
Healthcare Quarterly
Levels of Influence in the Built Environment on the Promotion of Healthy Child Development
There has been a major explosion of research on the built environment and health in the social epidemiology, urban planning, geography and other disciplines over the past several years. Of the portion of this recent research that focuses on children, the bulk of it targets the degree to which the built environment enables or constrains physical activity levels for children, especially routine physical activity such as walking to school, and the impact of such active transportation on outcomes such as obesity (Pabayo et al. 2010; Spence et al. 2008). Another branch of more established research examines the potential for hazards and risks in the built environment to cause harm to children, such as indoor and outdoor air pollution and outcomes such as asthma (Cummins and Jackson 2001).
Obviously, it is important to keep children safe and protected from risks and hazards in the built environment. But in this article, I adopt a different target: understanding the effects of children's built environments on healthy child development. This is a departure from traditional approaches that consider child diseases, disorders and the avoidance of hazards and risks in the built environment, and instead focuses affirmatively on the conditions of the built environment, at multiple geographical scales (i.e., locally, regionally, nationally), that promote healthy child development.
In order for the built environment to be an effective target for child health promotion, it is imperative that we get beyond relatively simple concepts such as the built environment and the mere avoidance of disease and illness and the reduction of hazards. Similarly, there are a number of conceptual models that argue that factors at different levels of social organization matter to healthy child development (e.g., Bronfenbrenner 1977, 1979, 2004), and specify which factors at which levels matter to which aspects of development.
Based on evidence from a study in Vancouver of the effects of the household and neighbourhood scales on kindergarten children's readiness to learn, which I discuss in more detail below (Oliver et al. 2008), there are now clues to tell us which attributes matter at different levels and to what aspects of healthy child development. This will go a long way to directing research that seeks to understand the mechanisms by which our environments affect healthy child development and to subsequently designing health promotion efforts for children.
In the first section of this article, I describe the approach to healthy child development that guides the remainder of the discussion. In the second section, I review seminal work from Urie Bronfenbrenner that describes how built and social environments promote healthy child development. In the final section, I describe some of the challenges that are associated with the adoption of an approach that focuses on the role of built environments in the promotion of healthy child development at a population level.
Domains of Healthy Child Development
In order to conceptualize the impact of the built environment on healthy child development, it is necessary to establish the key elements of child development so that the relative influence of specific built environment factors can be investigated for each element. Following the work of Kagan (1992), Doherty (1997) and Janus and Offord (2007), I adopt the position that the key elements of child development are social knowledge and competence, emotional development and maturity, language and cognitive development, healthy physical development, and communication skills and general knowledge. Social knowledge and competence refers to an "awareness of the general standards of acceptable behaviour in a public place, the ability to control one's own behaviour, the ability to cooperate with others in working together on assignments, appropriate respect for adult authority, and the skills to communicate feelings and wants in socially acceptable ways" (Doherty 1997).
Emotional development and maturity refers to such traits as the self-confidence to try new tasks and to not fear failure. It also includes the abilities to defer immediate gratification, to persist in repetitive exercises that are required for learning complex tasks and to cope with momentary failures without emotional outbursts (Doherty 1997).
Language development refers to such things as understanding the ways in which language can be used symbolically to represent remote or even imaginary events (Doherty 1997), as well as the ability to "understand adults' and other children's verbal communication … and verbally communicate experiences, ideas, wishes, and feelings in a way that can be understood by others" (Doherty 1997: 23). Cognitive development, on the other hand, "refers to the ways in which children perceive, organize, and analyze the masses of information provided by their social and physical environments. Adequate cognitive skills are essential for both the retention and retrieval of information, and for the effective exploration of new experiences" (Doherty 1997: 24). Healthy physical development "goes significantly beyond the concept of freedom from major disease or gross neurological impairment" (Doherty 1997: 21). It includes such factors as physical readiness for activities of daily life, physical independence, gross and fine motor skills and general vitality and resistance to illness (Council on Early Child Development n.d.; Doherty 1997).
Finally, communications skills and general knowledge includes the ability to clearly communicate one's own needs and to understand others, active participation in story-telling and interest in general knowledge about the world (Council on Early Child Development n.d.; Doherty 1997).
Influence of Built Environments at Different Levels on Healthy Child Development
According to Bronfenbrenner (1977, 1979, 2004), there are several necessary propositions about the influence of the environment on child development. Of relevance to this article, Bronfenbrenner suggested that children develop healthily and competently when they benefit from repeated, complex and bi-directional interactions with other people (particularly the primary caretaker) and objects in their everyday life. Healthy interactions are characterized as positive in nature and respectful of the child's person and emotions. He further suggested that development occurs as a joint function of the characteristics of (1) the developing person, (2) the environment – both immediate and remote – in which the processes are taking place, (3) the nature of the developmental outcomes under consideration and (4) the continuities and changes occurring in the environment over time, over the life course and over the historical period in which the person lives (Dunn et al. 2009). Finally, he proposed that mutual emotional attachment between the child and the child's primary caregiver motivate the child's interest in the immediate physical, social and symbolic environment, inviting exploration, manipulation, elaboration and imagination. Given the basic propositions about the processes of healthy child development (in the previous section) and the role of environments in shaping those processes (based on Bronfenbrenner), it becomes possible to develop a more robust conceptualization of the influence of built environments on healthy child development. The combination of these two perspectives invites a very different view on the built environment and child health promotion. It suggests that we need to understand specifically how, and to what extent, specific features of children's environments at different levels affect specific elements of healthy child development. In the next section, I turn to some empirical research that helps with the first steps in such a quest.
Toward a More Specific Model of Built Environments and Healthy Child Development
One of the challenges with most perspectives on how our built environments affect healthy child development is their lack of specificity. Bronfenbrenner (1977, 1979, 2004) described the types of experiences of the environment for children (as above). Moreover, Bronfenbrenner and many after him argued that there are factors at multiple levels or geographical scales (in Bronfenbrenner's terms, these are the microsystem, the exosystem and the mesosystem) that affect healthy child development, but we have relatively little research that tells us what factors, at what levels, are most strongly connected to which developmental processes.
Some recent research suggests a first step in this quest, however. Oliver et al. (2007) investigated the determinants of variations in the Early Development Index (EDI; Janus and Offord 2007) – a measure of kindergarten children's readiness to learn – among the 3,666 kindergarten children (excluding children with special needs) in the Vancouver School District in 2000. The EDI is a teacher-rated scale that consists of 113 questions grouped into five domains (Janus and Offord 2007). It measures the construct known as readiness to learn, which is defined as "the state of a child's neurosystem being ready to develop various skills and neuropathways based on the stimuli it will receive. A child is ready to learn right from birth, and likely even in utero" (Janus et al. 2007: 1). In the EDI, physical health and well-being are assessed by questions that evaluate gross and fine motor skills and the child's independence in looking after his or her own hygienic needs. Social knowledge and competence are assessed by questions that evaluate a child's ability to follow rules, co-operate with others and behave appropriately. Emotional health and maturity are evaluated by questions that gauge a child's ability to deal with his or her own feelings and to respond appropriately to others' feelings. Language and cognitive development are assessed by questions that evaluate reading skills, writing skills, numeracy skills and reading-memory appropriate to the child's age. Communication skills and general knowledge are evaluated by questions that assess a child's ability to communicate in English and his or her age-appropriate knowledge about the world.
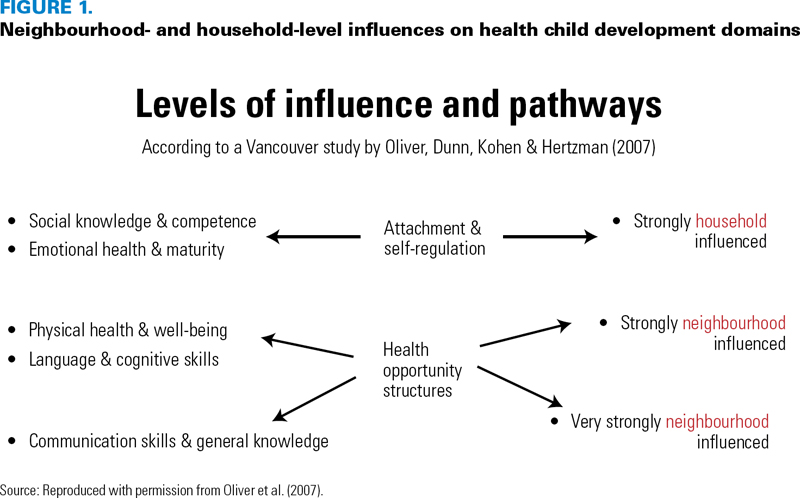
Oliver, et al. (2007) use multi-level modelling, a statistical technique that can separate out the proportion of total variance in the outcome that can be attributed to the neighbourhood level, and the proportion of variance that can be attributed to the household level. Overall Oliver et al.'s (2007) findings suggest that different domains of healthy child development are affected more strongly by some levels of social organization than others. Specifically, physical health and well-being, language and cognitive development and communication skills and general knowledge are more strongly influenced at the neighbourhood level, indicating that neighbourhoods can act as 'health opportunity structures' (Macintyre, et al. 2002) (Figure 1). Aspects of social and emotional well-being, on the other hand, are more strongly affected at the household level.
Based on Oliver et al.'s (2007) findings, there is an obvious role for what we normally think of the built environment. The large literature on aspects of the built environment that promote and inhibit physical activity (e.g., Pabayo et al. 2010; Singh et al. 2010) suggests that the built environment could be altered to enhance at least one aspect of physical well-being – physical activity. Additionally, it is possible to imagine that community recreation facilities and early learning programs addressing cognitive, language and communication skills could be expanded on a neighbourhood basis to significantly increase the stimuli that we now know children require to develop the skills and neuro-pathways needed for healthy trajectories (Janus et al. 2007).
The more challenging finding from Oliver et al.'s (2007) analysis is that there are two domains of healthy child development that are strongly household influenced, namely, social knowledge and competence and emotional health and maturity. As Figure 2 shows, the sensitive periods for areas such as emotional control and habitual ways of responding occur at very young ages. These are outcomes that are influenced by the development of parental attachment and the early establishment of emotional self-regulation. It follows that policy or program efforts in the built environment would be most effectively targeted at parents and the immediate environments of children. Moreover, the specific emphasis would need to be on providing built environment conditions that would help caregivers to have a stronger attachment with their newborn and infant, and help parents to regulate their own emotions so as to aid the child to establish its emotional regulation system.

It follows that the component of the built environment that would exert the greatest influence on social knowledge and competence and emotional health and maturity would be housing conditions. Unfortunately, there is very little research that investigates this question (Leventhal and Newman 2010). According to Bartlett (1998), "There seems to be little doubt that factors in the home environment can buffer children from the effects of other stressors in their lives (or add to those stressors) over the early years, but there is no convincing body of evidence on the effect that housing may have over the longer term." A study by Bartlett (1998) shows that housing inadequacies create stress and conflict among family members and can restrict opportunities for supportive parenting. Evans (2004) has shown that parents in crowded homes are more likely to be less responsive and employ harsher parenting practices. Similarly, Evans et al. (2001) have shown that children who report that they have a place to go to where they can be alone show better task persistence and fewer behavioural problems than children who do not, even with the same crowding levels. Ultimately, however, Leventhal and Newman (2010) argue that almost no research on children has focused on associations between crowding and social and emotional well-being, although there have been studies that examined the relationships between crowding and grade retention and school achievement.
This research need goes well beyond crowding, however, because there is a complex relationship between housing conditions, parenting and child attachment and self-regulation outcomes. On the one hand, it is possible to imagine that studies of housing affordability, design, satisfaction and security would show differences in parental and child outcomes, as Bartlett's (1998) research has shown. But there are undoubtedly other factors that are independent of the built environment that are at work as well, including parenting style, family history, time-use routines etc. Most importantly, the social conventions about the privacy of domestic space protect parenting practices from outside scrutiny and make it challenging for public policy to intervene to improve the outcomes that are related to domestic family relationships: emotional maturity, attachment and self-regulation. Although there are parenting classes, playgroups and other resources offered in communities, the supply of such programs is limited relative to the need, leaving the challenge of achieving a wide reach still to be achieved.
Conclusion
This article has argued that there is a great deal of interest in ensuring that built environments are safe for children and have features that promote their healthy development; this interest has existed for a long time. But in order for the built environment to be an effective target for child health promotion, we need to get beyond relatively simple models that state that factors at different levels matter to healthy child development; we must specify which factors at which levels matter to which aspects of healthy child development. Based on evidence from a study in Vancouver of the effects of the household and neighbourhood scales on kindergarten children's readiness to learn (Oliver et al. 2007), there are now clues to tell us what attributes matter at what levels to what aspects of healthy child development. These clues suggest that there are initiatives that can be undertaken at the neighbourhood level and that such efforts should target language and cognitive skills, communication skills and physical health and well-being. These can also be targeted at older children (i.e., age three years and up), which is appropriate because children of this age have a greater geographical range than younger children. For promoting healthy child development among younger children, the focus must be directed to the household level and on outcomes related to social knowledge and competence and emotional health and maturity. It will be challenging for public policy to address housing affordability, quality, security and design issues. But even more challenging will be penetrating into the domestic lives of families to ensure that very young children get the kind of early stimulation needed to promote healthy child development.
About the Author(s)
James R. Dunn, PhD, is the CIHR-PHAC chair in applied public health and the William Lyon Mackenzie King visiting chair in Canadian studies, at Harvard University (2011–2012), in Cambridge, Massachusetts. He is also an associate professor with the Department of Health, Aging and Society, at McMaster University, in Hamilton, Ontario; a scientist at the Centre for Research on Inner City Health, St. Michael's Hospital, in Toronto, Ontario; and a fellow in the Successful Societies Program, Canadian Institute for Advanced Research (CIFAR), in Toronto. He can be contacted at 905-525-9140, ext. 23832, or by e-mail at jim.dunn@mcmaster.ca.
References
Bartlett, S. 1998. "Does Inadequate Housing Perpetuate Children's Poverty?" Childhood 5: 403–20.
Begley, S. 1996, February 19. "Your Child's Brain." Newsweek 127: 55–62.
Bronfenbrenner, U. 1977. "Toward an Experimental Ecology of Human Development." American Psychologist 32: 513–31.
Bronfenbrenner, U. 1979. The Ecology of Human Development: Experiments by Nature and Design. Cambridge, MA: Harvard University Press.
Bronfenbrenner, U. 2004. Making Human Beings Human: Bioecological Perspectives on Human Development. Thousand Oaks, CA: Sage Publications.
Council on Early Child Development. n.d. The Early Development Instrument (EDI) – A Brief Description. Vancouver, BC: Author. Retrieved March 14, 2012. <http://www.councilecd.ca/internationaledi/09.%20The%20EDI%20-%20A%20Brief%20Description.pdf>.
Cummins, S.K. and R.J. Jackson. 2001. "The Built Environment and Children's Health." Pediatric Clinics of North America 48(5): 1241–52.
Doherty, G. 1997. Zero to Six: The Basis for School Readiness. Ottawa, ON: Human Resources Development Canada.
Dunn, J.R., N. Schaefer-McDaniel and J. Ramsay. 2009. "Neighborhood Chaos and Children's Development: Questions and Contradictions." In: G.W. Evans and T. Wachs, eds., Chaos and Its Influence on Children's Development: An Ecological Perspective. Washington, DC: APA Press.
Evans, G. 2004. "The Environment of Childhood Poverty." American Psychologist 59: 77–92.
Evans, G.W., S. Saegert and R. Harris. 2001. "Residential Density and Psychological Health among Children in Low-Income Families." Environment and Behavior 33(2): 165–80.
Janus, M. and D. Offord. 2007. "Development and Psychometric Properties of the Early Development Instrument (EDI): A Measure of Children's School Readiness." Canadian Journal of Behavioral Science 39(1): 1–22.
Janus, M., S. Brinkman, E. Duk, C. Hertzman, R. Santos, M. Sayers et al. 2007. The Early Development Instrument: Population-Based Measure for Communities. Hamilton, ON: Offord Centre for Child Studies.
Kagan, S.L. 1992. "Readiness Past, Present, and Future: Shaping the Agenda." Young Children 48(1): 48–53.
Leventhal, T. and K. Newman. 2010. "Housing and Child Development." Children and Youth Services Review 32: 1165–174.
Macintyre, S., A. Ellaway and S. Cummins. 2002. "Place Effects on Health: How Can We Conceptualise, Operationalise and Measure Them?" Social Science and Medicine 55: 125–39.
Oliver, L., Dunn, J.R. Kohen, D. and Hertzman, C. 2007. "Do Neighbourhoods Influence the Readiness to Learn of Kindergarten Children in Vancouver? A Multilevel Analysis of Neighbourhood Effects" Environment & Planning A 39(4): 848–68.
Pabayo, R., L. Gauvin, T.A. Barnett, B. Nikiema and L. Seguin. 2010. "Sustained Active Transportation Is Associated with a Favorable Body Mass Index Trajectory across the Early School Years: Findings from the Quebec Longitudinal Study of Child Development Birth Cohort." Preventive Medicine 50(Suppl. 1): S59–64.
Singh, G.K., M. Siahpush and M.D. Koga. 2010. "Neighborhood Socioeconomic Conditions, Built Environments, and Childhood Obesity." Health Affairs 29(3): 503–12.
Spence, J.C., N. Cutumisu, J. Edwards and J. Evans. 2008. "Influence of Neighbourhood Design and Access to Facilities on Overweight among Preschool Children." International Journal of Pediatric Obesity 3(2): 109–16.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed