
Healthcare Quarterly
Improving Patient Access to Medical Services: Preventing the Patient from Being Lost in Translation
Allison Bichel, Shannon Erfle, Valerie Wiebe, Dick Axelrod and John Conly
Abstract
The Medical Access to Service project was initiated to broadly engage participants in the health system to collectively improve service integration and patient access to primary care and specialist medical services. The Conference Model® (the Axelrod Group, Willmette, IL) was used as a change vehicle. The ideal design was translated into the creation of central access and triage (CAT) processes across medical specialties, development of prioritization tools and implementation of access and efficiency through Alberta AIM (access improvement measures) collaboratives for process re-engineering. The ultimate goal for all Albertans who need care is one point-of-access - one standardized process to ensure equal access for all regardless of where they live.
Introduction/Background
Improving access to health services is a priority across Canada. The data on Canada's performance with regard to access to primary and specialty care suggests a significant opportunity for improvement. For example, in 2004, Canada was identified as the country with the lowest percentage of citizens who could access a physician with a same-day appointment (27%), compared to the United States (33%), the United Kingdom (41%), Australia (54%) or New Zealand (60%) (College of Family Physicians of Canada 2006). With regard to access to specialty care, Canada ranked second lowest, with 57% of its citizens waiting at least four weeks to access specialty care, compared to the United States (60%), Australia (46%), the United Kingdom (40%), Germany (23%) and New Zealand (22%) (College of Family Physicians of Canada 2006). Nationally and internationally, there has been significant research on wait times. Postl reports, however, that "wait times are a symptom of a larger problem…Canadians need to support a transformation that puts patients at the centre of the system" (Postl 2006: 9). In the final report of the Federal Advisor on Wait Times, recommended actions to improve access included research to support benchmarking and operational improvements, adoption of modern management practices and innovation, accelerated implementation of information technology solutions and cultural change among health professions (Postl 2006). The challenge is navigating change across multiple healthcare service providers in diverse settings across the continuum of care. Change strategies that support access and integration include providing people-centred care, reducing clinical variance, organizing the care continuum and improving process management. These strategies became the major focus of the improvements implemented in Calgary.
The reality and practice of improving system-wide access is complex, as different programs and sectors use varying approaches toward the same objectives of improving access, quality and efficiency. For example, in the former Calgary Health Region (Alberta Health Services – Calgary and Area), the departments of medicine, family medicine and the primary care networks were trying to tackle access to services differently. The scope of services provided by these groups is significant and affects 1.3 million people. Approximately 30% of people needing outpatient services are seeking access to medical specialists. System complexities and the propensity for 250 medical specialists and approximately 700 primary care physicians to work in silos increases the risk of duplication and discontinuity, leaving the patient "Lost in translation." Organizing the care continuum through a patient-focused lens was a critical starting point to improving access.
The need to establish standardized processes based on best practice was evident. The referral process represents the critical interface across care providers and settings. Historically, primary care physicians worked alongside specialists in the hospital. Informal consultation was common, resulting in the development of individual collaborative relationships for patients to access specialist care. Despite unprecedented growth and further specialization, the referral process remained unchanged. Concerns with the referral process affect all services, providers and patients across the continuum of care, including: inconsistent referral criteria and clinical variance, diverse requirements for patient information, lack of communication regarding acceptance of the referral, and proliferation of intake points and subspecialty clinics with no corresponding service road map. System capacity was further reduced by the "shotgun" referral approach, no shows, and incomplete referrals resulting in multiple specialist appointments. The Medical Access to Service project was initiated with an overarching goal to work in a collaborative, integrated manner to improve medical access. Objectives included broadly engaging participants in the health system to collectively improve patient access to primary care and specialist medical services, and to improve service integration and communication between medical specialists, primary care physicians and their respective healthcare teams.
Methods and Change Process
Recognition of the Problem
The referral process is owned by everyone and no-one in particular. In large complex systems, seemingly small limitations in the referral process can be a major impediment to care, resulting in frustration, increased wait times, double booking, missed appointments and inefficiencies. Qualitative research and interviews with key stakeholders, through group discussions with rural and urban primary care physicians, illuminated the issue (Gramlich and Silvius 2006). As clarity emerged regarding the problems with the referral system, key leaders from the departments of medicine, family medicine, rural medicine, cardiac sciences and the primary care networks collaboratively sponsored a planning process to address improvements to the referral process.
Setting the Scope
The next step was to set the scope and identify where realistic change could be achieved. From a family physician's perspective, referral to internal medicine specialists represents only a subset of their patients' consultation needs. However, early in the project we included all internal medical specialties in the scope, including Cardiology, Endocrinology, General Internal Medicine, Gastroenterology, Geriatrics, Hematology and Hematologic Malignancies, Nephrology, Respirology and Rheumatology. Key leadership provided support to explore issues, identify an ideal design and implement recommendations.
The Conference Model® as a Change Vehicle
The Conference Model® (Axelrod 2002) was used as a change vehicle. This approach included the following parameters: clearly defining the purpose, utilizing workshop events to identify issues and solutions and creating an implementation plan. This whole system change approach is founded on four principles:
- Widening the circle of involvement to create a critical mass of people who design and support necessary changes;
- Connecting people to each other and to different perspectives, information and ideas creation and action;
- Creating communities for action to implement the change; and
- Embracing democracy so issues of self-interest versus the common good and minority versus majority opinion are balanced to ensure support (Axelrod 2002).
Two Referral and Access Conferences were hosted in October 2006 and January 2007. The first conference focused on issue identification, the second on ideal design. These non-traditional conferences involved two-day small- and large-group discussions with 200 attendees, including patients and family members, family physicians, specialists, secretaries, decision-makers and other healthcare professionals. Finally, for input and validation, the output from the conferences was discussed with people who had not been able to attend.
Engagement of several hundred stakeholders in redesigning referral and access at the outset raised some concerns with respect to time and financial commitment. Key leaders came together to achieve clarity on the purpose and to explore the risks and possibilities. Simulating the conferencing process was useful in strengthening the leadership team and guiding the overall engagement design. Inherent in this process was a perceived risk regarding whether or not a reasonable solution for successful implementation would be proposed. It was important to trust that people involved directly in the work were in the best position to provide creative solutions and support implementation. Finally, clarity from leadership around boundaries for eliciting change, and commitment to steward the work, were essential.
Interventions
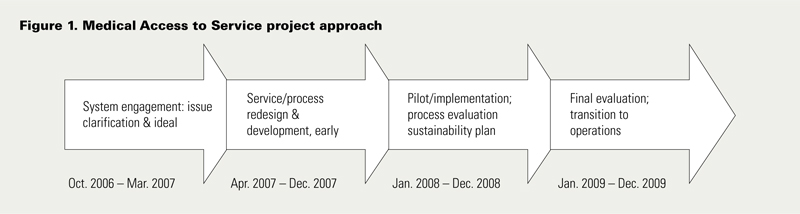
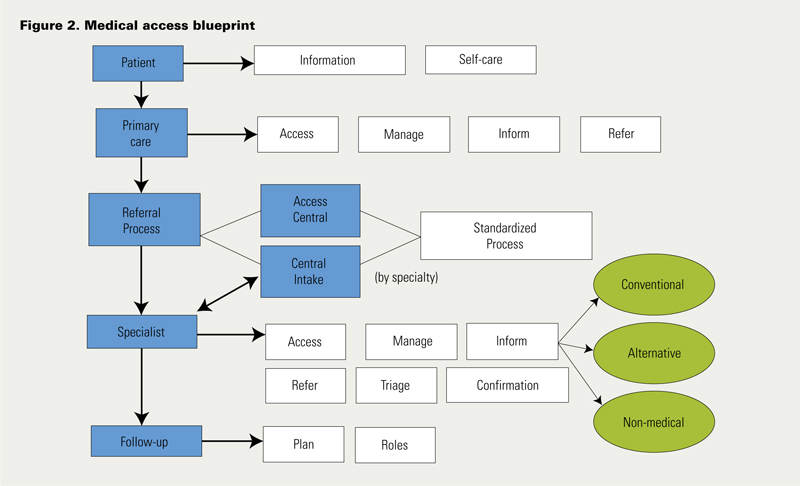
The Referral and Access Conferences were key events, and most importantly they were viewed as a part of an overall change plan (Figure 1). These conferences were assessed using a questionnaire with a standard Likert scale. Once the system had developed an ideal design (Figure 2), an implementation business case, a project structure and timeline were developed. This involved operationalizing critical design elements, identifying responsibility and accountability for implementation of the change, and identifying required resources, timelines, risks and communication plans. A steering committee and an operations committee were struck to provide oversight and guidance and to remove barriers to success. A project manager coordinated and provided leadership to working groups, facilitated delivery of the plan and acted as a liaison with stakeholders across the continuum. Working groups were established to deliver on parts of the plan. Three integrated projects were launched:
- Creation of central access and triage (CAT) systems across specialized medical services (Gastroenterology, Rheumatology, General Internal Medicine, Endocrinology, Hematology and Hematologic Malignancies, Cardiology, Geriatrics, Nephrology). Central access and triage involved pooling referrals by specialty; standardized information requirements (Figure 3) and policy for confirmation of receipt of referral, acceptance and appointment scheduling. Improvements to clinic access through implementation of CAT clinics were measured using wait time in weeks to appointment based on triage category and acceptance of referrals. Acceptance of referrals was measured to determine if using a standardized form improved referral quality, and as a proxy indicator for improved efficiency. Where appropriate, a t test was used to test for significance of continuous variables (wait times) and a p-value of < .05 was considered significant.
- Development of reliable, valid, clinically coherent prioritization tools for four specialties.
- Implementation of two Alberta AIM (access improvement measures) access and efficiency collaboratives in both specialty and primary care to redesign clinic process flow to reduce wait times before and during an appointment.

Results
Evaluation of the Referral and Access Conference
Evaluation of the second Referral and Access Conference (n = 89) indicated that 97% of participants either agreed or strongly agreed that the conference was a valuable way to begin the redesign of the referral process, and 92% either agreed or strongly agreed that the "ideal design" addressed their concerns with the current referral process. Quotes from participants regarding their conference experience are illustrated in Table 1.
| Table 1. Quotes from participants regarding their Referral and Access Conference experience |
| Evaluation results from second conference |
| "Overall, a worthwhile dialogue and starting point. This is a REAL issue and I'm happy to see it's being addressed." |
| "The most valuable part of the conference was networking, hearing different perspectives from different stakeholders, seeing a unified vision develop from different groups independently, developing a modified process and implementation plan." |
| "Thanks for considering ‘Patients’ to be in attendance. It was overall an eye-opener to see the problems but also to see the ingenuity and dedication to making a change. It was an overall awesome experience and I will do my part to make a difference." |
Involving patients and families in issue identification and ideal design was invaluable. Giving voice to their story and needs infused meaning and made the need for change compelling. It also helped to silence ego and self-interest. Broad stakeholder engagement also helped speed implementation. In particular, there was typically a credible peer, who had participated in the conferences, to whom different groups could be referred when they expressed concerns or resisted ideas reflected in the ideal design.
Central Access and Triage Clinic by Specialty
Preliminary evaluation of central access and triage has resulted in decreased wait times and timely access for patients requiring urgent care. The pooling of referrals has eliminated duplicate referrals, and wait times for each physician have equalized. By standardizing CAT through the use of a single, standardized referral form and consistent triage language (Emergency, Urgent, Semi-urgent and Routine referral types), referring healthcare providers reported increased ease and efficiency in sending referrals.
Rheumatology CAT was the initial pilot in 2006, with a reduction in wait times between 15% and 37% depending on urgency. With the success of Rheumatology, Gastroenterology CAT opened shortly afterwards, with a resultant 8% decrease in wait times despite a 153% increase in referrals. (An average 1,000 referrals were processed per month.) Patient wait is now based on patient urgency rather than physician name (previously, one patient could wait 38 times longer than another patient with the same urgency level).
From inception to December 2008 (Table 2), most clinics saw a significant increase in monthly referral volumes as follows: Endocrine 75%, Gastroenterology 50%, General Internal Medicine 26%. Rheumatology and Hematology saw no change in referral volume. Despite the increases in patient referrals, wait times (Table 3) improved for urgent assessments in Endocrinology from two weeks to one and in Gastroenterology from 52 to 12 weeks. Within Rheumatology, which piloted CAT prior to other divisions, data were available for wait times before implementation of CAT and following its implementation, and a significant reduction in wait times was observed for routine, moderate and urgent referrals compared to a 2005 practice audit (Barr et al. 2007). Wait times from 2005 for referrals classified as urgent, moderate and routine were compared with those from periods in 2006 and 2007. Wait times for consultation decreased from a mean (SD) of 29 (± 46) to 17 (± 14) days (p < .05) for urgent-level referrals, from 110 (± 57) to 63 (± 42) days (p < .00005) for moderate-level referrals, and from 155 (± 88) to 108 (± 37) days for routine-level referrals, respectively, between 2005 and 2008 (Barr et al. 2007). In addition, wait list shopping by referring physicians was documented to have ended. Although pre-implementation data were not available for all divisions, it may be expected that improvements in wait list times would have been comparable.

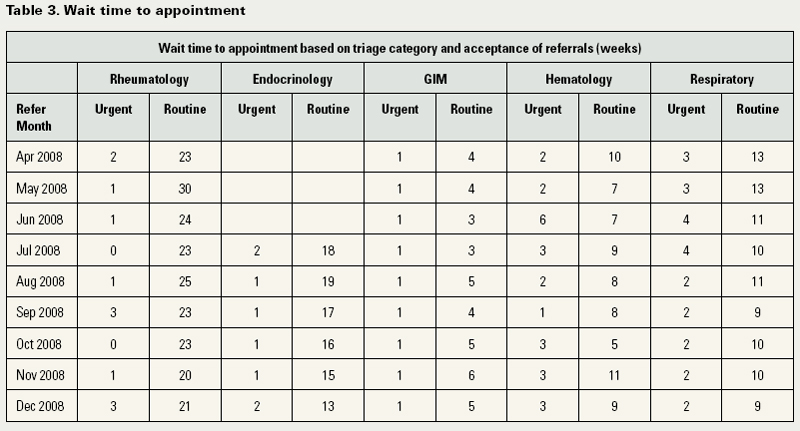
Acceptance of referrals is presented in Table 3. Referrals that were not accepted include referrals that were redirected, had incomplete information and were cancelled. In most cases, improvements were noted following implementation of central access clinics. Hematology went from 17% of referrals not accepted to 6% from April to November 2008, while Endocrinology improved from 19% of referrals not accepted to 9%, respectively, from July to November 2008.
Prioritization Tools
Western Canada Wait List (WCWL) prioritization tools have been developed for Rheumatology, Nephrology, Gastroenterology and Geriatric referrals. The tools are designed to provide a reliable and valid way of ranking the relative urgency for referrals and disposition of patients, with the intent of improving access to medical specialties. The tools will match the single-entry process via CAT for each of the specialties. Implementation and evaluation of the tools will occur through 2009. A testable version of the rheumatology tool is complete, and testing will commence in 2009. Beta versions of the other three tools are available.
Access Improvement Measures (AIM) Collaborative
Alberta AIM results are measured using cycle time and third-next-available appointment (Murray and Berwick 2003). Five of the 12 teams have been selected as a sample for evaluation and have participated in focus groups. The level of success achieved by these teams varies, although all of the teams reported they learned a useful perspective about the importance of measuring their daily activities. Nearly all found the regular involvement with a facilitator was useful but that the actual process was cumbersome. Clinics participating in both AIM and CAT saw synergistic results through their participation. Reported successes seen by specialty clinics as a result of participation in AIM for the Diabetes Hypertension and Cholesterol Centre included a reduction in wait times for all patients from 96 to four days, a reduction in wait times for urgent patients in Gastroenterology at Foothills Medical Centre from 60 to five weeks, and a reduction in the time to third-next-available appointment from 80 to 30 days in the division of General Internal Medicine at the Peter Lougheed Centre. The cycle time, the time a patient spends at the clinic, has been reduced by 30 minutes.
Discussion
An integrated approach using broad engagement at the start of this project was a prerequisite to achieving systemic change. This resulted in the development of an infrastructure that linked patients and families, primary care physicians, specialists and multi-disciplinary teams. Key strategies included workforce optimization, process re-engineering including the development and uptake of a single, standardized referral form, and improved communication between providers. The end result was improvement in access, integration and coordination of care.
Changes in referral volume reflected both an increase in the number of referrals to the specialty area and an adoption rate of CAT by referring physicians. In all areas, the adoption rate represents the number of referrals sent by referring healthcare providers to CAT. The maintenance of wait times for routine referrals and the decrease in wait times for urgent referrals suggests that despite an increase in referral volume, patients are being managed more efficiently. CAT positively impacts wait times for several reasons. Consistently applied triage criteria allow more patients to be appropriately redirected to alternative care providers or subspecialty clinics, including referrals to other sites such as the Colon Cancer Screening Centre, the Sleep Centre and the Cough Clinic.
Movement toward a single, standardized referral form, consistent triage language and consistent communication strategies allowed referring healthcare providers to follow explicit referral requirements. This improved communication between primary care and specialty care and increased the quality of the referral information. Improvements in ease and efficiency in the referral process enhanced patient care and safety. The decrease in referrals not accepted further reduced the time required by specialty clinics in both re-routing and information gathering on referrals. Similarly, the time spent in primary care offices to refer to alternate clinics was also minimized. At the same time, unnecessary patient visits in both primary and specialty care were reduced because the required information and test results were provided.
Clinics participating in AIM demonstrated varying results, the work is ongoing and final evaulation has commenced. Some limitations may be that facilitators and faculty were new to the process and in early stages of training. In some cases recruitment of adequate numbers of facilitators was problematic. Although the AIM approach targets wait times in primary care clinics, including specialty clinics in the collaboratives resulted in an indirect benefit of building relationships between specialty and primary care providers and enhancing understanding of each other's challenges. An area for further development is the need to reconcile the AIM philosophy that supply must equal demand, and the concept that triage slows patient flow, with practice in some specialty clinics. Given that some specialty clinics had doubled their number of referrals, the "supply equals demand" goal was considered difficult to achieve. Still, other components within AIM have been instrumental in decreasing wait times. Ensuring that healthcare professionals worked to full scope of practice, achieved through cross-training, resulted in increased capacity. The collaborative also reinforced the importance of team work and engaged a core group of people at all levels of the organization to ensure buy-in and commitment to the change process.
Conclusion
Outcomes achieved through these service innovations reflect change strategies that support integration. Involving patients and families, and cross-continuum multi-disciplinary healthcare team members, was integral to creating an ideal design that addressed diverse requirements. Changes implemented have lessons for all specialty services, and there is the potential for broadly spreading the central access and triage model. Enhanced awareness and communication between providers along the care continuum as a result of CAT and prioritization tools facilitated organization and collaboration along the continuum. Additionally, central access and standardized referral and triage criteria reduced clinical variance. Improving access through process improvement using the AIM methodology increased system capacity. There is ongoing opportunity for continued improvement in the models with which we have had success to date. Adoption of CAT by all clinics within a discipline across all sites in Calgary will be an important first step to delivery of a truly centralized access model that will ensure all patients have access to the first available specialist across the system. Furthermore, as healthcare in Alberta expands to a provincial model, it will be important to spread the work of centralized access provincially. The ultimate goal for all Albertans who need care is one referral form, one point-of-access, and a standardized process to ensure equal access for all, regardless of the locale within the province.
About the Author(s)
Allison Bichel, MPH, MBA, is a Senior Consultant with EverSpring Consulting Inc. Allison has extensive health service design, facilitation and project management experience. She is currently focusing her research on organizational change.
Shannon Erfle, RD, BSc, MBA, is the Project Manager of Medical Access to Service, Alberta Health Services. Shannon has experience in program design and project management. She is currently working with Alberta Health Services to improve and enhance patient access to medical services.
Valerie Wiebe, RN, BN, MN, is Executive Director, Medical Services, Alberta Health Services - Calgary and Area. Valerie has experience in healthcare leadership across the continuum, including in-patient and outpatient acute care systems, primary care networks, public health and long-term care. Valerie says that "the Medical Access Project has provided a process for collaboration and integration system-wide. Congratulations and thank you to the teams involved in this project as they demonstrate the expertise, commitment and dedication required to achieve improvement in quality access and patient outcomes."
Dick Axelrod, MBA, is Co-founder of The Axelrod Group Inc., Chicago, IL. Dick authored Terms of Engagement - Changing the Way We Change Organizations and helped pioneer the use of large group methods to change organizations. He is currently focusing on high-engagement organizational change in education and healthcare.
John Conly, MD, FRCPC, FACP, is Professor of Medicine, Pathology & Laboratory Medicine and Microbiology & Infectious Diseases; Head, Department of Medicine, University of Calgary; and Clinical Head, Department of Medicine, Calgary Health Region. Dr Conly has been the Head of the Department of Medicine in Calgary since 2002 and established one of the largest Academic Alternate Relationship Plans in the country to date. He has overseen several new innovative programs that have enhanced patient care delivery.
Acknowledgment
We would like to acknowledge the support of the Medical Access to Service Steering Committee, the Medical Access to Service Operations Committee, the Executive Sponsors Carol Gray, Vice President Northeast Portfolio, Brenda Huband, Vice-President Continuing Care, Medical Services and Seniors' Health and Sid Viner, Executive Medical Director, Northeast Portfolio, Calgary Health Region and the funding provided by Alberta Health and Wellness (Wait Times Management Steering Committee and Academic Alternate Relationship Plan). We are indebted to the work done by all the members of the Departments of Medicine, Family Medicine, Rural Medicine, Cardiac Sciences, the Clinic Managers in Medical Services within the Calgary Health Region including the central access and triage teams, and the Alberta AIM Initiative.References
Axelrod, R. 2002. Terms of Engagement. Changing the Way We Change Organizations. San Francisco, CA: Berrett-Koehler.
Barr, S., T. Lupton and L. Martin. 2007. "Central Referral & Triage for Rheumatology (CReATe Rheum) in Calgary: Year 1 Update" [Abstract 4971]. In: Canadian Rheumatology Association Conference and Annual Meeting. p.91. Retrieved August 4, 2009 <http://www.rheum.ca/Resources/CRA-Abstract-Book-2007.pdf>.
College of Physicians and Surgeons of Alberta. 2003. Referral/Consultation Process. Edmonton, AB: Author. Retrieved January 24, 2008. <http://www.cpsa.ab.ca/publicationsresources/attachments_policies/The%20Referral%20Consultation%20Process.pdf>.
College of Family Physicians of Canada. 2006. When the Clock Starts Ticking: Wait Times in Primary Care. Discussion Paper.
Gramlich, C. and J. Silvius. 2006, January 25. Fact Finding: Increasing Access to Medical Specialists. Calgary Health Region. Department of Medicine. Internal Report
Murray, M. and D. Berwick. 2003. "Reducing Waiting and Delays in Primary Care." JAMA 289: 1035-40.
Postl, B. 2006. Final Report of the Federal Advisor on Wait Times. Ottawa: Health Canada. Retrieved November 28, 2008 <http://www.hc-sc.gc.ca/hcs-sss/alt_formats/hpb-dgps/pdf/pubs/2006-wait-attente/index-eng.pdf>.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Note: Please enter a display name. Your email address will not be publically displayed