
Healthcare Quarterly
Key Characteristics of a Fragile Healthcare Supply Chain: Learning from a Pandemic
Abstract
The COVID-19 pandemic has highlighted the many challenges that provincial health systems have experienced while scaling health services to protect Canadians from viral transmission and support care for those who get infected. Supply chain capacity makes it possible for health systems to deliver care and implement public health initiatives safely. In this paper, we present emerging findings from a national research study that documents the key features of the fragility of the health supply chain evident across the seven Canadian provinces. Results suggest that the fragility of the health supply chain contributes to substantive challenges across health systems, thus limiting or precluding proactive and comprehensive responses to pandemic management. These findings inform strategies to strengthen supply chain capacity and performance in order to enable health systems to effectively respond to pandemic events.
Introduction
The COVID-19 pandemic has highlighted significant supply chain challenges in Canada as provincial health systems struggle to manage the impact and spread of the pandemic. In order for health services and public health to meet the unprecedented demands of the COVID-19 pandemic, supply chain and logistics infrastructure have assumed a critical role in ensuring that citizens, health teams and essential workers have the protective products and equipment needed to both mitigate the spread of COVID-19 and achieve optimal outcomes for those who become infected.
Supply chains in health systems source and distribute products to ensure that healthcare teams have timely access to essential products and equipment needed to support the delivery of patient care in a prompt, safe and secure manner. Supply chain infrastructure in health systems includes the movement of products, the people involved and the processes from the manufacturer to the point of care, ensuring that patients receive care when and where needed (Snowdon and Alessi 2016). In contrast to the highly developed supply chain and logistics infrastructure in the private sector, supply chain infrastructure in health systems is profoundly underdeveloped and characterized by antiquated manual systems that are lacking in automation and optimization (Snowdon and Alessi 2016).
Review of the Literature
There is mounting evidence that the failure of the health system supply chain is linked to tragic outcomes when products are not available or when supply chain processes are interrupted and do not function optimally. When supply chain processes are interrupted, or confronted with "stress events," there are severe consequences for health systems, which can place both clinicians and patients at great risk. The Ebola crisis demonstrated that the public-sector supply chain was simply unable to support an effective response to a serious outbreak of Ebola in 2014–2016 (Bell 2016). The rapid spread of Ebola affected a large number of people, largely due to poorly coordinated supply chain infrastructure globally. Flights were grounded, with only two airlines transporting goods to the regions of Africa that were most affected by the outbreak (O'Byrne 2014). This resulted in significant delays in the distribution of needed supplies, such as personal protection and other medical equipment. The outcome was a supply chain failure to provide the supplies required to protect health workers and aid to those citizens living within the outbreak areas. Similarly, during Hurricane Katrina, it is well documented that Walmart, one of the largest retailers in the world, was able to provide supplies more quickly and more efficiently to devastated areas than either FEMA (Federal Emergency Management Agency) or the Red Cross – the very agencies with the mandate to respond to such catastrophic events (Basu and Wright 2008: 7–8). At the time, there was no public organization that had the capacity to proactively predict how best to manage the disaster and no evidence or data to inform a coordinated, proactive response to locate and distribute products such as food, water and generators. There was no distribution or logistics capacity among publicly funded agencies or health systems to move products from where they were sourced to where they were needed in an effort to reduce the risk of devastating outcomes for the citizens of New Orleans. Hurricane Katrina highlighted the role of supply chain infrastructure, digital infrastructure and logistics expertise in supporting a timely, efficient and effective response. This capacity and infrastructure in the private sector were in stark contrast to the relative lack of supply chain and logistics expertise of disaster relief agencies such as FEMA or the Red Cross in the US.
The severe acute respiratory syndrome (SARS) epidemic demonstrated the importance of personal protective equipment (PPE) for the health and safety of health workers. As transmission of the virus was poorly understood and the use of PPE was inadequate to prevent said transmission, three of the 44 Canadians who died of SARS were healthcare workers (Low 2004). In total, 400 persons became ill with SARS, and 25,000 people went into quarantine (Varia et al. 2003). Although public health practices and infection-control procedures improved following the SARS epidemic in Canada, supply chain practices in Canadian health systems did not change.
In the US, there was a significant shortage of N95 respirator masks and face masks during the 2009 H1N1 influenza pandemic (Rebmann and Wagner 2009; Srinivasan et al. 2004) primarily due to the limited ability of the supply chain to sufficiently increase production when demand suddenly increased (Patel et al. 2017). The shortage resulted in significant back orders of supplies, such as N95 respirators, necessary for providing safe work environments for health professionals (Patel et al. 2017; Rebmann and Wagner 2009). The inability to properly plan and forecast usage led to the stockpiling of supplies by healthcare organizations should the pandemic worsen and the need for products increase (Patel et al. 2017).
Pandemics and epidemics are unique in their disruption of supply chains as these result in changes to both the supply and the demand of products (Ivanov and Dolgui 2020). Supply chain experts estimate that approximately 36,009 unique products are required for the delivery of care during a pandemic (Symmetric Health Solutions 2020). Health systems rely on supply chain teams to source and distribute everything, from beds to ventilators, intravenous (IV) pumps and tubing, medications and vaccines, PPE and endotracheal tubes, all necessary to provide safe and high-quality healthcare.
Supply Chain Challenges during the COVID-19 Pandemic
The COVID-19 pandemic brought forward new and diverse supply chain challenges experienced by global health systems. In the first wave of COVID-19, the worldwide shortage of ventilators was a challenge for many health systems grappling with the rapid surge of patients with severe COVID-19 (lyengar et al. 2020). Patients required mechanical ventilation that necessitated the rationing of ventilators in some jurisdictions (Truog et al. 2020). The capacity to offer patients with severe COVID-19 intensive care and mechanical ventilation was a life-or-death decision for these health systems (Iyengar et al. 2020). The shortage of PPE (e.g., masks, gowns, gloves, face shields) and lab testing supplies has profoundly impacted the ability of health systems to initiate surveillance methods, protect vulnerable population groups (e.g., the elderly, citizens with health conditions) and safely care for COVID-19 patients, resulting in high rates of COVID-19 infections in the global health workforce (ICN 2020). Recently, when primary care teams in Italy were asked to conduct widespread testing for COVID-19 surveillance following the first wave of the pandemic, the Federation of General Practitioners refused to assume this responsibility without assurances that PPE would be available to protect both physicians and citizens (Paterlini 2020). In the second wave of COVID-19, Italy experienced a greater volume of cases than was experienced during the first wave, which overwhelmed their health system.
Supply chains in the healthcare sector are complex (Abdulsalam et al. 2015; Landry and Beaulieu 2013), often involving multiple stakeholders, such as organizations, clinicians, providers and patients. The number and variation of products used in healthcare settings (e.g., medications, PPE, essential equipment such as ventilators, beds, monitors) contribute to this complexity (Abdulsalam et al. 2015). The unique features that characterize healthcare supply chains hinder the direct extrapolation of research evidence from other sectors for application to the healthcare supply chain strategy (Gendy and Lahmar 2019).
The complexity of the health supply chain
The study of healthcare supply chains has gained momentum over the past decade. However, significant gaps remain in research on the health supply chain, especially when compared to business sectors (Dixit et al. 2019; Gendy and Lahmar 2019; Kumar and Blair 2013). This includes gaps in research on areas such as digitally enabled supply chain infrastructure and risk-management strategies (Dixit et al. 2019). It is critically important to identify supply chain fragility in healthcare systems, not only because of the essential role global health supply chains assume in pandemic responsiveness but also because healthcare supply chains – and their fragility – directly impact human life.
COVID-19 outcomes have been widely recognized, at least in part, as a failure of supply chain capacity in health systems (Dai et al. 2020a, 2020b), returning us to the central focus of this paper: the identification of the key characteristics of supply chain fragility, which contributed to the inability of Canadian health systems to adequately respond to, and manage, the COVID-19 pandemic. Identifying the causes and characteristics of supply chain fragility can inform health system strategy to overcome the fragility of the health supply chain and build knowledge and awareness of the centrality of the health supply chain as an asset for pandemic preparedness and management.
This paper describes the characteristics of a fragile healthcare supply chain – a fragility exposed and exacerbated in most Canadian provinces by the COVID-19 pandemic. The term "fragility" in this paper describes supply chain characteristics and features that are easily disrupted or overwhelmed when placed under extreme stress, such as the stress of a pandemic situation. A fragile supply chain is extremely vulnerable to external vicissitudes and "stress events." Our assessment of supply chain fragility is informed by the emerging themes and findings of an ongoing COVID-19 operating grant (CIHR Ref. VR5 172669), which has used qualitative methods to examine the perceptions, experiences and perspectives of over 130 health system leaders, across seven participating provincial health systems. The purpose of this paper is to draw lessons from the current pandemic and isolate the key characteristics of supply chain fragility that are persistent across the provincial healthcare supply chain infrastructure in Canada.
Methodology
This paper features emerging findings from an ongoing COVID-19 Rapid Research Funding Opportunity called "Development of an Implementation Framework to Advance Provincial and National Health System Supply Chain Management of the COVID-19 Pandemic." A variety of sources were relied upon to inform this empirical study. Secondary data sources included government websites, media resources, reports, academic literature and grey literature. Findings emerging from analyses of secondary data and the conceptual framework guided qualitative interviews that were the primary source of data. Semi-structured interviews were conducted to elicit the perspectives and experiences of key informants from each participating province – British Columbia, Alberta, Manitoba, Ontario, Quebec, Nova Scotia and Newfoundland and Labrador. Theoretical sampling was used to identify 132 participants who represented varied perspectives and expertise in each provincial health system. Key stakeholders interviewed included supply chain teams, procurement teams, senior health system leaders, physicians, clinician teams, and leaders from public health, long-term care, hospitals, residential care, government, distributors and group purchasing organizations.
Interviews were audio-recorded, transcribed verbatim and analyzed using NVivo Transcription software. Qualitative data analysis was completed using inductive content analysis to generate new knowledge, grounded in participant data (Elo and Kyngas 2008). Interview transcripts were reviewed repeatedly and then coded and organized into smaller, more manageable segments. The coding scheme was designed using a systematic and analytic procedure to create a map of conceptual categories, with definitions and exemplars for each code and category (Hsieh and Shannon 2005). Themes were identified that linked the meanings of these conceptual categories. Content analysis was iterative, such that coded transcripts were revisited repeatedly as new insights surfaced during data collection and analysis. Data collection for this study continues; the findings reported in the following section represent experiences and perspectives from the first wave of the COVID-19 pandemic.
Findings: Fragility in the Health Supply Chain
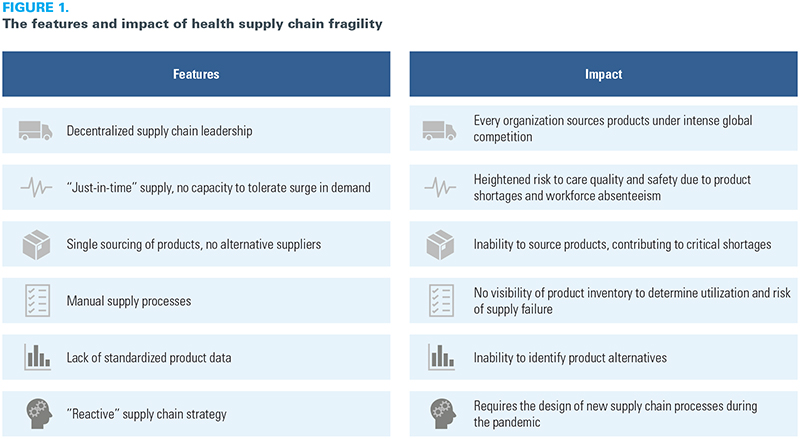
Emerging from the analysis of key informant interviews were common themes that indicated the features and impact of health supply chain fragility (Figure 1). Six key features of supply chain fragility emerged from the qualitative analysis: decentralized and distributed supply chain management; limited or no supply capacity to manage a surge in demand; reliance on single-jurisdiction or -supplier sourcing; a lack of supply transparency; a lack of interjurisdiction collaboration; and a reactive pandemic response strategy. We address each in the following section.
{kind=link}
Decentralized and distributed supply chain management
Supply chain leadership models in Canadian health systems are diverse in structure (e.g., centralized in some provinces, decentralized in others), with little or no coordination across provincial jurisdictions (Beaulieu et al. 2018). For example, Ontario and Quebec have decentralized supply chain management, whereby regional and organizational teams manage the supply chain and procurement independently. In a decentralized model, every health organization (e.g., hospitals, long-term care, primary care, community agencies, rehabilitation facilities) individually manages the sourcing and procurement of supplies and equipment needed for care delivery. In a decentralized model, there is no coordination of supply chain management across regions or across the province. Organizations manage the supply chain independently, resulting in little or no provision for provincial leaders to track supply inventories across organizations and no way to measure or track rates of product utilization across the province. More distributed supply chain management was associated with less capacity for the coordination of the sourcing and procurement of the critical products required to ensure that health systems can safely and effectively deliver care. Provincial leaders in decentralized models described a lack of availability of supply chain data, which made it impossible to identify organizations at greatest risk and to ensure that product allocations were prioritized accordingly. During critical-product shortages, informants working within decentralized supply chain jurisdictions described intense competition, whereby every organization was competing for sources of critical products within and across jurisdictions. During the first wave of the pandemic, the demand for products and equipment surged to unprecedented levels. Organizations rapidly exhausted their product supply and, therefore, faced intense competition with every other provincial organization – as well as with every other global jurisdiction – to procure products. In Ontario and Quebec, the decentralized supply chain management revealed a high degree of variation of supply chain expertise, capacity and experiences across health organizations, with informants commonly reporting little or no capacity to track product and equipment inventories, locations or utilization rates. Health system leaders described significant challenges in their decision-making processes concerning the allocation of critical products. They had no ability to identify the organizations that were at the greatest risk due to shortage of protective equipment (e.g., long-term care settings). There was also no coordination across regions to inform teams of the locations with product surpluses, which would have allowed for the redistribution of products to where they were needed the most, such as communities experiencing an outbreak.
In contrast, in a centralized supply chain management scenario, as evident in British Columbia, Alberta and Newfoundland and Labrador, designated teams were accountable for all supply chain management decisions across the province that were often supported and informed by a province-wide supply chain data infrastructure. Centralized supply chain management described the transparency of product inventories to regions and organizations across these provinces, where identification and location of products and equipment were easily done, and the utilization rate (e.g., burn rate) of products was well defined in each region or organization. Centralized supply chain management enabled a highly coordinated sourcing strategy, whereby distribution of products across a region or province was prioritized to every health organization based on need.Accordingly, due to its very limited capacity to coordinate supply chain management strategies, findings suggest that decentralized supply chain management creates a very fragile and highly chaotic environment in which every organization is on their own in managing severe product shortages and distributing the products critically needed for care delivery. Ontario and Quebec were also the two provinces with the highest rates of COVID-19 infections in long-term care settings. The decentralized model of supply chain strategy resulted in these organizations procuring their own PPE products during the first wave of COVID-19, accessing provincial supplies only if they had an outbreak at their facility.
Inability to manage surge in demand
A key challenge in the first wave of the COVID-19 pandemic was the inability of health systems to respond rapidly to a massive surge in demand for PPE. Health system capacity was quickly overwhelmed in Italy, Spain, New York and other global jurisdictions. Health system leaders in Canada reported experiencing a rapid and unexpected surge in the utilization of and demand for PPE, even before the identification of the first case of COVID-19. The sudden and exponential increase in demand for PPE and other critical supplies overwhelmed supply chain inventory in most provinces. Product inventory was rapidly diminished, and pandemic stockpiles were either non-existent or insufficient to meet the scope and scale of the demand for PPE. In many cases, pandemic supply had not been appropriately managed (e.g., critical supplies had been left to expire and were not replenished) and/or had been discarded prior to the COVID-19 pandemic (often due to cost-saving pressures).
Leaders of long-term care, homecare and community organizations described being quickly overwhelmed as PPE resources were exhausted in a matter of days and both staff and residents became infected with COVID-19. Two of the most dominant challenges for health organizations were the availability of workers and high absenteeism rates, often reported as 30%, which resulted in a heavy reliance on temporary workers (e.g., agencies) to support care delivery. In addition, all informants from these organizations described the struggle to provide adequate PPE that is required to safely deliver care to patients.During the early phases of the COVID-19 pandemic, provinces such as Ontario and Quebec focused their attention on conserving critical supplies and, in anticipation of the surge in demand for acute-care bed capacity, prioritized resources for hospitals. Lacking pandemic stockpiles, neither of these provinces had the capacity to manage the surge in demand for protective equipment. Moreover, existing supply inventories at the organization level were unknown to provincial leaders. The inability to manage the surge in demand for product and equipment supply resulted in the decision to prioritize protective equipment and bed capacity for hospitals, which resulted in all other health organizations having to source and procure protective equipment on their own. As public health teams focused on initiatives to "flatten the curve" (i.e., mitigate the spread of the virus) to reduce demand on acute care services, provinces such as Ontario and Quebec did not have the capacity to supply community organizations (e.g., long-term care, home care, primary care) with protective equipment during the first wave of the pandemic. The long-term care workforce had limited access to PPE, and the rates of infection among seniors in long-term care accounted for over 80% of deaths due to COVID-19 in Canada (CIHI 2020). The limited capacity to meet the surge in demand is a feature of supply chain fragility. The first wave of the COVID-19 pandemic was described by the majority of key informants as characterized by a very limited ability to manage the surge in demand for the products critically needed by health teams to safely deliver care and support preventive efforts to contain or reduce the spread of the virus.
Reliance on product sourcing from single geographies or limited supply sources
A key factor in health supply chain fragility described by respondents from every province was the dominant reliance on a single geographic source (e.g., China, which was the first jurisdiction to be shut down to contain the virus) for critical products. Clinical procurement efforts over the past decade have often prioritized product procurement at the lowest possible cost. Manufacturers of health products compete aggressively for lucrative health system contracts by offering the lowest possible pricing, which can only be achieved by manufacturing in jurisdictions with low labour costs. Competitive pricing has resulted in what many leaders described as 90% of health products in North America being sourced from manufacturers in China. When the pandemic was declared by the World Health Organization, it became quickly evident that the global supply of critical products (e.g., face masks, gowns, testing kits, N95 masks) was inadequate to meet the rapid surge in demand across every global jurisdiction. Provincial health systems in Canada were highly dependent on long health supply chains and offshore suppliers and manufacturing capacities, with no alternative supplier sources in other geographies. Health supply chain leaders described their existing or contracted supplier networks as unable to respond to the increased surge in demand or offer alternative sources for critical products; this was often attributed to a lack of redundancy in the health supply chain described as a by-product of the tendency toward a "just-in-time" supply chain model that privileges "leanness" over resiliency and domestic manufacturing capacity. This lack of redundancy was compounded by the lack of diversity in the health supply chain: reliance on a single geographic source often corresponded to a lack of substantial domestic manufacturing or supply capacity. Some provinces, such as Newfoundland and Labrador and Nova Scotia, worked to remedy this lack of supply chain diversity through the cultivation of their own domestic manufacturing capacity and local supplier network, which helped to diversify and support their health supply chains.Reliance on a single geographic source created an impossible supply chain situation in Canada. Products critical to patient care, the safety of the health workforce and public health efforts to contain the virus were in very short supply as companies sold products to the highest bidder. Due to this intense competition, supply chain teams had to "buy now" or lose the opportunity to procure the product, and they had little ability to validate the quality or certify the authenticity of products. In many instances, products from new suppliers were found to not meet quality standards and were discarded. In some instances, products never arrived as companies diverted product deliveries to health systems offering to pay higher prices.
Intense competition for critical pandemic products unfolded rapidly across all global jurisdictions, leaving Canada at a distinct disadvantage. The lack of coordination across organizations, provinces and federal agencies stymied the rapid sourcing and distribution of products to regions most heavily affected by COVID-19. Due to its large landmass and relatively small population, Canada's influence and buying power in the global marketplace were described as "limited" compared to other countries. Reliance on single-jurisdiction sourcing, or single-supplier sourcing (e.g., reliance on 3M as the dominant supplier of N95 masks), was another key characteristic of supply chain fragility, one that poses a great risk for supply chain failure because of the limited capacity to compete globally to find alternative sources during supply shortages.
Manual supply chain processes with limited digital infrastructure
Health system supply chain infrastructure in Canada varied widely across the seven provinces participating in this study. The lack of digital infrastructure in Canada's health supply chain results in a lack of transparency, making it impossible for ministry or health system leaders to make decisions informed by accurate supply chain data (Snowdon and Alessi 2016). Leadership decisions during the initial phase of COVID-19 have been described by one physician leader as "flying blind," meaning that leaders made decisions on the use and sourcing of PPE without any data to accurately track products and supplies on hand and the location of supplies and product utilization rates (e.g., burn rate) or to accurately forecast demand. Digitally enabled inventory management tools were described by leaders in British Columbia, Alberta, Manitoba and Newfoundland and Labrador to support supply chain management and provide data on the levels of inventory on hand. In other provinces, inventory management was typically manual and profoundly underdeveloped in smaller hospitals and in community organizations such as those in homecare, residential care and long-term care settings. Where such inventory management systems did exist, they were neither interoperable nor integrated across regions or jurisdictions, making it impossible to track supply (e.g., product inventory, location and availability of equipment) or demand (e.g., product utilization rates). In many provinces, health system leaders relied on manual counting of critical products daily, which was then reported to the ministry in order for inventory data to be collected. This manual counting and reporting process was created in Ontario in the early phase of the first wave of COVID-19 and described as a "virtual inventory," which has continued throughout the summer and fall months of 2020.
By comparison, Alberta has a highly digitized supply chain infrastructure and reported experiencing few supply chain challenges throughout the first phase of the COVID-19 pandemic. Alberta was also able to support other provinces by supplying PPE to Ontario and Quebec, where significant outbreaks had unfolded, particularly in long-term care settings, which further fuelled high demand for protective products across both provinces.
The lack of digital infrastructure in provincial health systems resulted in a complete lack of transparency (i.e., "flying blind") of supply inventories, with no ability for health system leaders and decision makers to track or forecast use of products either within or across provincial and territorial jurisdictions. The lack of robust digital infrastructure and reliance on manual supply chain processes is another feature of fragility in the health supply chain.
Lack of standardization of products and product data
Shortages of critical supplies during the early weeks of the pandemic resulted in supply chain teams having to source alternative products (e.g., KN95 masks) to ensure that protective equipment was available for health teams. Senior health system leaders described the strategy of creating specialized teams to source products in critical shortages. These teams quickly realized that there was no standardized product identification. The lack of product attribute or specifications data contributed to a complete lack of capacity toward accurate identification of product attributes or product specifications. Without product data, there was no way for these sourcing teams to evaluate new sources of products, or alternative products, to determine whether alternative types of products could be substituted for critical products in short supply. The lack of global standards for product identification also made it impossible for teams to distinguish suppliers selling counterfeit products looking to leverage the desperation of health systems trying to purchase high-demand products from suppliers selling legitimate products. Newfoundland and Labrador relied on partnerships with university labs to test product performance and functionality to determine product attributes. With the exception of Alberta, health system leaders in many provinces reported that global standards had not been adopted; hence, they were unable to accurately identify products and product attributes or to enable the traceability of products from the manufacturer to their use during patient care. Lack of global standards adoption to support accurate product identification, assess product equivalency and enable global traceability is a feature of supply chain infrastructure fragility.
Reactive supply chain responsiveness
The final characteristic of supply chain fragility is "reactivity." A reactive health supply chain mobilizes resources in the wake of an acute surge event or supply interruption; it does not anticipate, or plan for, such events and is unable to proactively mobilize resources to ensure that supplies, products, medications and equipment are available when and where they are most needed. A "reactive" approach was clearly described by leaders in a number of provinces, whereby processes had to be established to manually manage product inventory to respond to the demand surge for products in the early phases of the pandemic. As mentioned earlier, leaders in Ontario described developing a "virtual inventory," meaning that all organizations were asked to manually count supplies and report inventories daily. This virtual inventory was designed by consultants, who were contracted during the unfolding of the first wave of the COVID-19 pandemic in Ontario. This was a reactive strategy for managing a surge in demand for the critical products and equipment that are required to support health systems.Other provincial leaders resorted to managing product inventory using allocation formulas to limit the volume of products that a clinical team or setting was able to access. Health systems in British Columbia, Alberta, Ontario, Nova Scotia and Newfoundland and Labrador used allocation formulas to conserve available product inventory and guard against the "hoarding" behaviours that were observed when organizations attempted to order extraordinary volumes of products. In times of crisis, then, a reactive health supply chain is vulnerable to the pressures of acute surge events and to the corollaries of this vulnerability, such as product shortages, supply interruptions and delays in sourcing the products critical to patient care delivery and the mitigation of public health risk. In this way, reactivity, as a characteristic of supply chain fragility, highlights the central concern of this paper: the relationship between the strength of the health system supply chain and the safety of patient care delivery and the healthcare workforce.
Conclusion
The purpose of this paper has been to articulate the key characteristics of health supply chain fragility, informed by the experiences and perspectives of health and health supply chain leaders and stakeholders in Canadian health systems during the COVID-19 pandemic. The pandemic has brought into view six features of the fragility of Canada's current health supply chain. This paper has attempted to make clear that during times of crisis, such as a pandemic, Canada's healthcare supply chain is unable to meet the surge in demand for the products that are critical for safe delivery of patient care and public health initiatives. The fragility of the health supply chain limits the capacity of our health system to both effectively and safely deliver patient care to those infected with the virus and protect the health workforce from the transmission of the disease. The findings to date inform new strategies and approaches for strengthening supply chain fragility to better support pandemic management and health system performance. Health supply chain infrastructure must be thought of as a dynamic synergy that is foundational to the capacity of a health system to safely deliver high-quality healthcare.
About the Author(s)
Anne W. Snowdon, BScN, MSc, PhD, is the scientific director and chief executive officer of SCAN Health, an international knowledge translation platform that engages health system leaders and supply chain experts to advance global capacity to adopt and scale best practices in the healthcare supply chain to offer traceability of products and care processes from bench to bedside to patient outcomes. She is a full professor of Strategy and Entrepreneurship at the Odette School of Business, University of Windsor in Windsor, ON. She can be reached by e-mail at anne.snowdon@uwindsor.ca.
Michael Saunders, PhD, is a postdoctoral fellow in the Supply Chain Advancement Network in Health (SCAN Health) at the University of Windsor in Windsor, ON. He can be reached by e-mail at michael.j.saunders@uwindsor.ca.
Alexandra Wright, MPA, is a research analyst in the Supply Chain Advancement Network in Health (SCAN Health), University of Windsor. She is also a PhD candidate at the Dalla Lana School of Public Health, Institute of Health Policy, Management and Evaluation at the University of Toronto in Toronto, ON.
References
Abdulsalam, Y., M. Gopalakrishnan, A. Maltz, and E. Schneller. 2015. Health Care Matters: Supply Chains in and of the Health Sector. Journal of Business Logistics 36(4): 335–39. doi:10.1111/jbl.12111.
Basu, R. and J.N. Wright. 2008. Total Supply Chain Management. Elsevier: Butterworth-Heinemann.
Beaulieu, M., J. Roy and S. Landry. 2018. Logistics Outsourcing in the Healthcare Sector: Lessons from a Canadian Experience. Canadian Journal of Administrative Sciences 35(4): 635–48. doi:10.1002/cjas.1469.
Bell, B.P., I.K. Damon, D.B. Jernigan, T.A. Kenyon, S.T. Nichol, J.P. O'Connor et al. 2016. Overview, Control Strategies, and Lessons Learned in the CDC Response to the 2014–2016 Ebola Epidemic. Morbidity and Mortality Weekly Report 65(Suppl. 3):4–11. doi:10.15585/mmwr.su6503a2.
Canadian Institute for Health Information (CIHI). 2020, June. Pandemic Experience in the Long-Term Care Sector: How Does Canada Compare with Other Countries? Retrieved December 1, 2021. <https://www.cihi.ca/sites/default/files/document/covid-19-rapid-response-long-term-care-snapshot-en.pdf>.
Dai, T., M.H. Zaman, W.V. Padula and P.M. Davidson. 2020a. Supply Chain Failures amid Covid-19 Signal a New Pillar for Global Health Preparedness. Journal of Clinical Nursing. Advance online publication. doi:10.1111/jocn.15400.
Dai, T., G. Bai and G.F. Anderson. 2020b. PPE Supply Chain Needs Data Transparency and Stress Testing. Journal of General Internal Medicine 35(9): 2748–49. doi:10.1007/s11606-020-05987-9.
Dixit, A., S. Routroy and S.K. Dubey. 2019. A Systematic Literature Review of Healthcare Supply Chain and Implications of Future Research. International Journal of Pharmaceutical and Healthcare Marketing 13(4): 405–35. doi:10.1108/IJPHM-05-2018-0028.
Elo, S. and H. Kyngas. 2008. The Qualitative Content Analysis Process. Journal of Advanced Nursing 62(1): 107–15. doi:10.1111/j.1365-2648.2007.04569.x.
Gendy, A.W.A. and A. Lahmar. 2019. Review on Healthcare Supply Chain [conference paper]. 2019 IEEE/ACS 16th International Conference on Computer Systems and Applications (AICCSA) (pp. 1–10). doi:10.1109/AICCSA47632.2019.9035234.
Hsieh, H.-F. and S.E. Shannon. 2005. Three Approaches to Qualitative Content Analysis. Qualitative Health Research 15(9): 1277–88. doi.org/10.1177/1049732305276687.
International Council of Nurses (ICN). 2020, September 14. Protecting Nurses from COVID-19 a Top Priority: A Survey of ICN's National Nursing Associations. Retrieved December 1, 2020. <https://www.icn.ch/system/files/documents/2020-09/Analysis_COVID-19%20survey%20feedback_14.09.2020%20EMBARGOED%20VERSION_0.pdf>.
Ivanov, D. and A. Dolgui. 2020. Viability of Intertwined Supply Networks: Extending the Supply Chain Resilience Angles towards Survivability. A Position Paper Motivated by COVID-19 Outbreak. International Journal of Production Research 58(10): 2904–15. doi:10.1080/00207543.2020.1750727.
Iyengar, K., S. Bahl, R. Vaishaya and A. Vaish. 2020. Challenges and Solutions in Meeting Up the Urgent Requirement of Ventilators for COVID-19 Patients. Diabetes & Metabolic Syndrome: Clinical Research & Reviews 14(4): 499–501. doi:10.1016/j.dsx.2020.04.048.
Kumar, S. and J.T. Blair. 2013. U.S. Healthcare Fix: Leveraging the Lessons from the Food Supply Chain. Technology and Health Care 21(2): 125–41. doi:10.3233/THC-130715.
Landry, S. and M. Beaulieu. 2013. The Challenges of Hospital Supply Chain Management, from Central Stores to Nursing Units. In: B. Denton, ed., Handbook of Healthcare Operations Management (Vol. 184, pp. 465–82). Springer. doi:10.1007/978-1-4614-5885-2_18.
Low, D.E. 2004. SARS: Lessons from Toronto. Institute of Medicine (US) Forum on Microbial Threats. In S. Knobler, A. Mahmoud, S. Lemon, A. Mack, L. Sivitz and K. Oberholtzer, eds., Learning from SARS: Preparing for the Next Disease Outbreak (pp. 63–70). National Academies Press.
O'Byrne, R. 2014, November 3. The Ebola Outbreak and Why Logistics Are Struggling to Cope. Logistics Bureau. Retrieved December 1, 2020. <http://www.logisticsbureau.com/the-ebola-outbreak-and-why-logistics-are-struggling/>.
Patel, A., M.M. D'Alessandro, K.J. Ireland, W.G. Burel, E.B. Wencil and S.A. Rasmussen. 2017. Personal Protective Equipment Supply Chain: Lessons Learned from Recent Public Health Emergency Responses. Health Security 15(3): 244–52. doi:10.1089/hs.2016.0129.
Paterlini, M. 2020. Covid:19: Italy Has Wasted the Sacrifices of the First Wave, Say Experts. BMJ 371: m4279. doi:10.1136/bmj.m4279.
Rebmann, T. and W. Wagner. 2009. Infection Preventionists' Experience during the First Months of the 2009 Novel H1N1 Influenza A Pandemic. American Journal of Infection Control 37(10): e5–16. doi:10.1016/j.ajic.2009.09.003.
Snowdon, A. and C. Alessi. 2016. Visibility: The New Value Proposition for Health Systems. Retrieved December 1, 2020. World Health Innovation Network. <https://issuu.com/worldhealthinnovationnetwork/docs/full_paper_-_win_visibility_thought/1?e=25657717/39177387>.
Srinivasan, A., D.B. Jernign, L. Liedtke and L. Strausbaugh. 2004. Hospital Preparedness for Severe Acute Respiratory Syndrome in the United States: Views from a National Survey of Infectious Diseases Consultants. Clinical Infectious Diseases 39(2): 272–74. doi:10.1086/421777.
Symmetric Health Solutions. 2020, July 13. List of Medical Supplies at Risk of Shortage during COVID-19. Retrieved December 1, 2020. <https://www.symmetrichealthsolutions.com/blog/covid19-high-risk-supplies-list>.
Truog, R.D., C. Mitchell and G.Q. Daley. 2020. The Toughest Triage – Allocating Ventilators in a Pandemic. New England Journal of Medicine 382(21): 1973–75. doi:10.1056/NEJMp2005689.
Varia, M., S. Wilson, S. Sarwal, A. McGeer, E. Gournis, B. Henry and Hospital Outbreak Investigation Team. 2003. Investigation of a Nosocomial Outbreak of Severe Acute Respiratory Syndrome (SARS) in Toronto, Canada. CMAJ 169(4): 285–92.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed