
Healthcare Policy
Is It Worthwhile to Invest in Home Care?
Josée G. Lavoie, Evelyn L. Forget, Matt Dahl, Patricia J. Martens and John D. O'Neil
Abstract
The objective of this study was to estimate the impact of the First Nations and Inuit Home and Community Care Program (FNIHCCP) on the rates of hospitalization for ambulatory care sensitive conditions (ACSCs) in the province of Manitoba. A population-based time trend analysis was conducted using the de-identified administrative data housed at the Manitoba Centre for Health Policy, including data from 1984/85 to 2004/05. Findings show a significant decline in the rates of hospitalization (all conditions) following the introduction of the FNIHCCP in communities served by health offices (p<0.0001), health centres (p<0.0001) and nursing stations (p=0.0022). Communities served by health offices or health centres also experienced a significant reduction in rates of hospitalization for chronic conditions (p<0.0001).
The results of this study suggest that investment in home care resulted in a significant decline in rates of avoidable hospitalization, especially in communities that otherwise had limited access to primary healthcare.
Many studies have documented that First Nations experience a disproportionate burden of chronic diseases (CIHI 2004; First Nations Regional Health Survey National Committee 2005; Dyck 2001). The upward trend reported among the Canadian population (Canadian Healthcare Association 2009) is also evident, and will result in increased rates of hospitalization.
Recognizing this and following trends in all Canadian provinces, the First Nations and Inuit Health Branch (FNIHB) of Health Canada launched the First Nations and Inuit Home and Community Care Program (FNIHCCP) in 1999, its single most comprehensive new program to date. Investments totalled $152 million in the first three years of implementation, with an ongoing commitment of $90 million (Consilium Consulting Group 2006).
The objective of this study was to assess the impact, if any, of the FNIHCCP on the rates of hospitalization for ambulatory care sensitive conditions (ACSCs) in the province of Manitoba, Canada. The study is timely. While there seems to be broad consensus that home care services should become the next essential service to be covered under the Canada Health Act (Canadian Healthcare Association 2009; Kirby 2002; Romanow 2002; Tsasis 2009), we have been unable to locate solid evidence that investments in home care might result in a reduction in avoidable hospitalizations and savings associated with such a reduction.
This study is part of a larger study that investigated the relationship between models of community control, on-reserve access to primary healthcare services and health outcomes among First Nations people living in the province of Manitoba (Lavoie et al. 2010). Manitoba was selected for this study because, along with Saskatchewan, Manitoba is home to the highest proportion of First Nations people in Canada, at nearly 10% of the provincial population (Statistics Canada 2008). Second, Manitoba is unique in Canada and among other countries in that collaborations exist between the Assembly of Manitoba Chiefs, which represents First Nations, and the Manitoba Centre for Health Policy of the University of Manitoba, which houses the Population Health Research Data Repository ("the Repository"), consisting of provincial administrative databases that are longitudinal, de-identified yet linkable at the individual level. The Repository facilitates health research in areas that are of relevance to First Nations. Finally, this study was identified as a high-priority research area by the Assembly of Manitoba Chiefs.
Conceptual Framework
In this study, we are concerned with health needs that can be addressed through community-based primary healthcare intervention, including home care interventions. In this paper, we locate home care interventions within the primary healthcare continuum (Table 1). Home care includes secondary and tertiary prevention activities, as well as a spectrum of primary care interventions delivered in the home for the purpose of protecting and maintaining the autonomy of those living with chronic conditions.
| Table 1. Healthcare framework | |||
| Category & subcategory | Definition | Example | |
| Primary healthcare | Primary care | Outpatient treatment traditionally provided by general practitioners and, more recently, by nurse practitioners | Prescription, wound dressing |
| Tertiary prevention | Activities designed to assist in the management of complications once they manifest, to ensure that optimal autonomy is retained | Physical rehabilitation support after an amputation | |
| Secondary prevention | Activities focused on assisting in the management of chronic illness to avoid or delay the development of complications | Blood sugar monitoring and foot care | |
| Primary prevention | Early interventions designed to prevent the onset of chronic conditions | Education | |
| Source: Adapted by Lavoie from Starfield 1996. | |||
Although the exact role that primary healthcare can play in addressing health inequalities is limited (Marmot and Wilkinson 1999), reviews by Starfield and colleagues (2005) and Macinko and colleagues (2003) suggest that better access to primary care and primary prevention (these are the terms used by these authors, which when taken together roughly equate to primary healthcare) is associated with improved access to immunization; smoking cessation; better prenatal outcomes; decreased childhood morbidity; earlier detection of melanoma and breast, colon and cervical cancers; improved outcomes for patients with type 2 diabetes mellitus, hypertension and depression; improved management of asthma; and decreased all-cause mortality. As well, research at MCHP has shown that continuity of physician care is related to improved uptake of mammography and cervical cancer screening, higher rates of childhood immunization and lower rates of lower-limb amputations for people with diabetes (Martens and Fransoo 2008).
For the purpose of this study, we have defined outcomes in terms of hospitalization for ambulatory care sensitive conditions. These conditions are defined as "[t]hose diagnoses for which timely and effective outpatient [primary] care can help to reduce the risks of hospitalization by either preventing the onset of an illness or conditions, controlling an acute episodic illness or conditions, or managing a chronic disease or condition" (Billings et al. 1993).
Hospitalizations for ACSC diagnoses may therefore indicate a potentially preventable complication resulting from limited access to responsive primary healthcare services. Further, a disproportionate rate of hospitalization for ACSCs among First Nations people, when compared to other Manitobans, suggests possible inequity in access to primary healthcare (Martens et al. 2005) and the need for investment. This indicator has been endorsed by researchers and policy makers as a dependable indicator of the performance of primary healthcare services (CIHI 2006, 2007; Marshall et al. 2004).
Local access to care
In the First Nations context, on-reserve primary healthcare services are funded and were historically delivered by the First Nations and Inuit Health Branch of Health Canada. Broadly speaking, the current complement of on-reserve health services is based on a 1969 study (Booz Allen and Hamilton Canada 1969) that recommended a greater focus on prevention, among other factors. However, this study's recommendations were nested in a federal policy that saw the responsibility of the federal government as complementary to the services that were available from provincial governments. What emerged is a four-level framework that constitutes the basis of FNIHB funding for on-reserve health services, based on community size, level of remoteness and access to provincial services (Table 2). This categorization is generally termed facility designation.
Communities considered to have reasonable access to provincial healthcare services in nearby communities are funded to offer screening and preventive services (health offices). Communities located within a two-hour drive from provincial services are funded to ensure local access to preventive, screening and emergency care. These services, delivered through health centres, focus on primary prevention, with some level of secondary prevention interventions. There is no or limited funding to ensure off-hours coverage. More isolated communities served by nursing stations are funded to ensure local access to screening, prevention, emergency and treatment services on a 24/7 basis, delivered by nurses with an extended scope of practice.
Previous work by Martens and colleagues (2005) documented that diabetes prevalence is 4.2 times higher for Manitoba First Nations people compared to all other Manitobans (18.9% versus 4.54%), but the population rate of amputation due to diabetes is 16 times higher (3.1 versus 0.19 per thousand, ages 20 through 79). The study reported the highest rate of amputations (6.2 per thousand) in communities located in the southwest of the province. Although there is some variation, these communities are considered non-isolated (meaning that a general practitioner, a hospital or both are available within 60 kilometres, and that roads are passable all year) and are served by either a health office (N=5) or a health centre (N=4). These findings suggest that geographical accessibility does not guarantee that services can be accessed, are accessed or are responsive. These findings provide an impetus to look more carefully at the relationship between local access to care and outcomes.
In 1999, FNIHB rolled out the First Nations and Inuit Home and Community Care Program (FNIHCCP) in response to a national shift towards home care implemented in all provinces, which resulted in hospitals adopting early discharge of patients. This program was the most significant financial and program investment made by FNIHB in First Nations communities, and resulted in the expansion of secondary prevention activities for those living with chronic conditions (Health Canada FNIHB 2004c). It was made accessible to all First Nations communities as of 1999, with the exception of those communities receiving care from regional health authorities (i.e., no facilities in the community), under a 1964 agreement on jurisdictional issues between levels of health governance (FNIHB and Manitoba Health). Those communities can, at least theoretically, access home care from their RHA.
Home care services on reserves
The planning and development of the FNIHCCP was supported by a high-level advisory committee composed of federal, First Nations and Inuit partners. Unlike other programs rolled out in the past, the FNIHCCP was rolled out in a highly structured manner, with communities expected to complete a multistage program planning process, including completion of a community needs assessment, followed by the development of a service delivery plan, a training plan and a capital plan. As defined by FNIHB, key features of the program included on-reserve structured client needs assessments, managed care, access to home care nursing, access to in-home respite care and linkages with existing on- and off-reserve health and social services (Consilium Consulting Group 2006). These interventions can be defined as primary care (delivered by nurses where there are nursing stations), and secondary and tertiary prevention. As of September 2003, 96% of eligible communities were being funded by the program (Health Canada FNIHB 2004b), including all Manitoba First Nations communities, with the exception of those served by RHAs.
Methods
Data and sample
The sample for this research project includes all Manitoba residents eligible under the Manitoba Health Services Insurance Plan living on First Nations reserves (N=64,929 in 1984/85; N=71,510 in 2004/05). One conceptual impediment to pursuing this work to date has been that researchers have focused on ethnicity rather than residency in a community as the key independent variable. The current databases are unable to show First Nations identification reliably. This study, however, does not require First Nations identification because it is concerned with services accessible to community members, and theorizes that service availability is constrained by federal–provincial jurisdictional division of responsibilities over First Nations primary healthcare services, the level of on-reserve primary healthcare services funded and geography (Canada First Nations and Inuit Regional Health Survey National Steering Committee 2005).
We used six-digit postal code data in the administrative database to track all Manitobans to their home address to identify the population served by each community. Manitoba-registered First Nations represent 95.6% of the overall on-reserve population (Community Workload Increase System 2003/04 figures from FNIHB, Lavoie and Forget 2005). Others are non-status, Métis or non-Indigenous individuals who depend on the same services. In this study, only four communities (Dakota Plains, Dauphin River, Lake St. Martin and Long Plains, with a total population of approximately 2,000 individuals) could not be uniquely identified by postal code and thus could not be included in the sample. Table 3 provides a breakdown of communities per category. We estimate the impact of this omission to be negligible.
| Table 3. Description of the sample | ||||
| Number of communities | Total population included | |||
| 1984–85 | 2004–05 | 1984–85 | 2004–05 | |
| Level of primary healthcare available on reserve | ||||
| No facility | 2 | 2 | 2,627 | 1,031 |
| Health office | 24 | 24 | 22,631 | 19,225 |
| Health centre | 11 | 11 | 18,542 | 22,933 |
| Nursing station | 22 | 22 | 21,129 | 28,321 |
| 59 | 59 | 64,929 | 71,510 | |
Trends and patterns of health services used by residents living on First Nations reserves were identified from fiscal years 1984/85 to 2004/05 to assess the potential impact of community control and access to local primary healthcare services over time. The data used for this study included files held at the Repository housed at the Manitoba Centre for Health Policy, namely: (1) Vital Statistics files, (2) the Population Health Registry file for the provincial insured population and (3) the hospital record files. The Population Health Registry file provides demographic information such as sex, age and place of residence (a six-digit postal code), but is de-identified (i.e., no name, no complete address). A (new) family number is assigned when a resident becomes 18 years of age, is married or divorced. One of the divorced spouses, typically the woman, receives a new number. Tracking family numbers provides information on family composition. This population-based registry provides information on all residents in a given postal code, as well as their arrival and departures (births, deaths and moves) for any date since 1970 (Roos and Nicol 1999). Time-sensitive data (place of residence, family composition) are updated every six months. Longitudinal or linked data are typically put together as needed for each study. Each substantive file can be checked against the registry for accuracy of the identifiers and particular information, for example, date of in-hospital death (Roos et al. 2003).
Standardized data, based on every hospital contact, are submitted to Manitoba Health, the provincial agency responsible for funding. This information (including de-identified patient identifiers, physician claims, diagnoses, costs, hospitalization and institutionalization data) is part of a system maintained and controlled by Manitoba Health, and is accessible in a de-identified form via the Repository. This system allows tracking resource utilization over time for any given patient or particular medical diagnosis, including all hospitalization data.
Measures
Dependent Variable
The key dependent variable is hospitalization for an ACSC. For this study, we developed our own definition of ACSC. We began with a definition created by the Canadian Institute Health Information (2006, 2007), which is focused on an aging population. We added components from the Victorian Government of Australia, whose definition is more comprehensive (Victorian Government Department of Human Resources Division 2001). Finally, we fine-tuned our definition using recent studies related to the epidemiological profile of First Nations people in Manitoba and in Canada (Martens et al. 2002, 2005; Shah et al. 2003). Our final definition includes three categories of ACSCs: chronic, vaccine-preventable and acute conditions, as listed in Table 4. Each condition was defined based on the International Classification of Diseases. The 1984/85 to 2003/04 hospital data use the ICD-9-CM codes; the 2004/05 data use the ICD-10-CA codes. We used three-, four- and five-digit codes, depending on the condition.
| Table 4. Definition of ambulatory care sensitive conditions | |
| Conditions | Codes |
| Chronic conditions | Acute Bronchitis (only when a secondary diagnosis* of COPD is present); Asthma; Angina; Chronic Obstructive Pulmonary Disease (COPD); Diabetes, Diabetes with Complications; Grand Mal Status and other epileptic convulsions; Heart Failure and Pulmonary Edema; Hypertension (excluding cases with the following surgical procedures**); Iron Deficiency Anaemia, Other Deficiency Anaemia; Pneumonia (only when a secondary diagnosis* of COPD is present) |
| Vaccine-preventable conditions | Diphtheria; Haemophilus Influenza type B; Hepatitis A; Hepatitis B; Influenza; Measles; Meningococcal Disease (meningitis); Mumps; Pertussis; Pneumococcal Disease; Poliomyelitis; Rubella; Tetanus; Tuberculosis |
| Acute conditions | Cellulitis (excluding cases with the following surgical procedures except incision of skin and subcutaneous tissue where it is the only listed cause); Dental Conditions; Gastroenteritis; Pelvic Inflammatory Disease (excluding males or cases with a hysterectomy procedure); Severe ENT (Ear, Nose, Throat) Infections (excluding otitis media cases with a myringotomy procedure) |
| * "Secondary diagnosis" refers to a diagnosis other than most responsible. | |
| ** Code may be recorded in any position. Procedures coded as cancelled, previous and "abandoned after onset" were excluded. | |
| Source: CIHI 2006, 2007; Victorian Government Department of Human Resources Division, 2001. | |
Independent Variables
Two key independent variables were identified. The first focuses on the introduction of the FNIHCCP in 1999. The second is related to local access to primary healthcare. For this variable, we developed a database of First Nations communities in Manitoba that shows the level of care classifications outlined in Table 2. Accordingly, only 22 First Nations communities in Manitoba are resourced to offer a full complement of primary healthcare services (nursing stations). The remaining 35 are resourced for public health programs five days a week or less, that focus largely on primary prevention (education) and screening. In these communities, services to those individuals who have already been diagnosed with a chronic condition are extremely limited. Our sample includes an additional two communities that have no local access to services.
Statistical method
A model-based approach using the generalized estimating equations (GEE) method of parameter estimation was applied to these data to test for differences in hospital utilization rates for ACSCs. Generalized estimating equations are used as a method for analyzing correlated longitudinal data. These data have measurements (hospitalizations) taken over time (1984/85–2004/05) on subjects that share common characteristics (age group, gender and community). Therefore, one may expect the outcomes for subjects of similar age, gender and community to be correlated over time. The GEE method takes into account the correlated structure of the data and permits valid hypothesis-testing results.
Results
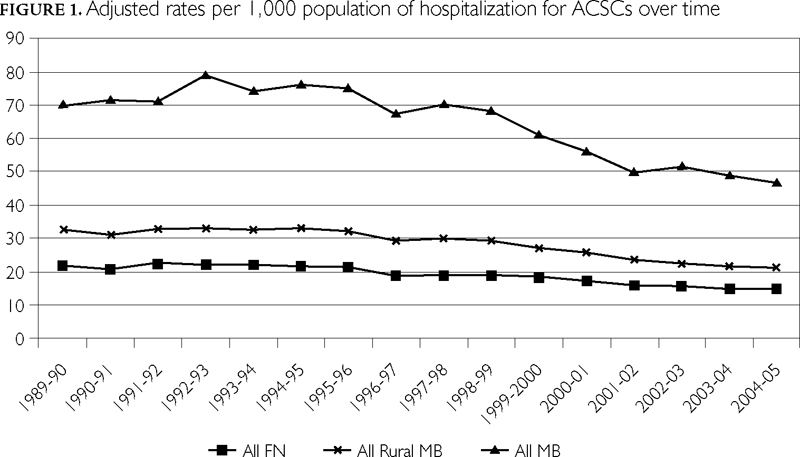
As shown in Figure 1, the rates of hospitalization for ACSCs have been declining over the past two decades in Manitoba, rural Manitoba and for individuals living on Manitoba First Nations reserves. To assess the potential impact of the FNIHCCP, we aggregated three years' worth of data for three separate time periods: 1989/92 was used as an overall baseline, the 1996/99 period was used as a FNIHCCP-specific baseline and 2002/05 was used as the post-intervention comparison.
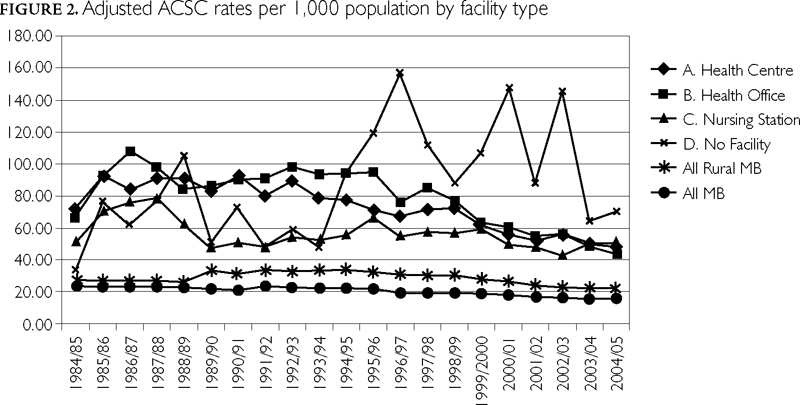
As shown in Table 5 and Figure 2, the rates of hospitalization for ACSCs steadily declined between 1989/92 and 2002/05 in all Manitoba communities and in Manitoba rural communities (First Nations communities excluded). In First Nations communities served by no facility, however, the rates of hospitalizations for ACSCs (all conditions) actually increased (p<0.0001) between 1989/92 in communities where individuals requiring care presumably accessed care outside the reserve in provincial facilities. There was no statistically significant difference for the 1996/99 to 2002/05 period for all conditions, although a significant decline in the rates for chronic conditions was noted (p=0.0409). Thus, the gains achieved in other Manitoba communities were not reflected in First Nations communities with no local access to care.
| Table 5. Relationship between the level of local access to primary healthcare (facility designation) and rates of hospitalization for ACSCs before and after introduction of the FNIHCCP | |||||||
| Avg. diff. in rates | ACSC | Time period | Mean estimate | Mean confidence limits | Chi-square | Pr > ChiSq | |
| No facility | All conditions | 1989/92 and 1996/99 | 0.4699 | 0.3281 | 0.6728 | 17 | <0.0001 |
| 1996/99 and 2002/05 | 1.3436 | 0.894 | 2.0194 | 2.02 | 0.1553 | ||
| Chronic conditions only | 1989/92 and 1996/99 | 0.5425 | 0.2760 | 1.0666 | 3.14 | 0.0762 | |
| 1996/99 and 2002/05 | 2.0025 | 1.0292 | 3.8961 | 4.18 | 0.0409 | ||
| Health office | All conditions | 1989/92 and 1996/99 | 1.1232 | 1.0202 | 1.2365 | 5.61 | 0.0179 |
| 1996/99 and 2002/05 | 1.6027 | 1.4531 | 1.7678 | 88.93 | <0.0001 | ||
| Chronic conditions only | 1989/92 and 1996/99 | 0.9879 | 0.8620 | 1.1322 | 0.03 | 0.8610 | |
| 1996/99 and 2002/05 | 1.5811 | 1.3610 | 1.8367 | 35.90 | <0.0001 | ||
| Health centre | All conditions | 1989/92 and 1996/99 | 1.2058 | 1.0844 | 1.3408 | 11.95 | 0.0005 |
| 1996/99 and 2002/05 | 1.3621 | 1.2205 | 1.5202 | 30.45 | <0.0001 | ||
| Chronic conditions only | 1989/92 and 1996/99 | 1.1600 | 0.9846 | 1.3666 | 3.15 | 0.0760 | |
| 1996/99 and 2002/05 | 1.3757 | 1.1781 | 1.6098 | 16.28 | <0.0001 | ||
| Nursing station | All conditions | 1989/92 and 1996/99 | 0.8789 | 0.7862 | 0.9825 | 5.15 | 0.0232 |
| 1996/99 and 2002/05 | 1.1744 | 1.0593 | 1.302 | 9.33 | 0.0022 | ||
| Chronic conditions only | 1989/92 and 1996/99 | 0.9275 | 0.7637 | 1.1265 | 0.58 | 0.4480 | |
| 1996/99 and 2002/05 | 1.1477 | 0.9526 | 1.3827 | 2.10 | 0.1473 | ||
| All Manitoba rural communities | All conditions | 1989/92 and 1996/99 | 1.0862 | 1.0246 | 1.1514 | 7.71 | 0.0055 |
| 1996/99 and 2002/05 | 1.3561 | 1.292 | 1.4233 | 152.11 | <0.0001 | ||
| Chronic conditions only | 1989/92 and 1996/99 | 1.1211 | 1.0395 | 1.2090 | 8.80 | 0.0030 | |
| 1996/99 and 2002/05 | 1.3634 | 1.2673 | 1.4668 | 69.06 | <0.0001 | ||
| All Manitoba | All conditions | 1989/92 and 1996/99 | 1.1333 | 1.0701 | 1.2001 | 18.31 | <0.0001 |
| 1996/99 and 2002/05 | 1.2537 | 1.2026 | 1.3069 | 113.5 | <0.0001 | ||
| Chronic conditions only | 1989/92 and 1996/99 | 1.2310 | 1.1423 | 1.3265 | 29.70 | <0.0001 | |
| 1996/99 and 2002/05 | 1.2287 | 1.1552 | 1.3068 | 42.89 | <0.0001 | ||
Communities served by a health office showed a decline in the rates of hospitalizations for ACSCs (all conditions, p=0.0179) between 1989/92 and 1996/99. This was not the case for chronic conditions. Following the introduction of the FNIHCCP, rates of hospitalizations for ACSCs fell, for all conditions and chronic conditions (p<0.0001). A similar pattern also took place in communities served by health centres. In communities served by nursing stations, the rates of hospitalization for all conditions were on the increase between 1989/92 and 1996/99 (all conditions, p=0.0232). Following the introduction of the FNIHCCP, the rates of hospitalization for all conditions dropped (p<0.001). Results for chronic conditions were not statistically significant.
Discussion
This study sought to document the relationship between local access to primary healthcare and the rates of hospitalization for ACSCs among First Nations people living on reserves in the province of Manitoba, Canada. We acknowledge a number of limitations to this study.
First, we used locality (postal codes) as opposed to ethnicity to identify First Nations. As a result, it is likely that some non-Indigenous individuals living on reserves (employees, partners), and some First Nations and non-Indigenous individuals living close to the reserve, were included in the sample. Because this study is focused on the impact of local access to care, we see this broader inclusion as acceptable. Many of these communities are remote and relatively isolated. Further, it is generally the case that First Nations people living close to a reserve will seek care on the reserve. Because access to care is constrained by geography, it is reasonable to assume that barriers to accessing care are shared by those who live near the reserve.
A second limitation is related to the size of our sample and the size of the communities, which prevented us from undertaking condition-specific analyses. Such analyses would have allowed us to look for condition-specific response time, as well as condition-specific service gaps. We are currently pursuing discussions in order to replicate this study in other provinces. While replication may provide opportunities to increase the sample size, it will also create challenges related to data comparability.
A third limitation is that, following Caminal and colleagues (2004), we chose to develop our own definition of ACSC, to match the epidemiological profile of First Nations. This choice will limit the comparability of our results to other studies. While this is a limitation, our purpose was to document the impact of a policy option on health outcomes, to complement other studies that compared the prevalence of health conditions and the disproportionate rates of avoidable hospitalization among Manitoba First Nations compared to the Canadian and Manitoba populations (Martens et al. 2002, 2005, 2007).
The final major limitation is the fact that this study is observational, and thus our results show association, not causation, which cannot be assumed. Further, we cannot disentangle the impact of the FNIHCCP from that of other interventions. That being said, the data used for this study include all people living in First Nations communities. Further, this comparative time trend analysis, with rural Manitoba being a comparison group, demonstrates that the decline in ACSCs experienced in other communities did not occur until the FNIHCCP was introduced. Still, we acknowledge that communities are diverse, and that other factors may have influenced our results.
Conclusion
This study documented that in the years prior to the implementation of the First Nations and Inuit Home and Community Care Program, communities served by health offices and health centres had limited access to primary healthcare. The introduction of the FNIHCCP expanded primary healthcare activities in those communities. It appears that these activities had a positive impact on rates of hospitalization for ACSCs. This is true for all ACSC conditions and for chronic conditions.
Communities served by nursing stations showed decreases in rates of hospitalization for ACSCs for all conditions. The same gains were not documented for chronic conditions, however. This finding is somewhat puzzling, and may be explained by the fact that communities served by nursing stations have local access to a broad complement of primary healthcare services. We postulate that the FNIHCCP did not have the same impact on chronic conditions as it did in other communities, because access to key services was already available. The program did, however, have an impact on rates of hospitalization for all conditions, suggesting that expanding human resources in primary healthcare was needed.
Finally, this study documented that in First Nations communities where access to the FNIHCCP was not available, the gains reported above were not experienced. Although more work is required to explain these results, they suggest that the FNIHCCP may have had an important impact.
This study is a first attempt at quantifying health outcomes evidence in relationship to the FNIHCCP. Our results show that this investment resulted in improved outcomes, and in a shift to utilization of home care services rather than hospital care. At the national level, our findings suggest that investments in home care services result in improved efficiency in the healthcare system, thereby bringing evidence to current interests in expanding services insurable under the 1984 Canada Health Act to include home care services.
Vaut-il la peine d'investir dans les soins à domicile?
Résumé
Cette étude visait à estimer l'impact du Programme de soins à domicile et en milieu communautaire des Premières nations et des Inuits (PSDMCPNI) sur les taux d'hospitalisations liées à des conditions propices au traitement ambulatoire dans la province du Manitoba. Nous avons procédé à une analyse évolutive des tendances, fondée sur la population, à partir de données administratives anonymes recueillies par le Centre des politiques de santé du Manitoba, notamment celles de la période entre 1984-1985 et 2004-2005.
Les résultats indiquent un déclin significatif des taux d'hospitalisations (pour tous les états de santé) suite à la mise en place du PSDMCPNI dans les communautés desservies par les offices de la santé (p<0,0001), les centres de santé (p<0,0001) et les postes infirmiers (p=0,0022). Les communautés desservies par les offices ou les centres de santé ont également connu une réduction substantielle des taux d'hospitalisations pour les états chroniques (p<0,0001).
Les résultats de cette étude indiquent que l'investissement dans les soins à domicile a mené à un déclin significatif des taux d'hospitalisations évitables, particulièrement dans les communautés qui ont un accès limité aux soins de santé primaires.
About the Author(s)
Josée G. Lavoie, PhD, Associate Professor, School of Health Sciences, University of Northern British Columbia, Prince George, BC
Evelyn L. Forget, PhD, Professor, Department of Community Health Sciences, University of Manitoba, Winnipeg, MB
Matt Dahl, BSc, Data Analyst, Manitoba Centre for Health Policy, Department of Community Health Sciences, Faculty of Medicine, University of Manitoba, Winnipeg, MB
Patricia J. Martens, PhD, Director & Senior Research Scientist, Manitoba Centre for Health Policy, Professor, Department of Community Health Sciences, Faculty of Medicine, University of Manitoba, Winnipeg, MB
John D. O'Neil, PhD, Professor and Dean, Faculty of Health Sciences, Simon Fraser University, Vancouver, BC
Correspondence may be directed to: Josée G. Lavoie, PhD, Associate Professor, School of Health Sciences, University of Northern British Columbia, 3333 University Way, Prince George, BC V2N 4Z9; e-mail: Jlavoie0@unbc.ca.
Acknowledgment
The authors would like to acknowledge the participation of the Assembly of Manitoba Chiefs in the planning of this study, and the Chiefs Task Force for their assistance in the analysis of the data. We would also like to acknowledge the Canadian Institutes for Health Research (CIHR) and Manitoba Health, who provided the financial support for this study. We are thankful for the assistance provided by the Manitoba First Nations Centre for Aboriginal Health Research and the Manitoba Centre for Health Policy, University of Manitoba, for use of data contained in the Population Health Research Data Repository (Health Information Privacy Committee, project 2007–005).
The results and conclusions are those of the authors; no official endorsement by the Manitoba Centre for Health Policy, Manitoba Health or other data providers is intended or should be inferred. Patricia J. Martens would like to acknowledge CIHR and the Public Health Agency of Canada (PHAC) for her CIHR/PHAC Applied Public Health Chair (2008–2013).
References
Billings, J., L. Zeital, J. Lukomnik, T.S. Carey, A.E. Blank and L. Newman. 1993. "Impact of Socio-Economic Status on Hospital Use in New York City." Health Affairs 12: 162–73.
Booz Allen and Hamilton Canada. 1969. Study of Health Services for Canadian Indians. Ottawa: Author.
Caminal, J., B. Starfield, E. Sanchez, C. Casanova and M. Morales. 2004. "The Role of Primary Care in Preventing Ambulatory Care Sensitive Conditions." European Journal of Public Health 14: 246–51.
Canada First Nations and Inuit Regional Health Survey National Steering Committee, ed. 2005. "Mapping the Path to Health Equity: First Nation Adults' Access to Primary Health Care Measures." In First Nations and Inuit Regional Health Survey. Ottawa: Health Canada and the Assembly of First Nations.
Canadian Healthcare Association. 2009. Home Care in Canada: From the Margins to the Mainstream. Ottawa: Author.
Canadian Institute for Health Information (CIHI). 2004. Improving the Health of Canadians. Ottawa: Author.
Canadian Institute for Health Information (CIHI). 2006. Pan-Canadian Primary Health Care Indicators: Report 1, Volume 1: Pan-Canadian Primary Health Care Indicator Development Project. Ottawa: Author.
Canadian Institute for Health Information (CIHI). 2007. Health Indicators 2007. Ottawa: Author.
Consilium Consulting Group. 2006. Final Draft, First Nations and Inuit Home and Community Care Project. Ottawa: Assembly of First Nations.
Dyck, R.F. 2001. "Mechanisms of Renal Disease in Indigenous Populations: Influences at Work in Canadian Indigenous Peoples." Nephrology 6: 3–7.
First Nations Regional Health Survey National Committee. 2005. First Nations Regional Longitudinal Health Survey (RHS) 2002/03. Results for Adults, Youths and Children Living in First Nations Communities. Ottawa: Author. Retrieved March 17, 2011. <http://www.fnigc.ca/node/6>.
Health Canada First Nations and Inuit Health Branch (FNIHB). 2003. Health Facility Classification Policy, Working Draft. Ottawa: Author.
Health Canada First Nations and Inuit Health Branch (FNIHB). 2004a. Community Planning Management System (CPMS). Ottawa: Author.
Health Canada First Nations and Inuit Health Branch (FNIHB). 2004b. First Nations and Inuit Home and Community Care Program (FNIHCCP). Study 1, Implementation: "Foundations for Success." Summary Report: Executive Summary and Key Findings. Ottawa: Author.
Health Canada First Nations and Inuit Health Branch (FNIHB). 2004c. First Nations and Inuit Home and Community Care Program: Annual Report 2002–2003. Ottawa: Author.
Kirby, M.J. 2002. The Health of Canadians – The Federal Role. Ottawa: Standing Senate Committee on Social Affairs, Science and Technology. Retrieved March 17, 2011. <http://www.parl.gc.ca/37/2/parlbus/commbus/senate/com-e/soci-e/rep-e/repoct02vol6-e.htm>.
Lavoie, J.G. and E. Forget. 2005. A Financial Analysis of the Current Health Care Expenditures for First Nations in Manitoba. Unpublished manuscript. Winnipeg: Centre for Aboriginal Health Research, University of Manitoba.
Lavoie, J.G., E. Forget, T. Prakash, M. Dahl, P. Martens and J.D. O'Neil. 2010. "Have Investments in On-Reserve Health Services and Initiatives Promoting Community Control Improved First Nations' Health in Manitoba?" Social Science and Medicine 71: 717–24.
Macinko, J., B. Starfield and L. Shi. 2003. "The Contribution of Primary Care Systems to Health Outcomes within Organisation for Economic Co-operation and Development (OECD) Countries, 1970–1998." Health Services Research 38: 831–65.
Marmot, M. and R.G. Wilkinson. 1999. Social Determinants of Health. Oxford: Oxford University Press.
Marshall, M., S. Leatherman, S. Mattke and Members of the OECD Health Promotion, Prevention and Primary Care Panel. 2004. Selecting Indicators for the Quality of Health Promotion, Prevention and Primary Care at the Health Systems Level in OECD Countries. Report no. 16. Paris, France: OECD Technical Papers.
Martens, P., R. Bond, L. Jebamani, C. Burchill, N. Roos and S. Derksen. 2002. The Health and Health Care Use of Registered First Nations People Living in Manitoba: A Population-Based Study. Winnipeg: Manitoba Centre for Health Policy, Department of Community Health Sciences, Faculty of Medicine, University of Manitoba.
Martens, P.J. and R. Fransoo. 2008. "The Need to Know Team." In E. Burland, H. Prior, C. Burchill, L. Romphf, D. Chateau, A. Bailly and C. Ouelette, eds. What Works? A First Look at Evaluating Manitoba's Regional Health Programs and Policies at the Population Level. Winnipeg: Manitoba Centre for Health Policy.
Martens, P.J., B.D. Martin, J.D. O'Neil and M. MacKinnon. 2007. "Distribution of Diabetes and Adverse Outcomes in a Canadian First Nations Population: Associations with Health Care Access, Socioeconomic and Geographical Factors." Canadian Journal of Diabetes 31: 131–39.
Martens, P.J., D. Sanderson and L. Jebamani. 2005. "Health Services Use of Manitoba First Nations People: Is It Related to Underlying Need?" Canadian Journal of Public Health 96(Suppl. 1): S39–S44.
Romanow, R. 2002. Building on Values: The Future of Health Care in Canada. Final Report of the Commission on the Future of Health Care in Canada. Retrieved March 17, 2011. <http://dsp-psd.pwgsc.gc.ca/Collection/CP32-85-2002E.pdf>.
Roos, L. and J. Nicol. 1999. "A Research Registry: Uses, Development, and Accuracy." Journal of Clinical Epidemiology 52: 39–47.
Roos, L., R. Sooden, R. Bond and C. Burchill. 2003. "Working More Productively: Tools for Administrative Data." Health Services Research 38: 1339–57.
Shah, B.R., N. Gunraj and J.E. Hux. 2003. "Markers of Access to and Quality of Primary Care for Aboriginal People in Ontario, Canada." American Journal of Public Health 93: 798–802.
Starfield, B. 1996. "Public Health and Primary Care: A Framework for Proposed Linkages." American Journal of Public Health 86: 1365–69.
Starfield, B., L. Shi and J. Macinko. 2005. "Contribution of Primary Care to Health Systems and Health." Milbank Quarterly 83: 457–502.
Statistics Canada. 2008. "Aboriginal Population Profile Manitoba". Retrieved March 23, 2011. <http://www12.statcan.ca/census-recensement/2006/dp-pd/prof/92-594/details/Page.cfm?Lang=E&Geo1=PR&Code1=46&Geo2=PR&Code2=01&Data=Count&SearchText=Manitoba&SearchType=Begins&SearchPR=01&B1=All&Custom=>.
Tsasis, P. 2009. "Chronic Disease Management and the Home-Care Alternative in Ontario, Canada." Health Services Management Research 22: 136–39.
Victorian Government Department of Human Resources Division. 2001. The Victorian Ambulatory Care Sensitive Conditions Study: Opportunities for Targeting Public Health and Health Services Intervention. Melbourne: Public Health Division, Victorian Government Department of Human Services.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed