
Healthcare Quarterly
An Evaluation of Patient Safety Leadership Walkarounds
Rosanne Zimmerman, Ivan Ip, Charlotte Daniels, Teresa Smith and Jill Shaver
Abstract
Patient safety leadership walkarounds (PSLWA) have been identified as an effective tool to improve patient safety culture. At Hamilton Health Sciences, after one year of monthly PSLWA in all clinical and service programs, 1,351 patient safety issues were identified, of which 64-80% have been resolved or have active improvement work in progress. Five hundred staff were invited to complete a process evaluation regarding the effectiveness of the current process of PSLWA.
A total of 341 surveys were returned (68%). The overall evaluation demonstrated satisfaction with the process of PSLWA; 93% of those surveyed reported that they felt comfortable openly and honestly discussing patient safety issues and had an enhanced awareness of patient safety. Five areas of opportunity for process improvement were identified: scheduling, scripts, feedback, reporting and resolving issues deferred for an organization approach.
PSLWA have offered an effective way to engage leadership and staff in open discussions about patient safety and collaborative approaches for solutions suggesting an enhanced patient safety culture.
The patient safety movement is striving to develop a culture of safety whereby each individual, whether on the receiving or delivery end of care, is preoccupied with safety, is armed with the skills to evaluate his or her environment for potential harm, and is supported and rewarded for making appropriate choices" (Frankel et al. 2003: 16). Patient safety leadership walkarounds (PSLWA) have been identified in the literature as a powerful tool to develop patient safety culture by connecting senior leaders and front-line staff in open dialogues about patient safety (Leonard et al. 2004). Additionally, this strategy promotes teamwork, opens communication channels and offers an opportunity for teams to engage in working together to improve patient safety.
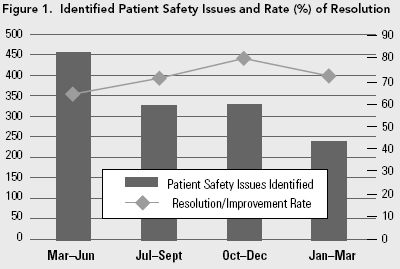

At Hamilton Health Sciences (HHS), PSLWA were initiated in March of 2006, in conjunction with other initiatives to address patient safety culture. HHS is a four-site, 1,000-bed regional tertiary care facility that is composed of five hospitals and a cancer centre. PSLWA offered a unique way to address the challenges of developing patient safety culture in a large organization of 10,000 staff spread over four sites. In the first year of implementation, 984 walkarounds were scheduled. During these PSLWA, 1,351 patient safety issues were identified (Table 1), of which 64-80% were resolved or have active improvement work in progress (Figure 1). The identified patient safety issues were categorized using Vincent's (2006) themes (Figure 2). Following the first year of implementation of this strategy, a process evaluation was completed regarding the current process of PSLWA at HHS.

PSLWA at HHS
There are different processes described in the literature for conducting PSLWA. HHS has adapted the original WalkRounds framework created by Dr. Alan Frankel (Frankel et al. 2003) at Brigham and Women's Hospital in Boston. Although the majority of literature related to PSLWA suggests the application to clinical or clinical support areas, at HHS, PSLWA are conducted in all clinical and service areas in alignment with our philosophy that patient safety is the responsibility of everyone at HHS. PSLWA occur each month in every clinical unit or service area and are led by the manager in the absence of the director or senior team. The director attends PSLWA in all areas of accountability once per quarter, and senior team members attend walkarounds monthly in rotating areas. A central shared access scheduling drive is provided to allow for ease of scheduling multiple leaders. Scripted themed questions are provided to the leaders each quarter to facilitate leading the PSLWA and are to be posted prior to the walkaround for staff. Accountability for resolution of patient safety issues occurs at the unit or area leadership level for most issues and is delegated up for program- or organizational-level issues. Quarterly reports of patient safety issues and the corresponding action plans are summarized by the managers in a computer database. As well, these unit- or area-level reports are then summarized into program reports, which are submitted by the directors to the Patient Safety Team for collation into an organizational report. This report is presented quarterly to the Patient Safety Steering Team.
Recognizing that communication of response to issue identification is a critical success factor for the sustainability of this initiative, all levels of the organization are responsible to provide feedback to staff of action taken on the issues for their relevant level. Formal training for all of the leadership team was provided initially and is ongoing.
Evaluation Method and Demographics of Respondents
In March of 2007, 500 staff (including the leadership team and five front-line members from each unit or area) were asked to complete a survey to evaluate the PSLWA process. Each area was asked to include one staff member who had not yet taken part in PSLWA, if possible. The survey tool consisted of demographic questions, 15 four-point scale questions and four open-ended questions related to the process. In addition, leaders were asked to complete an additional 10 questions related to their role in PSLWA. All surveys were submitted to the Patient Safety Team for analysis. Of a possible 500 responses, 341 were received from 26 programs, which represented a return rate of 68%. Front-line staff comprised 57% of the respondents, and the remaining 43% were formal and informal leaders. Clinical areas represented 71% of the responses, and service areas 28%. A total of 11% of respondents had never attended a walkaround, 56% had attended between one and five PSLWA and the remaining 33% had attended more than five PSLWA.
Results and Next Steps
Strengths
The overall evaluation demonstrated satisfaction with the process of PSLWA and identified some minor improvement opportunities. Some of the strengths identified in the process included the following: 93% of respondents agreed that the PSLWA had enhanced awareness of patient safety issues and that they felt comfortable openly and honestly discussing patient safety issues; 70% of respondents felt they were always heard at PSLWA; and 91% of leaders felt comfortable leading PSLWA (96% clinical, 86% service). Five areas of the process were identified as opportunities for improvement. These areas for improvement were brought to a stakeholder team for discussion and to provide input into resolutions.
Opportunity 1: Scheduling
Consistent with known and ongoing workload issues, 48% of respondents indicated that attendance at PSLWA was difficult or somewhat difficult. Front-line staff reported this more frequently (49%) than leaders (46%), and clinical staff more frequently (54%) than service staff (34%). The stakeholder group further elaborated that general workloads, competing priorities and time of day were contributors to this difficulty. To improve this part of the process, leaders have been encouraged to schedule PSLWA up to a year in advance in the shared schedule and to consider workload patterns for front-line staff in choosing the time of day to conduct PSLWA.
Opportunity 2: Scripting
The scripted questions were reported to be easy to answer (93%) and most of the time led to discussions about patient safety (91%). As well, 66% of PSLWA were reported to take 45 minutes or less. Some of the narrative comments in the survey suggested that there was room to improve transferability and relevance of questions to all areas and to shorten the number of questions to ensure more timely completion of PSLWA.
To address this concern, the scripts were decreased to a standardized format of four questions. The first question is an organizationally generated question to prompt dialogue about a current initiative, work or safety concern that has contextual and temporal relevance at a corporate level. The second question is an open-ended question asking what patient safety issues staff have observed in the past week. The third question allows the unit to choose a question that was specifically relevant to their area or unit in the time frame when it was being asked. To facilitate the selection of a third question, a dictionary of over 100 themed questions was developed from the patient safety literature and from a stakeholder group. This dictionary allows each area the flexibility to customize a relevant discussion to their current issues. The final question asks each participant how they will contribute to resolving the issues discussed at the PSLWA. This is meant to continue to engage all participants to work as a team to solve patient safety issues.
A second issue identified related to scripting was that 40% of respondents indicated that pre-posting of the scripted questions to allow front-line staff time to consider and prepare for the walkaround did not occur. Upon further investigation of this with the stakeholder group, it was found that managers were unaware of the need to post questions or had competing priorities. This requirement of the process has been re-communicated at multiple forums as well as the suggestion to delegate this role.
Opportunity 3: Feedback
Despite the expectation that all levels of the organization would provide feedback of their relevant improvement work related to identified issues, 32% of respondents felt that feedback was below or somewhat below expectations. Clinical areas (30%) reported this less frequently than service areas (39%). To facilitate this feedback, the script introduction now includes a section in which the manager will communicate the ongoing resolution or work in progress related to the identified issues of the previous walkaround at the beginning of the current one. As well, all program directors and the Patient Safety Team are responsible quarterly to report program and organizational level work being done related to patient safety. Respondents also suggested that feedback should be given in multiple forms of media, such as newsletters, bulletin board postings, staff meetings, e-mails and program meetings.
Opportunity 4: Reporting
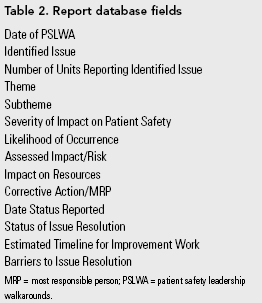
Currently, quarterly reports are in an Excel-based database format with multiple fields of drop-down boxes (Table 2). The time required to complete the quarterly report was noted by the majority of respondents to be less than one hour (82%); however, a large number of respondents (45%) indicated the need for an easier reporting template to use. Several revisions and changes have already been made to the reporting template including a self-generating risk matrix of severity and likelihood that assigns patient safety risk and standardized sub-themes. A stakeholder group has provided some recommendations to be considered for further revisions, and work is in progress to improve the ease of use of the current report.
Opportunity 5: Accountability for Issues Requiring an Organizational Approach
The final area identified for improvement was the need for a clear process and accountability for the resolution of issues that have been deferred from programs because they require an organizational approach. Patient safety issues referred to the organization for resolution are now presented to the director group, which will determine an action plan for resolution and provide a report of progress to the Patient Safety Steering Team.
Conclusion
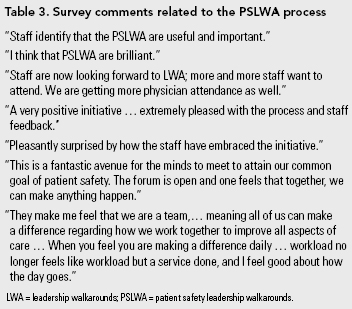
The purpose of PSLWA is to encourage open dialogue about patient safety issues and to enhance patient safety culture. The initial process evaluation of PSLWA has proven this to be a beneficial strategy that may suggest an enhanced patient safety culture. Respondents clearly reported an increased awareness of patient safety issues, and there was an expression of a level of comfort in openly and honestly discussing them. The overwhelmingly positive feedback to the process is reflected in the many narrative comments in the survey (Table 3).
After the first year of PSLWA, we continue to refine and improve the process to ensure a sustainable and valued process. We continue to address the challenges related to the creation of a robust reporting and feedback system. As well, changes related to the script, scheduling and accountability for issues related to organizational processes are ongoing. Senior leadership support has been key in the success and sustainability of this initiative.
Our next step includes assessing the impact to patient safety culture through a patient safety culture survey. As the Health and Safety Commission stated, "Organizations with a positive patient safety culture are characterized by communications founded on mutual trust, by shared perceptions of the importance of safety, and by confidence in the efficacy of preventative measures" (Vincent 2006). PSLWA have offered an effective way to engage leadership and staff in open discussions about patient safety and collaborative approaches for solutions.
About the Author(s)
Rosanne Zimmerman, RN, BHScN, MEd, is a patient safety specialist at Hamilton Health Sciences (HHS), in Hamilton, Ontario. She can be reached at 905-521-2100, ext. 42106, or by e-mail at zimmeros@hhsc.ca.
Ivan Ip, RN, BN, CHE, MBA, PhD (C), is the senior consultant for Quality, Patient Safety and Clinical Resource Management at HHS.
Charlotte Daniels, RN, BScN, MScT, is the integrated vice-president of Patient Services at HHS.
Teresa Smith, RRT, BSc, MBA, is the assistant vice-president of Quality, Patient Safety and Clinical Resource Management at HHS.
Jill Shaver, RD, BSc, MBA, MSOD, is the former assistant vice-president of Organizational Effectiveness at HHS.
References
Frankel, A., E. Graydon-Baker, C. Neppi, T. Simmonds, M. Gustafson and T. Gandhi. 2003. "Patient Safety Leadership WalkRounds™." Joint Commission Journal of Quality and Safety 29(1): 16-26.
Leonard, M., A. Frankel and T. Simmonds. 2004. Achieving Safe and Reliable Healthcare: Strategies and Solutions. Boston: Institute for Healthcare Improvement and the American Organization of Nurse Executives.
Vincent, C. 2006. Patient Safety. UK Health and Safety Commission.Toronto: Elsevier.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed