ centers/gnirc/protocols.htm
Gillespie, L.D., W. Gillespie, M.C. Robertson, S.E. Lamb, R.G. Cumming and B.H. Rowe. 2003. "Interventions for Preventing Falls in Elderly People." The Cochrane Database of Systematic Reviews, Issue 4, Art. No. CD000340. DOI: 10.1002/14651858. Oxford: Update Software.
Greenhalgh, T., R. Glenn and P. Bate. 2004. "How to Spread Good Ideas: A Systematic Review of the Literature on Diffusion, Dissemination and Sustainability of Innovations in Health Service Delivery and Organization." NHS, Service Delivery Organization (SDO) site. http://www.sdo.lshtm.ac.uk/pdf/ changemanagement_greenhalgh_report.pdf
Halfon, P., Y. Eggli, G. Van Melle and A. Vagnaire. 2001. "Risk of Falls for Hospitalized Patients: A Predictive Model Based on Routinely Available Data." Journal of Clinical Epidemiology 54(12): 1258-66.
Hanger, H.C., M.C. Ball and L.A. Wood. 1999. "An Analysis of Falls in the Hospital: Can We Do without Bedrails?" Journal of American Geriatrics Society 47(5): 627-28.
Healey, F., A. Monro, A. Cockram, V. Adams and D. Heseltine. 2004. "Using Targeted Risk Factor Reduction to Prevent Falls in Older In-patients: A Randomized Control Trial." Age and Aging 33(4): 390-95.
Hill, K., F. Vrantsidis, B. Haralambous, M. Fearn, R. Smith, K. Murray and J. Sims. 2004. "An Analysis of Research on Preventing Falls and Fall Injury in Older People: Community, Residential Care and Hospital Settings." Report by the National Ageing Research Institute to the Australian Government, Department of Health and Ageing, Injury Prevention Section. Retrieved August 18, 2006. http://www.health.gov.au/internet/wcms/Publishing.nsf /Content/health-pubhlth-publicat-document- falls_community-cnt.htm
IOM (Institute of Medicine). 2000. To Err Is Human: Building a Safer Health System. Washington, DC: National Academy Press.
IOM (Institute of Medicine). 2004. "Keeping Patients Safe: Transforming the Work Environment of Nurses." Washington, DC: National Academy Press. Pp. 53-64.
Jeffs, L., M. Law, R. Baker and P. Norton. 2005. "Patient Safety Research in Australia, United Kingdom, United States and Canada: A Summary of Research Priority Areas, Agenda-Setting Processes and Directions for Future Research in the Context of Their Patient Safety Initiatives." Prepared for the Canadian Patient Safety Institute, Canadian Health Services Research Foundation and the Canadian Institutes of Health Research for the research priority-setting retreat, February 28-March 1, 2005.
Kitson, A., G. Harvey and B. McCormack. 1998. "Enabling the Implementation of Evidence-Based Practice: A Conceptual Framework." Quality in Health Care 7: 149-58.
Leipzig, R.M., R.G. Cumming and M.E. Tinetti. 1999. "Drugs and Falls in Older People: A Systematic Review and Meta-Analysis: II. Cardiac and Analgesic Drugs." Journal of American Geriatrics Society 47(1): 40-50.
Lord, S.R., S. Castell, J. Corcoran, J. Dayhew, B. Matters, A. Shan and P. Williams. 2003. "The Effect of Group Exercise on Physical Functioning and Falls in Frail Older People Living in Retirement Villages: A Randomized, Controlled Trial." Journal of the American Geriatrics Society 51(12): 1685-92.
McClure, R., C. Turner, N. Peel, A. Spinks, E. Eakins and K. Hughes. 2005. "Population-Based Interventions for the Prevention of Fall-Related Injuries in Older People." Cochrane Database of Systematic Reviews, Issue 1, Art. No. CD004441.pub2. DOI: 1002/14651858.
Morse, J.M. 1997. Preventing Patient Falls. Thousand Oaks, CA: Sage Publications.
Morse, J. 2002. "Enhancing the Safety of Hospitalization by Reducing Falls." American Journal of Infection Control 30(6): 376-80.
National Quality Forum. 2006. Website. Retrieved August 18, 2006. http://www.qualityforum.org
Needleman, J., P. Buerhaus, S. Mattke, M. Stewart and K. Zelevinsky. 2002. "Nurse-Staffing Levels and the Quality of Care in Hospitals." The New England Journal of Medicine 346(22): 1715-22.
NHS Modernisation Agency. 2002. "Research into Practice Program: Improvement Leaders' Guide to Sustainability and Spread." http://www.modern.nhs.uk
Registered Nurses Association of Ontario (RNAO). 2006. "Nursing Best Practice Guidelines." RNAO site. http://www.rnao.org/bestpractices/index.asp
Rycroft-Malone, J., G. Harvey, K. Seers, A. Kitson, B. McCormack and A. Tichen. 2004. "An Exploration of the Factors That Influence the Implementation of Evidence into Practice." Journal of Clinical Nursing 13: 913-24.
Seago, J. 2001. "Nurse Staffing, Models of Care Delivery, and Interventions." In K. Shojania, B. Duncan, K. McDonald and R. Wachter, eds., Making Health Care Safer: A Critical Analysis of Patient Safety Practices. Evidence Report/Technology Assessment No. 43. Rockville, MD: AHRQ.
Solberg, L., M. Brekke, C. Fazio, J. Fowles, D. Jacobsen, T. Kottke, G. Mosser, P. O'Connor, K. Ohnsorg and S. Rolnick. 2000. "Lessons Learned from Experienced Guideline Implementers: Attend to Many Factors and Use Multiple Strategies." Journal on Quality Improvement 26(4): 171-88.
Thomas, L., N. Cullum, E. McColl, N. Rousseau, J. Soutter and N. Steen. 1999. "Guidelines in Professions Allied to Medicine (Cochrane review)." The Cochrane Library, Issue 3. Oxford: Update Software.
VA National Center for Patient Safety. 2004. "Falls Toolkit." National Center for Patient Safety site. http://www.patientsafety.gov/ SafetyTopics/fallstoolkit/index.html
Wilson, R., B. Runciman, R. Gibberd, B. Harrison, L. Newby and J. Hamilton. 1995. "The Quality of Australian Health Care Study." Medical Journal of Australia 163: 458-71.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Note: Please enter a display name. Your email address will not be publically displayed