
Healthcare Quarterly
Is Ontario Ready for the Health Costs Associated With Dementia?
Abstract
People living with dementia require care from a variety of health professionals and in different settings to optimize their quality of life. A phase-based approach to costing health system use supports our understanding of the longitudinal costs of care through disease progression at a population level. This report estimates five-year and phase-based net health system costs of dementia.
Introduction
While close to 770,000 Canadians live with dementia from Alzheimer's disease or other causes (hereafter dementia), few effective therapies exist, and most focus on symptom management (Alzheimer Society of Canada 2025; Marasco 2020). The prevalence of dementia in Canada is projected to increase more than twofold in the next several decades, largely due to demographic trends that include the increased longevity of older adults (Manuel et al. 2016). Consequently, dementia-related health system resource utilization and its associated costs are also anticipated to increase. People living with dementia require support from a variety of different healthcare providers and sectors, including family physicians, dementia specialists (e.g., geriatricians, neurologists) as well as home care to allow them to live in the community and maximize their quality of life (CIHI 2018). Long-term care facilities provide important, specialized care for people living with dementia who are not able to live at home and require more intensive personal support and nursing care; however, care in these settings is costly (Grignon and Spencer 2018).
Internationally, dementia costing studies have examined the macroeconomic burden of dementia (Chen et al. 2024) as well as health system costs (Edwards et al. 2024; Zilling et al. 2025). In Canada, prior studies have examined the total economic burden of dementia (Adlimoghaddam et al. 2018) and variation in dementia health system costs by multi-morbidity (Griffith et al. 2019; Tonelli et al. 2022); however, few estimates of the longitudinal health system costs of dementia by phase of disease are available. A greater understanding of health system costs incurred by people living with dementia can help policy makers and health system planners anticipate future needs throughout the different stages of dementia progression. A phase-based costing approach allows for the estimation of costs of care across different stages of the disease, allowing for an in-depth examination of contributors to costs of care. This method is commonly used to study costs associated with cancer diagnoses (de Oliveira et al. 2016). We used ICES data to estimate the net health system costs of dementia by phase of care and over a five-year period after new dementia ascertainment to quantify the impact of this condition on the health system in Ontario.
Approach
We conducted a population-based, propensity-score matched cohort study among older adults newly ascertained with dementia residing in the community. Linked health administrative databases were used to obtain information on health insurance eligibility and demographics and to characterize health system costs. These datasets were linked using unique encoded identifiers and analyzed at ICES. ICES is an independent, non-profit research institute whose legal status under Ontario's health information privacy law allows it to collect and analyze healthcare and demographic data, without consent, for health system evaluation and improvement. The use of data in this project was authorized under section 45 of Ontario's Personal Health Information Protection Act (Province of Ontario 2004) and does not require review by a Research Ethics Board. All analyses were conducted using SAS Version 9.4 (SAS Institute Inc.).
We included Ontario residents aged 66 years and older who were newly ascertained with dementia between April 1, 2010 and March 31, 2017. Dementia status was obtained using a validated health administrative data algorithm (Jaakkimainen et al. 2016). Potential controls were selected from individuals who had no previous dementia and who were alive at the start of the accrual period and were matched to those with dementia. People residing in long-term care facilities were excluded.
Phase-based costs of care
People living with dementia and controls were followed to either death or the end of the observation period (March 31, 2018). We attributed individual-level, direct, health system costs covered by provincial health insurance using methods described previously (Wodchis et al. 2013). All costs were calculated on an annualized basis and standardized to 2018 Canadian dollars. We used a phase-based costing methodology to examine mean net costs of dementia throughout the phases of disease progression: (1) pre-ascertainment (one year prior to dementia when assessments may occur); (2) initial phase (up to one year following dementia ascertainment when therapies and related care may be initiated); (3) continuing phase (period between initial and terminal phases when continuing dementia care may be provided); and (4) terminal phase (up to one year period prior to death when end of life care may be provided). We calculated the mean net annual costs of care by subtracting costs incurred by controls from costs incurred by people living with dementia. We also calculated five-year costs.
Key Findings
We were able to match 164,640 people newly living with dementia (88% of those living in the community and newly ascertained during the study period) to a control living without dementia. People living with dementia and controls were well-balanced in demographic characteristics (Table 1) and comorbidities. Both groups were on average 81.3 years of age, and 58.7% were females.
| TABLE 1. Characteristics of people living with dementia and matched controls | ||
| Characteristics | Dementia (N = 164,640) |
Controls (N = 164,640) |
| Age (years) | ||
| 66–74 years | 30,588 (18.6%) | 29,927 (18.2%) |
| 75–84 years | 76,660 (46.6%) | 77,610 (47.1%) |
| ≥ 85 years | 57,392 (34.9%) | 57,103 (34.7%) |
| Female sex | 96,715 (58.7%) | 96,715 (58.7%) |
| Income quintile | ||
| 1 (lowest) | 36,268 (22.0%) | 37,147 (22.6%) |
| 2 | 36,028 (21.9%) | 36,025 (21.9%) |
| 3 | 31,992 (19.4%) | 32,138 (19.5%) |
| 4 | 30,054 (18.3%) | 29,629 (18.0%) |
| 5 (highest) | 30,298 (18.4%) | 29,701 (18.0%) |
| Rural | 20,126 (12.2%) | 21,113 (12.8%) |
Phase-based costs of care
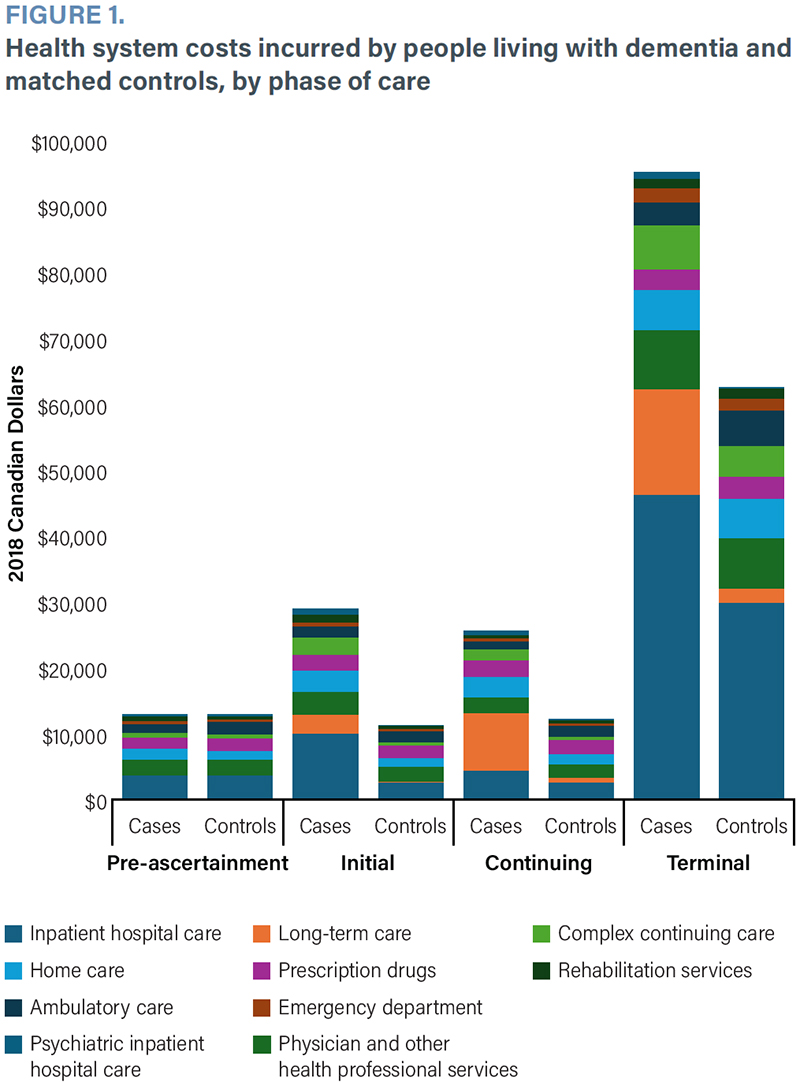
Total mean annual health system costs incurred by people living with dementia were highest in the terminal phase ($95,147), followed by the initial phase ($29,079), continuing phase ($25,774) and pre-ascertainment phase ($13,041) (Figure 1). Mean net costs of dementia followed a similar pattern (terminal phase net $32,348, initial phase net $17,624 and continuing phase net $13,407). Costs of care during the pre-ascertainment phase were not significantly different between people living with dementia and matched controls. Higher net costs in the dementia group in the continuing and terminal phases were driven predominantly by in-patient hospital care and long-term care.
{kind=link}

Five-year costs
Overall, the mean five-year net costs incurred by people living with dementia totalled $48,077 (Table 2). The mean five-year net costs of dementia were highest for long-term care ($28,655), inpatient hospital care ($7,629), complex continuing care ($4,690) and home care ($4,557). These costs were always higher in people living with dementia (compared with controls), except for ambulatory care ($2,424). Overall, five-year net costs were higher for females ($50,158) than for males ($44,800).
| TABLE 2. Five-year net health system costs incurred by people newly living with dementia | |||
| Sector | Net costs (Mean 2018 $ CDN; 95% confidence interval) |
||
| Overall N = 164,640 pairs | Females N = 96,715 pairs | Males N = 67,925 pairs | |
| Total | 48,077 (47,183, 48,970) | 50,158 (49,053, 51,263) | 44,800 (43,323, 46,277) |
| In-patient hospital care | 7,629 (7,180, 8,078) | 6,732 (6,199, 7,265) | 8,831 (8,056, 9,605) |
| Long-term care | 28,655 (28,307, 29,003) | 33,016 (32,530, 33,502) | 22,318 (21,850, 22,787) |
| Physicians and other health professional services | 686 (608, 763) | 704 (609, 799) | 653 (524, 782) |
| Home care | 4,557 (4,387, 4,727) | 4,278 (4,048, 4,507) | 4,913 (4,663, 5,164) |
| Prescription drugs | 1,507 (1,379, 1,635) | 1,823 (1,676, 1,970) | 1,051 (823, 1,279) |
| Complex continuing care | 4,690 (4,340, 5,039) | 3,673 (3,254, 4,091) | 6,094 (5,494, 6,693) |
| Ambulatory care | -2,424 (-2,611, -2,237) | -2,007 (-2,225, -1,788) | -3,004 (-3,332, -2,676) |
| Emergency department | 225 (204, 246) | 199 (172, 226) | 260 (226, 293) |
| Rehabilitation services | 555 (454, 655) | 361 (236, 487) | 825 (659, 990) |
| Psychiatric inpatient hospital care | 1,997 (1,800, 2,193) | 1,379 (1,175, 1,583) | 2,860 (2,487, 3,232) |
Significance and Solutions
Over time, health system costs of dementia are considerable in Ontario, particularly in the later phases of care, where in-patient hospitalization and long-term care home admission are common. Our cost estimates differed somewhat from international research, which has shown that cost differences are greatest in the first year after diagnosis, whereas our longitudinal study shows the highest costs in the terminal phase (Coe et al. 2023; Persson et al. 2022; Phelan et al. 2012). These findings suggest that upstream investments in home care and other services that support individuals in the community may provide a better quality of life and be cost-saving from the health system perspective. For example, adult day programs offer promise, but the factors ensuring their success are not yet clear (Nguyen et al. 2024). We also found that women incur higher net costs, which may indicate that they require specific support to meet their needs.
In the future, emerging innovations in new biomarkers and drug therapies have the potential to change care pathways and health system utilization significantly for the growing population of Canadians living with dementia (Smith et al. 2025; Turner et al. 2020). However, our publicly funded and provincially administered health systems currently struggle in their ability to provide timely and equitable access to existing services for people living with dementia. It is unclear whether the Canadian healthcare system is adequately resourced to provide quality care according to current models, let alone the more intensive care that might be needed with new innovations. Improving the quality of dementia care is critical to preventing unnecessary disability and improving quality of life. Evaluating and comparing the quality of dementia care across – and within – provinces over time is a necessary first step toward improving equitable and efficient care at a population level.
Conclusion
Understanding the health system contributors to costs of care is beneficial for ensuring optimal use of health system resources throughout dementia progression and for future health system planning.
Funding and Support
This research was conducted with support from the Ontario Neurodegenerative Disease Research Initiative (ONDRI) through the Ontario Brain Institute, an independent non-profit corporation, funded partially by the Ontario Government. This study was also supported by ICES, which is funded by an annual grant from the Ontario Ministries of Health and Long-Term Care. Parts of this material are based on data and/or information compiled and provided by the Ontario Ministry of Health, Canadian Institute for Health Information and Ontario Health. This document also uses data adapted from the Statistics Canada Postal CodeOM Conversion File, which is based on data licensed from Canada Post Corporation and/or data adapted from the Ontario Ministry of Health Postal Code Conversion File. We thank IQVIA Solutions Canada Inc. for the use of their Drug Information File. The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
About the Author(s)
Susan E. Bronskill, Phd, is a senior core scientist and program leader at ICES in Toronto, ON, and a professor at the Institute of Health Policy, Management and Evaluation (IHPME), University of Toronto. She can be reached by e-mail at susan.bronskill@ices.on.ca.
Laura C. Maclagan, MSc, is an associate research methodologist at ICES in Toronto, ON.
Luke Mondor, MSc, is a staff scientist at ICES in Toronto, ON.
Longdi Fu, MSc, is a senior research analyst at ICES in Toronto, ON.
Jun Guan, MSc, is a research methodologist at ICES in Toronto, ON.
Isabella J. Sewell, BSc, is a master's student in psychology at York University, Toronto, ON.
Andrea Iaboni, MD, DPhil, is a geriatric psychiatrist and scientist at KITE Research Institute in Toronto, ON, and an associate professor of psychiatry at the University of Toronto.
Richard H. Swartz, MD, Phd, is a neurologist and scientist at Sunnybrook Research Institute in Toronto, ON, and an associate professor of neurology at the University of Toronto.
Colleen J. Maxwell, Phd, is a senior adjunct scientist at ICES and a professor in the School of Pharmacy at the University of Waterloo, Waterloo, ON.
Claire de Oliveira, Phd, is a senior health economist at the Centre for Addiction and Mental Health (CAMH) in Toronto, ON, and an associate professor at the IHPME at the University of Toronto.
Acknowledgment
A preliminary version of these findings was presented at the 2021 Alzheimer's Association International Conference and published as a podium abstract.
References
Adlimoghaddam, A., B. Roy and B.C. Albensi. 2018. Future Trends and the Economic Burden of Dementia in Manitoba: Comparison With the Rest of Canada and the World. Neuroepidemiology 51(1-2): 71–81. doi:10.1159/000490414.
Alzheimer Society of Canada. 2025. Dementia Numbers in Canada. Retrieved March 18, 2025. <https://alzheimer.ca/en/about-dementia/what-dementia/dementia-numbers-canada>.
Canadian Institute for Health Information (CIHI). 2018, June 26. Dementia in Canada. Retrieved March 18, 2025. <https://www.cihi.ca/en/dementia-in-canada>.
Chen, S., Z. Cao, A. Nandi, N. Counts, L. Jiao, K. Prettner et al. 2024. The Global Macroeconomic Burden of Alzheimer's Disease and Other Dementias: Estimates and Projections for 152 Countries or Territories. Lancet Global Health 12(9): e1534–43. doi:10.1016/S2214-109X(24)00264-X.
Coe, N.B., L. White, M. Oney, A. Basu and E.B. Larson. 2023. Public Spending on Acute and Long-Term Care for Alzheimer's Disease and Related Dementias. Alzheimer's and Dementia 19(1): 150–57. doi:10.1002/alz.12657.
de Oliveira, C., R. Pataky, K.E. Bremner, J. Rangrej, K.K.W. Chan, W.Y. Cheung et al. 2016. Phase-Specific and Lifetime Costs of Cancer Care in Ontario, Canada. BMC Cancer 16(1): 809. doi:10.1186/s12885-016-2835-7.
Edwards, S., D. Trepel, C. Ritchie, J.H. Hahn-Pedersen, D.E. Robinson, M.S. Chan et al. 2024. Real World Outcomes, Healthcare Utilisation and Costs of Alzheimer's Disease in England. Aging and Health Research 4(1): 100180. doi:10.1016/j.ahr.2024.100180.
Province of Ontario. Personal Health Information Protection Act, 2004, S.O. 2004, c. 3, Sched. A. Retrieved June 12, 2025. <https://www.ontario.ca/laws/statute/04p03>.
Griffith, L.E., A. Gruneir, K. Fisher, D. Panjwani, A. Gafni, C. Patterson et al. 2019. Insights on Multimorbidity and Associated Health Service Use and Costs From Three Population-Based Studies of Older Adults in Ontario With Diabetes, Dementia and Stroke. BMC Health Services Research 19(1): 313. doi:10.1186/s12913-019-4149-3.
Grignon, M. and B.G. Spencer. 2018. The Funding of Long-Term Care in Canada: What Do We Know, What Should We Know? Canadian Journal on Aging 37(2): 110–20. doi:10.1017/S0714980818000028.
Nguyen, H., A. Rahman, A. Ubell, Z. Goodarzi, C.J. Maxwell, S. Allana et al. 2024. Adult Day Programs and Their Effects on Individuals with Dementia and Their Caregivers (ADAPT-DemCare): A Realist Synthesis to Develop Program Theories on the How and Why. Systematic Reviews 13(1): 265. doi:10.1186/s13643-024-02683-1.
Jaakkimainen, R.L., S.E. Bronskill, M.C. Tierney, N. Herrmann, D. Green, J. Young et al. 2016. Identification of Physician-Diagnosed Alzheimer's Disease and Related Dementias in Population-Based Administrative Data: A Validation Study Using Family Physicians' Electronic Medical Records. Journal of Alzheimer's Disease 54(1): 337–49. doi:10.3233/JAD-160105.
Manuel, D.G., R. Garner, P. Finès, C. Bancej, W. Flanagan, K. Tu et al. 2016. Alzheimer's and Other Dementias in Canada, 2011 to 2031: A Microsimulation Population Health Modeling (POHEM) Study of Projected Prevalence, Health Burden, Health Services, and Caregiving Use. Population Health Metrics 14(1): 37. doi:10.1186/s12963-016-0107-z.
Marasco, R.A. 2020. Current and Evolving Treatment Strategies for the Alzheimer Disease Continuum. The American Journal of Managed Care 26(8 Suppl): S167–76. doi:10.37765/ajmc.2020.88481.
Persson, S., S. Saha, U.G. Gerdtham, H. Toresson, D. Trépel and J. Jarl. 2022. Healthcare Costs of Dementia Diseases Before, During and After Diagnosis: Longitudinal Analysis of 17 Years of Swedish Register Data. Alzheimer's and Dementia 18: 2560–69. doi:10.1002/alz.12619.
Phelan, E.A., S. Borson, L. Grothaus, S. Balch and E.B. Larson. 2012. Association of Incident Dementia With Hospitalizations. JAMA 307(2): 165–72. doi:10.1001/jama.2011.1964.
Smith, E.E., N.A. Phillips, H.H. Feldman, M. Borrie, A. Ganesh, A. Henri-Bhargava et al. 2025. Use of Lecanemab and Donanemab in the Canadian Healthcare System: Evidence, Challenges, and Areas for Future Research. The Journal of Prevention of Alzheimer's Disease 12(3): 100068. doi:10.1016/j.tjpad.2025.100068.
Tonelli, M., N. Wiebe, Y. Joanette, B.R. Hemmelgarn, H. So, S. Straus et al. 2022. Age, Multimorbidity and Dementia With Health Care Costs in Older People in Alberta: A Population-Based Retrospective Cohort Study. CMAJ Open 10(3): E577–88. doi:10.9778/cmajo.20210035.
Turner, R.S., T. Stubbs, D.A. Davies and B.C. Albensi. 2020. Potential New Approaches for Diagnosis of Alzheimer's Disease and Related Dementias. Frontiers in Neurology 11: 496. doi:10.3389/fneur.2020.00496.
Wodchis, W.P., K. Bushmeneva, M. Nikitovicand and I. McKillop. 2013. Guidelines on Person-Level Costing Using Administrative Databases in Ontario. Health System Performance Research Network: Working Paper Series Vol. 1. Retrieved March 24, 2025. <https://utoronto.scholaris.ca/items/4996f4f6-389a-4973-9aff-0153f31144f4>.
Zilling, J., U.-G. Gerdtham, J. Jarl, S. Saha and S. Persson. 2025. The Formal Care Costs of Dementia: A Longitudinal Study Using Swedish Register Data. The European Journal of Health Economics 26: 353–61. doi:10.1007/s10198-024-01707-w.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed