
Healthcare Quarterly
Using Human Factors Methods to Evaluate the Labelling of Injectable Drugs
Kathryn Momtahan, Catherine M. Burns, Sylvia Hyland, Jennifer Jeon and Sandra Gabriele
Abstract
Adverse drug events, including in-hospital medication errors, are a well-documented world-wide problem. This interdisciplinary team set out to examine the issues related to the labelling of injectable drugs. We sought answers to the following two questions: (1) To what extent do injectable drug labels adhere to existing Canadian design practice recommendations and regulations for labelling and (2) is there a need to make changes to the recommendations or regulations for labelling of injectable drugs in Canada? The project contained three phases. The first phase involved taking a sample of vials and ampoules from a hospital pharmacy and identifying adherence to the 1999 Canadian Standards Association standard for the labelling of drug ampoules, vials and prefilled syringes, as well as with the Canadian (Health Canada) Food and Drug Regulations for labelling. The second phase involved a failure mode and effects analysis of the label-reading process in order to identify information on the label considered critical for safe medication use. The third phase involved a preliminary human factors experiment addressing one problem identified with existing labels. Our finding is that existing injectable drug labels do not adhere sufficiently to available best design standards for labels and also do not adhere to all Canadian Food and Drug Regulations. Recommendations are made to inform future enhancements to labelling standards, guidelines and regulations.
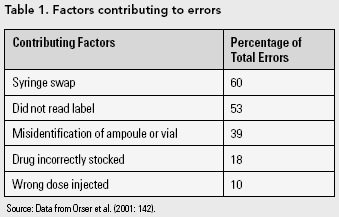
Poor labelling of injectable medications can be a contributing factor to medication errors leading to adverse drug events. In 2001, Orser et al. reported the results of a survey they conducted regarding medication errors in anesthesia practice. The researchers received survey responses from 687 anesthesiologists who reported knowledge of a total of 1,038 medication errors. The anesthesiologists were asked to identify factors that they felt contributed to the errors. Table 1 provides a list of these factors. In this same survey, 84% of the anesthesiologists agreed that improved standards for drug labels would reduce the incidence of error.
In an analysis of medication errors reported to the United States Pharmacopoeia (USP) voluntary Medication Errors Reporting Program for a one-year period between 1996 and 1997, the USP found that 33% of the reports cited labelling or packaging as having contributed to the medication error (USP 1998). In nearly 30% of the fatalities reported, labelling or packaging was cited as a contributing factor to the medication error that led to the fatality. The types of problems listed were the following:
- Lack of prominent placement of drug name and strength
- Small size and poor readability of printed information
- Insufficient prominence given to route of administration (e.g., nasal versus injection, intravenous versus intramuscular)
- Poorly designed or cluttered labels
- Lack of differentiation between drug products that have similar names
- Similar-appearing labels or packages of different products
- Poor use or absence of colour to differentiate products
- Prominence of company logos versus information that identifies the product
- Inadequate warnings about proper drug use
There are several extensive reviews of the causes of medication errors and possible solutions to medication system designs (e.g., Berman 2004; Cohen 2007; Institute of Medicine of the National Academies 2007). Medication label design is an area where the consideration of human factors principles is critical (Greenall et al. 2004). Confusing drug labels have been identified as a contributing factor to medication errors across different disciplines in medicine (Ashcroft et al. 2005; Cohen 1999, 2007; Kenagy and Stein 2001; Orser and Oxorn 1994). Injectable drugs, in particular, were found to be the most common dosage form associated with medication errors that resulted in patient death reported to the US Food and Drug Administration from 1993 to 1998 (Phillips et al. 2001). Furthermore, injectable drugs were involved in more than half the medication error reports submitted by hospital pharmacists to the USP Drug Product Problem Reporting program between 1995 and 1999 (USP 2000).
Phase One: Existing Manufacturer Labels and Adherence to Current Standards and Regulations
The Canadian Standards Association (CSA) published a standard in 1999, CAN/CSA-Z264.2-99, for the labelling of drug ampoules, vials and pre-filled syringes (CSA 1999). The Canadian Anesthesiologists' Society, the Canadian Society of Hospital Pharmacists, the Centre for Health Promotion and the Institute for Safe Medication Practices were key groups involved in the development of the standard. The standard defines minimum design requirements for the presentation of information on the inner label for injectables and complements the requirements in the Canadian Food and Drug Regulations (Government of Canada 2006). The inner label is the label on, or affixed to, the immediate container of a drug product.
The CSA standard focuses on ensuring the organization and the legibility of label content, especially for what it calls "critical information": the drug product's common name(s) in English and French and the total amount of drug ingredient(s) as milligrams per total millilitres, followed by the concentration of drug ingredient(s) as milligrams per one millilitre. The standard's legibility section, which was adopted from the Man-Systems Integration Standard of the National Aeronautics and Space Administration (NASA 1995), defines typographical specifications for ensuring legibility of critical information. There is no legal requirement for pharmaceutical manufacturers to follow the CSA standard, but there is a legal requirement for them to follow the Canadian Food and Drug Regulations. In addition, although some of the requirements set out in both the CSA standard and the NASA standard are based on previous research, there are many aspects of the CSA standard that are based on expert opinion. The objectives of phase one of this study were to answer the following two questions: (1) to what extent do the inner labels on ampoules and vials of injectable drugs currently used in Canadian hospitals adhere to the CSA standard? and (2) to what extent do they adhere to the Canadian Food and Drug Regulations?
Method
A total of 78 samples (21 ampoules and 57 vials) were randomly collected from a pharmacy inventory in a large urban teaching hospital. This represented 18% of the 116 different ampoules and 22% of the 265 different vials carried by the hospital. The evaluation was conducted from May 2006 to July 2006. The first two thirds of the samples were collected from used, or expired, ampoules and vials returned to the pharmacy. The remaining third were randomly collected from all areas of inventory to ensure refrigerated items and narcotic products were included in the sample. The final sample is thought to be representative of the currently available ampoules and vials in a hospital formulary in Canada.
Typographical dimensions (i.e., the stroke width, character height, character width, etc.) were measured on the inner labels of the containers. A transparent plastic ruler marked in millimetres and a magnifying glass were used to make the measurements. The measurements are considered accurate to 0.5 mm.
Results
The clauses of the CSA standard are divided into three categories: clauses worded with shall are proposed as mandatory requirements, clauses worded with should are considered recommendations and clauses worded with may are taken as suggestions. There are 25 shall clauses, eight should clauses and two may clauses relevant to the labelling of ampoules and vials. For the purposes of this study, 23 shall clauses and six should clauses were considered.
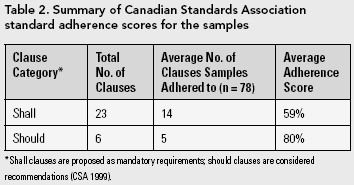
None of the samples adhered to all of the shall and should clauses of the CSA standard. Table 2 summarizes the average adherence score for shall and should clauses. The adherence score for a sample was calculated by determining the ratio of the number of adhered-to clauses to the total number of clauses.
[Table 3]
Table 3 lists the shall and should clauses and suggests findings and possible reasons for non-adherence for the CSA standard clauses that had a non-adherence rate of 50% or more.
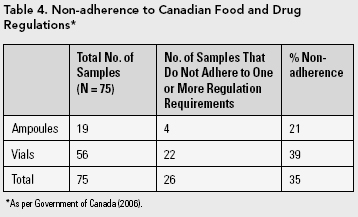
Three samples were determined to be special access drugs that are not available for sale in Canada and were excluded from the analysis for evaluating adherence to Canadian Food and Drug Regulations. All three drugs failed one or more requirements of the regulations. Table 4 lists the non-adherence rate for the remaining 75 samples.
A more detailed examination of non-adherence can be found in Appendix A ("Rates of Non-adherence to CSA Standards") and Appendix B ("Rates of Non-adherence to Government of Canada Food and Drug Regulations").
Phase Two: Failure Mode and Effects Analysis of the Label-Reading Process
To investigate potential failures, causes and effects of the label-reading process, a failure mode and effects analysis (FMEA) was conducted with a group of seven healthcare professionals with previous FMEA training. The results of this FMEA revealed the components of the label on injectable drugs considered important by the end-users for safe medication use. Failure modes (or errors) that are related to reading the brand name, common name, concentration, total amount of drug ingredient(s) and route of administration were rated as potentially severe modes of failure; therefore, these elements need to be carefully considered when designing labels. A full account of this FMEA has been reported elsewhere (Jeon et al. 2007).
Phase Three: Human Factors Experiment with One Type of Existing Label
Although Cohen (2007) argues against printing directly on ampoules because the lack of contrast between the print and the background renders the text illegible, this concern related to printing is not fully addressed in the CSA standard and is not addressed in the Canadian Food and Drug Regulations. We therefore designed an experiment to test the speed and accuracy of identifying information on ampoules with type printed directly on the glass container, or on a clear substrate that is adhered to the glass, and compared the results to those with the same label design printed with black ink on an opaque, white substrate adhered to a container.
Method
Participants
Twenty-four registered nurses (two males and 22 females) from an acute care hospital were recruited for the experiment. They ranged in age from 33 to 60 years (mean age 44) and had eight to 37 years of practice experience (mean 21.4 years). Participants were allowed to wear their glasses or contact lenses. All participants were tested for visual acuity and colour vision.
Stimuli
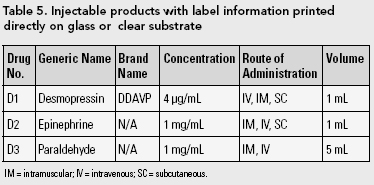
Three ampoules with type printed directly on the glass or a clear substrate (existing labels) that are currently available in Canada and identical ampoules with label information printed with black ink on an opaque, white substrate were presented to the participants (i.e., a total of six different labels). The details of the existing drugs used are summarized in Table 5. The labels designed for this experiment were identical to the existing labels except for the use of black lettering on a white paper substrate (Figure 1).
[Figure 1]
Procedure
For each of the six ampoules, participants were asked three different questions: (1) What is the concentration? (2) What is the generic name? and (3) What are the routes of administration? The rate of response for each was timed. The experiment was conducted in two rooms with similar lighting conditions. The sessions were video recorded with a camera positioned behind and diagonally from the participants such that their faces were not shown in the recordings. A set of six ampoules were placed upright in a single row on top of a flat table surface covered by a white foam cup until the participant was ready. The participant read a question displayed on a computer monitor and then picked up the ampoule to answer the question. Time to respond to the information being asked and accuracy of the response were recorded. Each 40-minute session consisted of six practice trials preceding 18 actual trials divided into three blocks of six trials.
Results
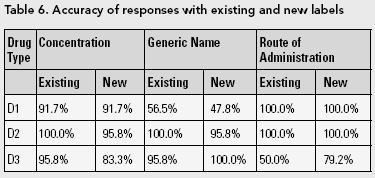
Since the participants were allotted as much time as they needed to identify the concentration, generic name and routes of administration of the drug, the accuracy rate for reading the existing labels and the new labels was similar. These results are presented in Table 6. The only statistically significant difference (p < .05) between the accuracy of responses for the existing and new labels was for the route of administration for D3.
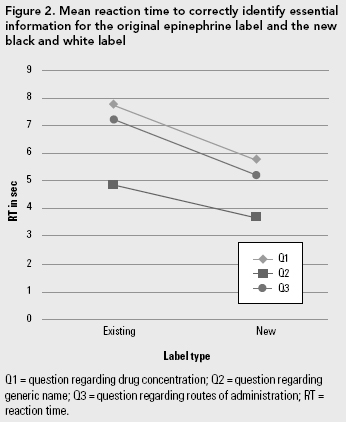
The amount of time that it took to identify the information on the existing labels that were printed directly on glass or a clear substrate versus the new labels printed with black ink on an opaque, white substrate was statistically significantly longer (p < .0001). For instance, the mean correct reaction time for each of the three questions asked for epinephrine (D2) is presented in Figure 2.
Discussion and Recommendations
Two approaches to examining the labelling of injectable drugs that have not been extensively employed and that have been reported in this paper are (1) routine examination of the adherence of drug labels to standards and regulations and (2) experimentation to support existing and future recommendations (although some experiments have been conducted by others, i.e., Filik et al. [2006], Gabriele [2006] and Wogalter and Vigilante [2003]).
In phase one of our study, 78 sample vials and ampoules collected from a hospital pharmacy inventory were evaluated against the current CSA (1999) recommendations that define minimum design requirements for labels on ampoules and vials. The vials and ampoules were also evaluated for adherence to the Canadian Food and Drug Regulation for labelling (Government of Canada 2006). Some of the statements in the CSA standard and in the Food and Drug Regulations are worded in a way that requires interpretation. For example, the Government of Canada (2006) Food and Drug Regulation C.01.004. (3) states, "Where the container of a drug is too small to accommodate an inner label that conforms to the requirements of these Regulations," but it is not clear what is considered too small to accommodate an inner label as required in the regulations. For the purposes of this study, a container capacity of five millilitres or less was considered to be "too small" as is the case in the CSA standard. An unclear statement in the CSA standard specifies the minimum space between characters for displaying critical information (clause 4.4.8). However, the word "space" is not clearly defined in the standard. For the purposes of this study, the space was interpreted as the space between two straight-sided characters such as H and L as defined in the NASA's Man-Systems Integration Standard (NASA 1995), from which the legibility section of the standard was derived. Other examples of wording that could be interpreted incorrectly can be found in Appendix C ("Ambiguities in the Canadian Food and Drug Regulations and in the CSA standard")
The adherence rate to the 23 mandatory requirements in the CSA standard was 59%. The average proportion of the inner labels for ampoules and vials that did not adhere to one or more of the requirements in the Canadian Food and Drug Regulations was 35%. It is important to note that although the percentage of drugs that did not meet one or more of the Canadian Food and Drug Regulation requirements was 35%, a large portion of the non-adherence resulted from not including both the English and French versions of the word sterile and stérile (24% of the total samples) and for not including the manufacturer address on the label (9.3% of the total samples). It is also noted that Health Canada does allow exceptions to the labelling information requirements through a policy for labelling of "special containers." The policy applies to containers that are too small to accommodate a full label and containers whose design causes their label to be destroyed during use. Also, at the time of this publication, there was no labelling guideline by Health Canada available to verify our interpretations of the regulations since Health Canada is in the process of developing a new labelling guideline. Therefore, the non-adherence rate found in this study might change if the new labelling guideline or the special container policy were to be taken into consideration. Of interest, Health Canada has recently initiated a Progressive Licensing Project which aims to improve the drug regulatory system and will include a review of current drug regulations and labelling requirements.
Of concern is that one of the samples did not display the common name properly and two of the samples did not display the route(s) of administration. In the case of an improperly displayed common name, it appears that there was preferential emphasis placed on the manufacturer's branding. There may be instances where explaining the rationale for specific recommendations in a document might improve adherence. For example, an explanation of why a mixed set of characters is preferable to all capital characters (lowercase characters have more variation in character design and thus the visual cues provided by a combination of capitals and lowercase characters renders type more legible than if it is set in all capital characters) conveys the importance of the choice of a mixed character set.
Phase two of the project was an FMEA conducted with seven healthcare professionals with previous experience with FMEA in order to identify the critical information needed on an ampoule or vial for safe medication use. Failure modes related to reading brand name, common name, concentration, total amount of drug ingredient(s) per total volume and route(s) of administration were rated with higher-than-average criticality in the FMEA.
Phase three involved a human factors experiment with a group of 24 nurses. This experiment demonstrated the superiority of black lettering on a white background over printing directly on ampoules (or on a clear substrate that is adhered to ampoules).
This research has focused on some of the concerns with the current labelling of ampoules and vials from a human factors perspective. Although the three-phased study reported here is limited in scope, there are several recommendations, based on the results, that can be made regarding the improvement of guidelines, standards and regulations related to drug labelling:
- When the CSA standard and the government regulations are under review, consider
- performing user testing regarding the interpretation of the guideline or regulations;
- including an explanation (evidence) of the rationale for particular recommendations or requirements;
- examining the failure modes (or errors) related to the brand name, common name, concentration, total amount of drug ingredient(s) and route of administration;
- evaluating the necessity of the information required in regulations, such as "address of manufacturer," which takes valuable space on the label.
- Study the feasibility of using larger-sized ampoules and vials for small volumes to increase surface area for label information.
- Prohibit the use of printing directly on glass or a clear substrate in the labelling of ampoules or vials containing medications.
[To view the Appendices, please download the PDF.]
About the Author(s)
Kathryn Momtahan, RN, PhD, is the Corporate Coordinator, Nursing Research, in the Nursing Professional Practice Department at the Ottawa Hospital, Ottawa, Ontario.
Catherine M. Burns, PhD, PEng, is the Director, Advanced Interface Design Lab, and Associate Professor, Systems Design Engineering, at the University of Waterloo, Waterloo, Ontario.
Jennifer Jeon, BASc , is a Masters Candidate, Systems Design Engineering, at the University of Waterloo, Waterloo, Ontario.
Sylvia Hyland, RPh, BScPhm, MHSc (Bioethics), is Vice-President, Institute for Safe Medication Practices Canada (ISMP Canada), Toronto, Ontario.
Sandra Gabriele, MDes, is an Assistant Professor with the Department of Design at York University, Toronto, Ontario.
Acknowledgment
The authors gratefully acknowledge the financial support of the Canadian Patient Safety Institute and the participation of the nurses in this study. Thanks to Sharon Ann Kearns for supporting this project.References
Ashcroft, D.M., P. Quinlan and A. Blenkinsopp. 2005. "Prospective Study of the Incidence, Nature and Causes of Dispensing Errors in Community Pharmacies." Pharmacoepidemiology and Drug Safety 14(5): 327-32.
Berman, A. 2004. "Reducing Medication Errors through Naming, Labeling, and Packaging." Journal of Medical Systems 28(1): 9-29.
Canadian Standards Association. 1999. Labelling of Drug Ampoules, Vials, and Prefilled Syringes (Vol. CAN/CSA-Z264.2-99). Etobicoke, ON: CSA.
Cohen, M.R. 1999. "The Role of Drug Packaging and Labeling in Medication Errors." In M.R. Cohen, ed., Medication Errors. Washington, DC: American Pharmaceutical Association.
Cohen, M.R. 2007. "The Role of Drug Packaging and Labeling in Medication Errors." In M.R. Cohen, ed., Medication Errors (2nd ed.). Washington, DC: American Pharmacists Association.
Filik, R. K. Purdy, A. Gale and D. Gerrett. 2006. "Labeling of Medicines and Patient Safety: Evaluating Methods of Reducing Drug Name Confusion." Human Factors: The Journal of the Human Factors and Ergonomics Society 48: 39-47.
Gabriele, S. 2006. "The Role of Typography in Differentiating Look-Alike/Sound-Alike Drug Names." Healthcare Quarterly 9: 88-95.
Government of Canada. 2006. Food and Drug Regulations, C.R.C., c. 870. Ottawa: Author.
Greenall, J. S. Hyland, M. Colquhoun and V. Jelincic. 2004. "Applying Engineering Principles to Medication Safety." Canadian Journal of Hospital Pharmacy 57(2): 110-13.
Health Canada. 2008. Progressive Licensing Project. Accessed March 3, 2008. http://www.hc-sc.gc.ca/dhp-mps/ homologation-licensing/index_e.html.
Institute of Medicine of the National Academies. 2007. Preventing Medication Errors. Washington, DC: The National Academies Press.
Jeon, J., S. Hyland, K. Momtahan and C.M. Burns. 2007. Challenges with Applying FMEA to the Process for Reading the Labels on the Containers for Injectable Drugs. Proceedings of the 51st Annual Meeting of the Human Factors and Ergonomics Society, Baltimore, MD.
Kenagy, J.W. and G.C. Stein. 2001. "Naming, Labeling, and Packaging of Pharmaceuticals." American Journal of Health Promotion 58(21): 2033-41.
National Aeronautics and Space Administration. 1995. Man-Systems Integration Standards (B ed., Vol. 1). Washington, DC: Author.
Orser, B.A., R.J. Chen and D.A. Yee. 2001. "Medication Errors in Anesthetic Practice: A Survey of 687 Practitioners." Canadian Journal of Anaesthesia 48(2): 139-46.
Orser, B.A. and D.C. Oxorn. 1994. "An Anaesthetic Drug Error: Minimizing the Risk." Canadian Journal of Anaesthesia 41(2): 120-4.
Phillips, J., S. Beam, A. Brinker, C. Holquist, P. Honig, L.Y. Lee and C. Pamer. 2001. "Retrospective Analysis of Mortalities Associated with Medication Errors." American Journal of Health-System Pharmacy 58(19): 1835-41.
United States Pharmacopoeia. 1994, November. "Simplifying Overcrowded Injection Labels." USP Quality Review 45.
United States Pharmacopoeia. 1998, May. "National Recommendations: Practice Safe Labeling." USP Quality Review. 62
United States Pharmacopoeia. 2000, September. "DPPR - A Final Glance." USP Quality Review 75.
Wogalter, M.S. and W.J. Vigilante Jr. 2003. "Effects of Label Format on Knowledge Acquisition and Perceived Readability by Younger and Older Adults." Ergonomics 46(4): 327-44.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Note: Please enter a display name. Your email address will not be publically displayed