
Healthcare Quarterly
Beyond the Pandemic Surge: Building a Resilient System for Adolescent and Young Adult Eating Disorder Care
Alene Toulany, Kathryn Trottier, Darryl Yates, Jeff Mainland and Paul Kurdyak
Abstract
Eating disorders are serious, complex conditions that place a significant burden on health systems, individuals and families. Even before the COVID-19 pandemic, hospitalizations for eating disorders in Ontario were rising and characterized by longer hospital stays, greater medical complexity and increasing admissions among young male adults. Using linked ICES data, our work shows that the pandemic was associated with a disproportionate increase in these existing trends, with emergency department visits and hospitalizations among adolescents rising well above expected levels and remaining elevated through 2023; in contrast, young adult rates have largely returned to baseline. These patterns highlight the unique vulnerabilities of adolescents. We discuss the ongoing challenges of limited workforce capacity, long wait times and fragmented services, and propose solutions informed by Ontario Health's Eating Disorders quality standard. Coordinated, multidisciplinary and measurement-driven approaches, co-designed with patients and caregivers, are essential to build a resilient, equitable system capable of meeting the complex needs of this population.
Introduction
Before the COVID-19 pandemic, pediatric hospitalizations for eating disorders in Ontario were already on the rise. Increases were observed across diagnostic groups, with particularly sharp growth in admissions for anorexia nervosa, and among male adolescents (Smith et al. 2023). The same study reported longer hospital stays, greater use of nasogastric feeding (from 21.8% in 2002–2005 to 40.8% in 2018–2020) and more frequent involvement of psychiatric services, reflecting rising illness severity. These trends may reflect earlier detection, increased public awareness, evolving clinical practices and improved recognition among historically underdiagnosed groups such as young male adults (Smith et al. 2023). Collectively, they signal a growing burden on constrained in-patient pediatric care and set the stage for the surge in acute presentations observed during the COVID-19 pandemic.
A System Under Sustained Pressure
During the COVID-19 pandemic, these existing trends became more pronounced with higher-than-expected increases in acute care use. In our initial study using linked ICES data, we examined population-level patterns during the first year following the onset of the pandemic. Among children and adolescents, emergency department (ED) visits for eating disorders increased by 66%, while hospitalizations rose by 37%, relative to pre-pandemic trends (Toulany et al. 2022). These findings signaled a sharp surge in acute presentations during the early pandemic period, concentrated among younger populations.
Subsequent work by our team extended the analysis to include both adolescents and adults from March 2020 to August 2022 (Toulany et al. 2023a). Among adolescents aged 10–17 years, ED visits for eating disorders rose by 121% compared with expected levels, while hospital admissions increased by 54%. These increases peaked in late 2021, when ED visits were nearly four times higher than expected and hospital admissions were more than double what was expected. In contrast, young adults (18–26 years) saw only a modest 13% rise in ED visits, and hospitalizations were slightly lower than expected. Older adults experienced little change or declines, highlighting age-based differences in the persistence of demand.
Our most recent study (Toulany et al. 2025) examined new versus pre-existing eating disorder presentations and extended the analysis through September 2023, 3.5 years after the pandemic onset. Among adolescents, ED visits peaked in 2021 at 170% above expected levels for new cases and 238% for pre-existing cases (Figure 1).
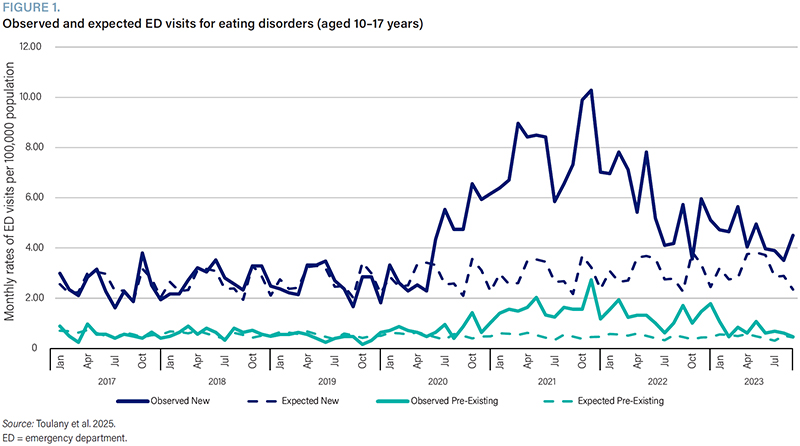{kind=link}

Hospitalizations followed a similar pattern, with peaks of 80% above expected for new cases and more than double for pre-existing cases. Although rates declined from these peaks, adolescent ED visits and hospitalizations in 2023 remained 37% and 53%, respectively, above the expected levels (Figure 2).
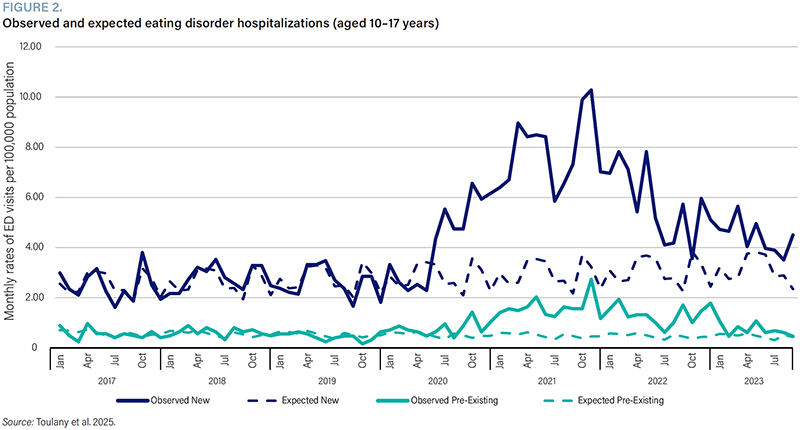{kind=link}

For young adults (18–26 years), the increases were smaller and more transient. ED visits for new cases peaked 21% above expected levels, while ED visits for pre-existing cases rose by 45% during the pandemic. However, hospitalizations among young adults did not rise above expected levels, and by 2023, both ED visits and hospitalizations had returned to or fallen below the baseline.
These findings indicate that although adolescent acute care use has declined from its peak, rates remain elevated above pre-pandemic expectations, with both new and pre-existing cases contributing to this ongoing burden. In contrast, young adult rates have largely returned to those observed before the pandemic. This divergence highlights the unique vulnerabilities of adolescents and highlights the need for continued surveillance to inform system-level responses (Toulany et al. 2025).
Global trends and contributing factors
This pattern is not unique to Ontario. A recent systematic review and meta-analysis (Madigan et al. 2025) synthesized data from 52 studies across 15 countries, encompassing over 148,000 pediatric eating disorder-related visits. The authors reported a 54% overall increase in healthcare use for eating disorders during the COVID-19 pandemic, with larger increases among adolescents compared with children and among young female adults. Significant rises were observed across EDs, in-patient and outpatient settings, with anorexia nervosa showing the most marked increase. The reasons behind this disproportionate rise in adolescent eating disorder presentations are not fully understood, but several hypotheses have emerged. A growing body of evidence indicates that the pandemic and associated public health restrictions contributed to heightened psychological distress in children and adolescents, with documented increases in anxiety, depression, self-harm and suicide attempts (Mitchell et al. 2023; Saunders et al. 2022; Toulany et al. 2023b). Within this broader context, multiple interrelated factors may have elevated the risk for disordered eating in youth. Disruptions to daily structure, social isolation, increased screen time and social media exposure and the loss of in-person supports, such as school-based monitoring and peer networks, are believed to have intensified pre-existing vulnerabilities. Heightened psychological distress, changes in family dynamics and reduced access to early intervention may have further compounded these risks. Moreover, improved caregiver vigilance and awareness may have contributed to increased detection and help-seeking. While causal mechanisms remain uncertain, these associations may help explain the disproportionate increases observed. Continued surveillance and research are needed to clarify these drivers and inform future system responses.
Implications for policy and practice
Ontario's eating disorder care system is under significant strain. Many youth are presenting with cases of greater severity and complexity, including with co-occurring conditions such as anxiety, depression and neurodevelopmental disorders, as well as more severe illness trajectories that make treatment more challenging. One reason for this is inadequate treatment resources, such that individuals need to become “sick enough” to warrant care, which means that illness progresses in severity before intervention. This is not a responsive, system-based approach to meet population-based needs.
These complexities require coordinated, multidisciplinary care, yet current services are often fragmented and under-resourced. Early identification and intervention are critical to preventing illness progression and reducing the need for hospitalization or more intensive levels of care. However, many youth do not receive timely support due to long wait times and limited access to outpatient services. This delay contributes to more severe presentations by the time care is accessed. There is a pressing need for investment in dedicated teams with expertise in adolescent medicine, psychiatry, psychology, social work, dietetics and nursing to work in tandem with primary care and community-based supports. Without a coordinated approach, patients and families face a system that is difficult to navigate, with care that is inconsistent and reactive rather than proactive.
The transition from pediatric to adult care remains one of the most vulnerable periods for youth with eating disorders. Pediatric and adult systems operate under different models of care, and the abrupt shift can leave young people without the support they need at a critical time. It is our responsibility to better prepare adolescents and families for this transition by ensuring continuity of relationships, alignment of treatment approaches and collaborative and coordinated planning between pediatric and adult teams. Solutions may include age-spanning programs (e.g., 16–25 years), transition navigators, flexibility in age of transfer/acceptance and regular joint case conferences to review care plans and risk factors. Such approaches can help reduce relapse, improve engagement and build trust during this developmental stage.
More broadly, Ontario's system is deeply fragmented, with limited accountability or incentive structures to promote collaboration across care settings. However, the early pandemic response demonstrated that system-wide coordination is possible when there is strong leadership and a shared sense of urgency. During the first waves of the COVID-19 pandemic, Ontario Health and the Ministry of Health encouraged institutions and sectors to work together in new ways to address emerging needs. This allowed for a population-based system response and a clear understanding of individual and community health indicators in real time. These efforts led to innovative partnerships and showed that collaboration across institutions can be both feasible and beneficial. Other provinces with regional health authorities offer further examples of system-based care, and Ontario can learn from these models to develop more integrated, regional networks spanning tertiary, community and primary care. Hub-and-spoke models, shared-care agreements and virtual consultations can ensure equitable access to specialized expertise across the province.
The Ontario Health Eating Disorders quality standard provides a comprehensive framework to guide these reforms (Ontario Health 2023). Implementing these nine quality statements will require a renewed commitment to measurement and accountability (Table 1).
| TABLE 1. Ontario Health Eating Disorders quality standards | |
| Comprehensive assessment | Timely physical and mental health evaluations that capture both medical risks and psychological needs. |
| Level of care | Matching patients to the most effective level of care, from outpatient to day treatment or in-patient programs. |
| Transition from youth to adult services | Structured transition planning to ensure continuity during this high-risk period. |
| Psychotherapy | Timely access to evidence-based therapies such as family-based treatment for youth and CBT-ED for adults. |
| Monitoring and medical stabilization | Ongoing medical monitoring and rapid stabilization for those at risk of complications. |
| Support for family and caregivers | Actively involving caregivers in treatment planning, with education and resources to support them. |
| Management of comorbidities | Integrating care for mental and physical health conditions that frequently co-occur with eating disorders. |
| Promoting equity | Ensuring that care is accessible, inclusive and trauma-informed, with attention to rurality, gender, cultural and socio-economic barriers. |
| Care for individuals not in active treatment | Offering regular follow-up and pathways for re-engagement, even when patients are not currently receiving therapy. |
| CBT-ED = cognitive behavioural therapy for eating disorders. | |
Quality indicators, including timeliness of assessments, readmission rates and patient-reported experiences, should be used to track performance and drive improvement. However, measurement must remain focused on outcomes that matter most to patients and families. Linked health administrative data, such as ICES datasets, can be leveraged alongside patient-reported measures to provide a comprehensive view of system performance.
Finally, the voices of patients and caregivers must be at the centre of these reforms. Lived experience offers invaluable insight into the challenges of navigating care, the emotional toll of illness and the gaps that are most in need of change. Establishing youth and caregiver advisory panels across regional networks and embedding co-design principles into program planning and evaluation will ensure that services are both relevant and responsive.
Looking ahead, it remains unclear whether the elevated rates of adolescent eating disorder presentations represent a sustained shift in population-level risk or a transient surge driven by pandemic-related factors. Ongoing surveillance will be essential to monitor trends and anticipate future system needs. To better predict service demands, health systems could leverage forecasting tools, such as predictive analytics and machine learning, informed by linked administrative and patient-reported data. These models could help identify high-risk populations and geographic areas, supporting more responsive and equitable resource planning across the province.
Conclusion
The disproportionate increase in eating disorder presentations during the pandemic highlighted both the resilience and the shortcomings of Ontario's current system of care. While hospital-based programs and multidisciplinary teams have played a vital role in stabilizing young people during acute episodes, these services were not designed to manage the sustained volume, complexity and transition challenges that are now common. Adolescents, especially those moving from pediatric to adult care, remain particularly vulnerable, with persistent gaps in continuity and support. Moving forward, the path to a more responsive and resilient system will require investments in workforce development, improved integration across tertiary, community and primary care and implementation of the Ontario Healths' Eating Disorders quality standard as a unifying framework. The pandemic showed that coordination across institutions is not only possible but also highly effective when aligned under common goals. Ontario can build on this momentum to establish more connected regional systems of care, supported by shared-care models and virtual consultation networks. In addition, developing publicly funded, evidence-informed residential treatment options would address a longstanding gap in the continuum of care for youth with severe illness. By prioritizing timely assessment and access to evidence-based interventions, coordinated transitions and family involvement, while focusing on outcomes that matter the most to patients and caregivers, Ontario can move from a reactive to a proactive model of care. Continued surveillance and robust data measurement, combined with the voices of youth and families at every level of planning and evaluation, will be essential to building sustainable, equitable eating disorder services for the future.
About the Author(s)
Alene Toulany, MD, MSc, is an adolescent medicine specialist at the Hospital for Sick Children (SickKids) and an adjunct scientist at ICES in Toronto, ON. She can be reached by e-mail at alene.toulany@sickkids.ca.
Kathryn Trottier, Phd, CPsych, is a psychologist at the University Health Network and a provincial clinical lead, Eating Disorders, at Ontario Health (Mental Health and Addictions Centre of Excellence) in Toronto, ON.
Darryl Yates, RN, BScN, MHSc, is the executive director, Brain and Mental Health Services, at the Hospital for Sick Children (SickKids) in Toronto, ON.
Jeff Mainland, BSc, MBA, is the executive vice-president at the Hospital for Sick Children (SickKids) in Toronto, ON.
Paul Kurdyak, MD, Phd, is the vice-president, Clinical, at Ontario Health (Mental Health and Addictions Centre of Excellence) and a scientist and lead in mental health and addictions research at ICES in Toronto, ON.
References
Madigan, S., T. Vaillancourt, G. Dimitropoulos, S. Premji, S.M. Kahlert, K. Zumwalt et al. 2025. A Systematic Review and Meta-Analysis: Child and Adolescent Healthcare Utilization for Eating Disorders During the COVID-19 Pandemic. Journal of the American Academy of Child and Adolescent Psychiatry 64(2): 158–71. doi:10.1016/j.jaac.2024.02.009.
Mitchell, R.H.B., A. Toulany, H. Chung, E. Cohen, L. Fu, R. Strauss et al. 2023. Self-Harm Among Youth During the First 28 Months of the COVID-19 Pandemic in Ontario, Canada: A Population-Based Study. CMAJ 195(36): E1210–20. doi:10.1503/cmaj.230127.
Ontario Health. 2023. Eating Disorders: Care for People of All Ages. Retrieved August 19, 2025. <https://www.hqontario.ca/Portals/0/documents/evidence/quality-standards/qs-eating-disorders-quality-standard-en.pdf>.
Saunders, N.R., P. Kurdyak, T.A. Stukel, R. Strauss, L. Fu, J. Guan et al. 2022. Utilization of Physician-Based Mental Health Care Services Among Children and Adolescents Before and During the COVID-19 Pandemic in Ontario, Canada. JAMA Pediatrics 176(4): e216298. doi:10.1001/jamapediatrics.2021.6298.
Smith, S., A. Charach, T. To, A. Toulany, K. Fung and N. Saunders. 2023. Pediatric Patients Hospitalized With Eating Disorders in Ontario, Canada, Over Time. JAMA Network Open 6(12): e2346012. doi:10.1001/jamanetworkopen.2023.46012.
Toulany, A., P. Kurdyak, A. Guttmann, T.A. Stukel, L. Fu, R. Strauss et al. 2022. Acute Care Visits for Eating Disorders Among Children and Adolescents After the Onset of the COVID-19 Pandemic. Journal of Adolescent Health 70(1): 42–47. doi:10.1016/j.jadohealth.2021.09.025.
Toulany, A., N.R. Saunders, P. Kurdyak, R. Strauss, L. Fu, N. Joh-Carnella et al. 2023a. Acute Presentations of Eating Disorders Among Adolescents and Adults Before and During the COVID-19 Pandemic in Ontario, Canada. CMAJ 195(38): E1291–99. doi:10.1503/cmaj.221318.
Toulany, A., S. Vigod, P. Kurdyak, T.A. Stukel, R. Strauss, L. Fu et al. 2023b. New and Continuing Physician-Based Outpatient Mental Health Care Among Children and Adolescents During the COVID-19 Pandemic in Ontario, Canada: A Population-Based Study. Frontiers in Psychiatry 14: 1063203. doi:10.3389/fpsyt.2023.1063203.
Toulany, A., A. Babujee, H. Lu, N. Joh-Carnella, T.A. Stukel, A. Guttmann et al. 2025. Long-Term Trends in New and Pre-Existing Eating Disorder Acute Presentations Among Adolescents and Young Adults During and After the COVID-19 Pandemic: A Population-Based Cohort Study. Journal of Adolescent Health 77(4): 756–65. doi:10.1016/j.jadohealth.2025.06.012.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed