
Healthcare Quarterly
Health Indicators 2009: A Focus on Cardiac Care in Canada
Yana Gurevich, Tina LeMay, Dragos Daniel Capan and Jeremy Herring
Abstract
Close to 18,000 Canadians die each year after having had a heart attack. Heart attacks are costly to the system: ischemic heart disease (including heart attacks) cost the Canadian healthcare system $8.1 billion in 2000. The Canadian Institute for Health Information's recently released Health Indicators 2009 includes new information relating to heart attacks. This article highlights some of the key findings from the report related to cardiac care. It examines the declining rates of for heart attacks, socio-economic factors relating to heart attacks, falling 30-day in-hospital mortality rates and trends and provincial differences in cardiac procedures.
Importance of Measuring Heart Attacks and Procedures
Heart attack, also known as acute myocardial infarction (AMI), is one of the leading causes of death in Canada (Statistics Canada 2009). About 18,000 people die each year due to this condition (Statistics Canada 2004), making it a major concern for Canadians. Heart attacks are a result of a sudden blockage (usually caused by a buildup of plaques – fat and other materials) to the coronary arteries that supply blood to the heart. Heart attacks may not only result in death but also cause other health problems that are sometimes preventable (Heart and Stroke Foundation 2003). They are costly to the individual and the health system. Based on a recent report by the Public Health Agency of Canada (PHAC), ischemic heart disease including heart attacks cost the health system $8.1 billion in 2000 (PHAC 2009). There are many efforts to help reduce the number of heart attacks in Canada, including the development of prevention programs, the promotion and adoption of healthier lifestyles and the advancement of research on cardiac disease.
A 2009 report (Health Indicators 2009) by the Canadian Institute for Health Information (CIHI), in collaboration with Statistics Canada, provides new information relating to heart attacks. For the first time, it shows rates of admissions to acute care hospitals for new heart attacks. This statistic is more refined than hospitalization rates, which include those people who went into hospital two or more times for the same heart attack or who were transferred to another hospital and were counted more than once. The report also provides information on pan-Canadian angioplasty and bypass surgery rates, the 30-day AMI in-hospital death rate and the rate of unplanned readmissions following discharge from hospital for a heart attack. This article highlights some of the key findings from the report.
| Defining Heart Attack Indicators |
|
All indicators (except mortality rate) are per 100,000 Canadians aged 20 years or older. New hospitalized heart attack event rate: The age-standardized rate of a first-ever acute care hospitalization for a heart attack or recurrent hospitalized heart attack occurring more than 28 days after admission for the previous event in the reference period. Percutaneous coronary intervention (PCI) rate: The age-standardized rate of PCI (or angioplasty) performed in acute care hospitals, same-day surgery facilities or catheterization laboratories. Coronary artery bypass graft (CABG) surgery rate: The age-standardized rate of bypass surgery (CABG) performed in acute care hospitals. 30-day acute myocardial infarction (AMI) in-hospital mortality rate: The risk-adjusted rate (for age, sex and select co-morbid conditions) of in-hospital deaths for any reason occurring within 30 days of first admission to an acute care hospital with a diagnosis of a heart attack. |
Rates of Hospitalized Heart Attacks Declining
In Canada, the rates of hospitalized heart attacks declined significantly over the past several years. More specifically, the rate decreased by 13% between 2003–2004 and 2007–2008 (Figure 1). The decrease was about the same for both men and women; however, the rate of heart attacks was higher for men than women in all age groups.
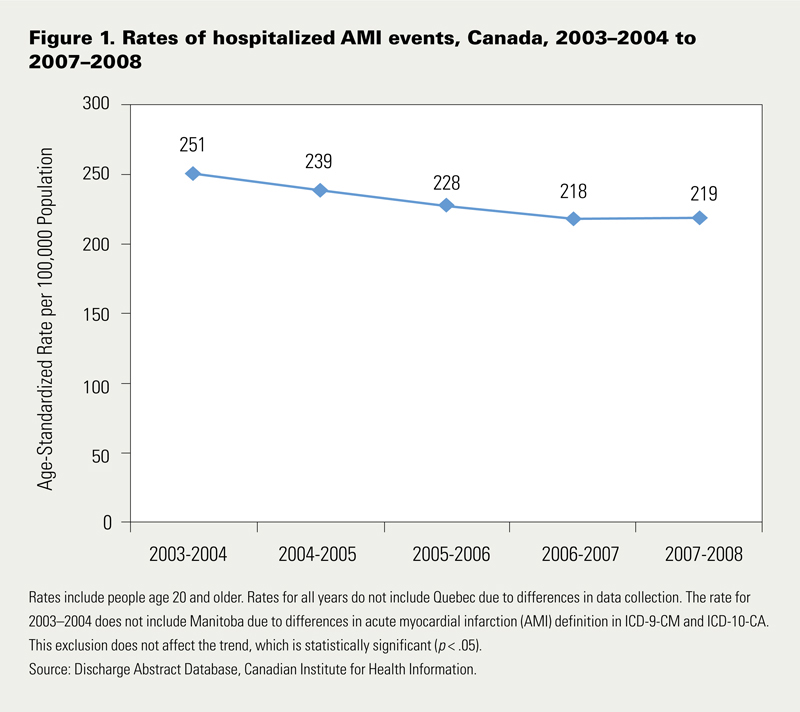
The decline in rates of heart attacks may be a result of better care of Canadians who may be at risk of heart attack (e.g., those with high blood pressure), healthier diets and increased physical activity alongside reduced rates of smoking (PHAC 2009). However, research indicates that this decline in rates of heart attacks may change as the rates of obesity, diabetes and hypertension rise (Lee et al. 2009). Also, it has been suggested that although rates of heart attacks have fallen, there may be a rise in the number of heart attacks in older Canadians, making them possibly more difficult to treat (Tu et al. 2009).
Improvements in, and Gaps between, Heart Attack Rates and Socio-economic Status
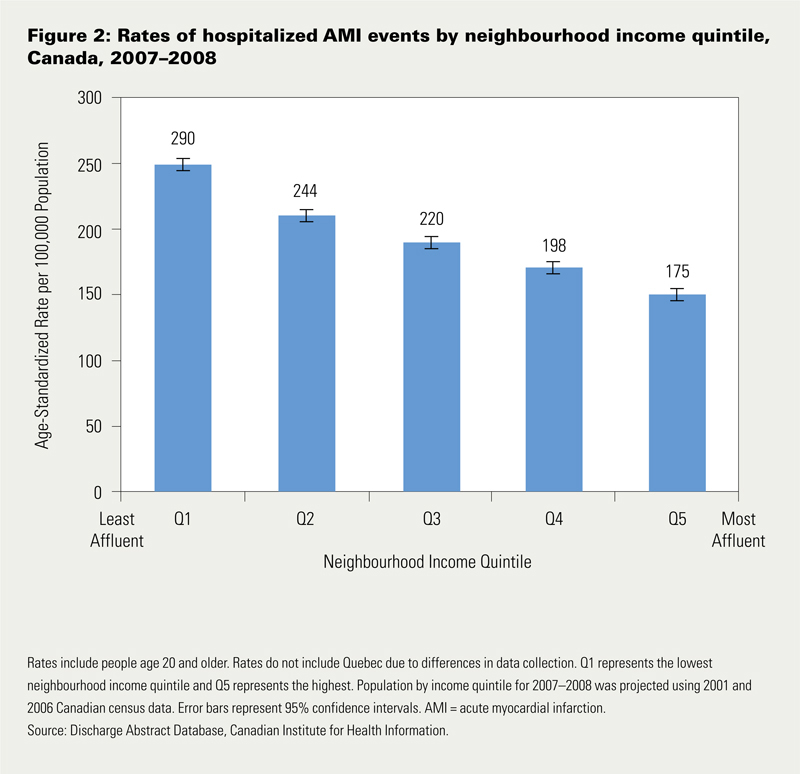
The likelihood of having a heart attack is inversely associated with socio-economic status and the gaps between the socio-economic groups are increasing. Trends show a significant decline in new hospitalized heart attack rates for all socio-economic groups. However, the decrease was greater for those who lived in the most affluent neighbourhoods (–17%) compared with those in the least affluent neighbourhoods (–10%) during the five-year study period.
Also, the gap between these income groups is significant: heart attack rates were two thirds higher for those in the least affluent neighbourhoods compared with those in the most affluent neighbourhoods in 2007–2008 (Figure 2). Research suggests that those in lower-income groups tend to have higher rate of risk factors that are associated with coronary disease, such as hypertension, diabetes and obesity (Lee et al. 2009).
Outcomes: 30-Day AMI In-Hospital Mortality Rates Falling
Not only is the rate of hospitalized heart attacks down, so is the rate of in-hospital deaths. Over the past five years, the 30-day AMI in-hospital mortality rate decreased by 11%. As well, in-hospital mortality rates fell in all age groups and for both men and women over this time period. However, rates varied across the country. Among the provinces, risk-adjusted rates ranged from a high of 11.3% to a low of 7.8%, based on three years (2005–2006 to 2007–2008) of pooled data. To compare, the risk-adjusted rate for Canada over this time period, not including Quebec, was 9.4%.
The drop in in-hospital deaths following heart attacks may be due to adherence to expert guidelines and best practices (Krumholz et al. 2008), breakthroughs in treatments – particularly the timing of re-opening coronary arteries for blood flow (Bavry et al. 2006; Labinaz et al. 2006; Heart and Stroke Foundation et al. 1996) – and a quicker response in performing revascularization procedures. CIHI analyses show that patients with heart attacks are receiving revascularization procedures (by angioplasty or bypass surgery) sooner than in the past. Among all heart attack patients who received a revascularization procedure in 2007–2008, about 43% had the procedure the same day of the day after they were admitted to hospital compared with 28% in 2003-2004. Also, CIHI data show that patients who received a revascularization procedure within 30 days of hospital admission for a heart attack had lower mortality rates than patients who did not.
Trends and Provincial Differences in Rates of Cardiac Procedures
In the past several years, there has been a shift in the types of treatments performed on patients with heart disease. Until the early 1990s, bypass surgery (i.e., coronary artery bypass graft [CABG]) was the preferred procedure for treating coronary disease. Since that time, angioplasty (i.e., percutaneous coronary intervention [PCI]) has become an increasingly common practice for treating this disease. Angioplasty is a less invasive procedure, and it has evolved over time making the treatment more effective and efficient than in its earlier days, so there is less risk to the patient (Hoffman et al. 2003). Bypass surgery is major heart surgery that requires the opening of the chest. This surgery is typically used if angioplasty is not considered an appropriate treatment.
Between 1998–1999 and 2007–2008, the number of angioplasties more than doubled from 17,000 to 36,000, respectively. However, after adjusting for population aging and growth, the increase was about 68.8% over this time period.
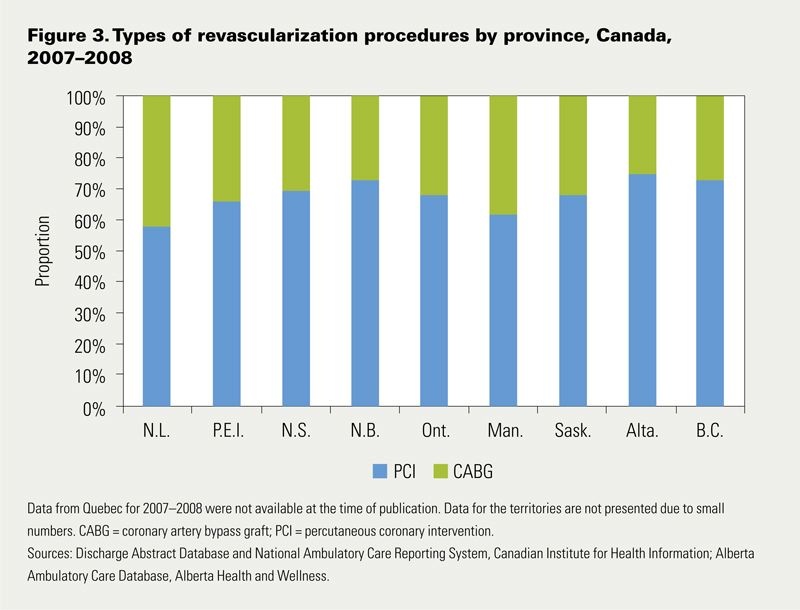
Overall, the cardiac revascularization rate (i.e., the rate of PCI and CABG combined) has increased by 39%, after age and population growth are taken into account. The types of revascularization procedures used vary across the provinces. For example, angioplasty procedures were used most in New Brunswick, Alberta and British Columbia and least in Newfoundland and Labrador, Manitoba and Prince Edward Island (Figure 3). These differences may be due to the population health needs or practice patterns within a given geographical area.
Conclusion
Observed improvements in the rates of heart attacks and 30-day AMI in-hospital mortality suggest that past efforts in prevention, diagnosis and treatment have been successful. Nevertheless, heart disease remains one of the leading causes of death, and continued efforts are still required to prevent this disease and reduce the risk of heart attacks in Canada.
About the Author(s)
Yana Gurevich, MD, MPH, is a methodologist for the Health Indicators team at the Canadian Institute for Health Information (CIHI), Toronto, ON. Prior to working with CIHI, Yana worked as a health services researcher in various governmental settings.
Tina LeMay, BA, BComm, is a program lead for the Health Reports team at CIHI, Toronto, ON. Prior to joining CIHI, Tina was a management consultant at PricewaterhouseCoopers Consulting, providing consulting services for the government and health sectors.
Dragos Daniel Capan, MStat, BSApMath, is a senior analyst for the Health Indicators team at CIHI, Toronto, ON.
Jeremy Herring, MSc, is a senior analyst for the Health Indicators team at CIHI, Toronto, ON.
References
Bavry, A.A., D.J. Kumbhani, A.N. Rassi, D.L. Bhatt and A.T. Askari. 2006. "Benefit of Early Invasive Therapy in Acute Coronary Syndromes: A Meta-Analysis of Contemporary Randomized Clinical Trials." Journal of the American College of Cardiology 48(7): 1319–25.
Canadian Institute for Health Information. 2009. Health Indicators 2009. Ottawa, ON: Author.
Heart and Stroke Foundation of Canada. 2003. The Growing Burden of Heart Disease and Stroke in Canada 2003. Ottawa, ON: Author.
Heart and Stroke Foundation of Canada, Canadian Cardiovascular Society and Canadian Association of Emergency Physicians for the Emergency Cardiac Care Coalition. 1996. "Recommendations for Ensuring Early Thrombolytic Therapy for Acute Myocardial Infarction." Canadian Medical Association Journal 154(4): 483–87.
Hoffman, S.N., J.A. TenBrook Jr., M.P. Wolf, S.G. Pauker, D.N. Salem and J.B. Wong. 2003. "A Meta-Analysis of Randomized Controlled Trials Comparing Coronary Artery Bypass Graft with Percutaneous Transluminal Coronary Angioplasty: One- to Eight-Year Outcomes." Journal of the American College of Cardiology 41(8): 1293–304.
Krumholz, H.M., B.L. Bachelder, S.D. Fihn, P.M. Ho, F.A. Masoudi, E. DeLong, D.C. Goff Jr., L.A. Green and M.J. Radford. 2008. "ACC/AHA 2008 Performance Measures for Adults with ST-Elevation and Non–ST-Elevation Myocardial Infarction: A Report of the American College of Cardiology/American Heart Association Task Force on Performance Measures." Circulation 118(24): 2596–648.
Labinaz, M., T. Swabey, R. Watson, M. Natarajan, W. Fucile, B. Lubelsky, B. Sawadsky, E. Cohen and K. Glasgow (for the CCN Consensus Panel on Access to Urgent PCI for ST Segment Elevation Myocardial Infarction). 2006. "Delivery of Primary Percutaneous Coronary Intervention for the Management of Acute ST-Segment Elevation Myocardial Infarction: Summary of the Cardiac Care Network of Ontario Consensus Report." Canadian Journal of Cardiology 22(3): 243–50.
Lee, D.S., M. Chiu, D.G. Manuel, K. Tu, X. Wang., P.C. Austin, M.Y. Mattern, T.F. Mitiku, L. W. Svenson, W. Putnam, W.M. Flanagan and J.V. Tu.; for the Canadian Cardiovascular Outcomes Research Team. 2009. "Trends in Risk Factors for Cardiovascular Disease in Canada: Temporal, Sociodemographic and Geographic Factors." Canadian Medical Association Journal 181(3–4): E55–66.
Public Health Agency of Canada. 2009. 2009 Tracking Heart Disease and Stroke in Canada. Ottawa, ON: Author.
Statistics Canada. 2004. Mortality, Summary List of Causes 2004. Ottawa, ON: Author.
Statistics Canada. 2009. Leading Causes of Death in Canada. Ottawa, ON: Author.
Tu, J.V., L. Nardi, J. Fang, J. Liu, L. Khalid and H. Johansen; for the Canadian Cardiovascular Outcomes Research Team. 2009. "National Trends in Rates of Death and Hospital Admissions to AMI, Heart Failure and Stroke." Canadian Medical Association Journal 180(13): E118–25.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Note: Please enter a display name. Your email address will not be publically displayed