
Healthcare Quarterly
Using Performance Status to Guide Initiation of Palliative Care Support among Patients with Cancer
The Issue
For patients with cancer, information on their performance status is often used by providers for determining when to initiate or enhance palliative care support (Seow et al. 2011). Information on performance status can also help patients address personal and family matters and focus care on quality of life in an appropriate and timely manner. Since January 1, 2007, the provincial cancer authority in Ontario under the initiative known as the Ontario Cancer Symptom Management Collaborative has systematically collected measures on performance status in cancer outpatients by implementing a standardized validated tool, the Palliative Performance Scale (PPS), in the province's cancer centres (Ho et al. 2008).
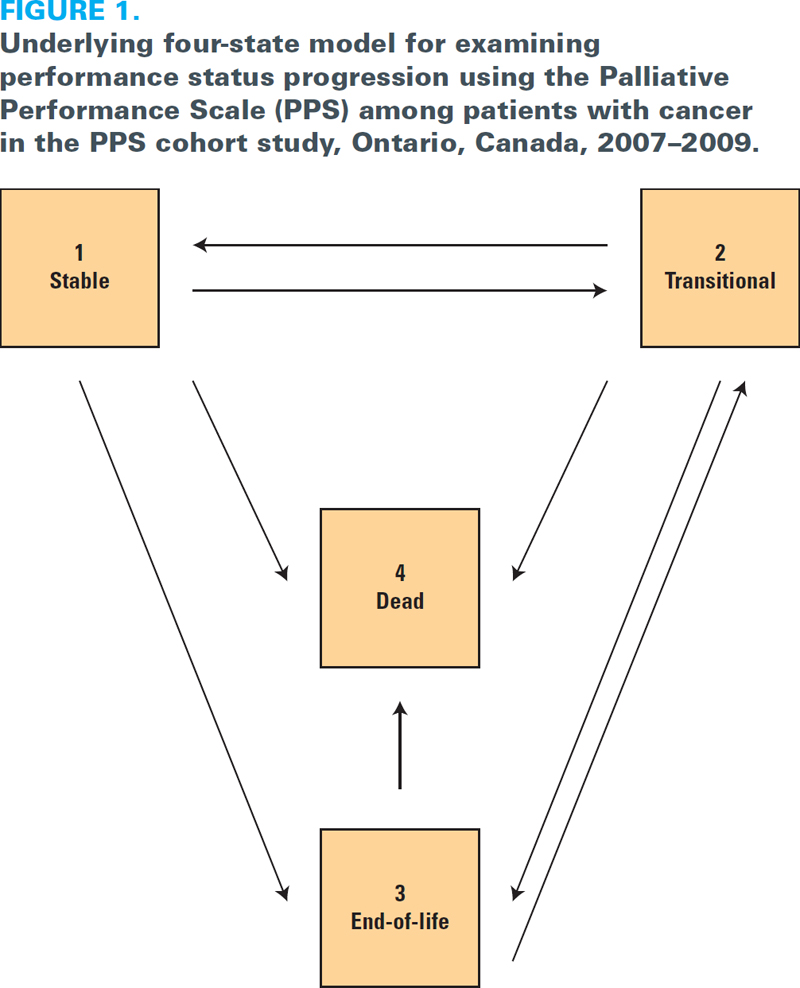
Measured by the physician, the PPS ranges from 10 to 100 (100 = best) in 10-point increments; the measure is based on a patient's level of ambulation, activity level, evidence of disease, ability to perform self-care, nutritional intake and level of consciousness. Three distinct states are used to describe performance status: (1) patients with PPS scores in the range of 70–100 are considered to be in the stable state, (2) patients with scores of 40–60 are considered to be in the transitional state and (3) patients with scores of 10–30 are considered to be in the end-of-life state, at which point, physicians often decide to start discussions regarding palliative care support (Lau et al. 2009). However, is it appropriate to wait until a patient reaches the end-of-life state before initiating palliative care services?
When searching for evidence to address this question, most studies implemented naïve methodological approaches to examine the association between performance status and time to death. For example, several studies used only a single performance status score (measured at an initial assessment) to examine the association with the hazard of death (Lau et al. 2006, 2009). These studies did not account for changes in a patient's performance status over time, and thus could not determine the likelihood of either improvement or deterioration in performance status. Moreover, although patients were assessed only at intermittent clinic visits, previous work did not account for the fact that the exact time at which a patient reached a performance status state was unknown; a patient may have reached that state prior to the time of the clinic visit. Without addressing these substantial limitations, it is difficult to determine whether reaching the end-of-life performance status state is an appropriate trigger for initiating palliative care services.
The Evidence
The overall aim was the longitudinal examination of the progression of performance status to determine the most appropriate point at which to initiate palliative care services. A series of studies at the Institute for Clinical Evaluative Sciences (ICES) was conducted on an Ontario-wide cohort of adult patients diagnosed with cancer after January 1, 2007 (Sutradhar et al. 2011, 2013; Sutradhar and Barbera 2014). A total of 11,342 patients with cancer underwent nearly 71,000 PPS assessments where the median time between assessments was three weeks. A Markov multistate model was implemented to examine the improvement and deterioration in performance status over time, while accounting for intermittent assessments. Figure 1 illustrates the underlying four-state model. The arrows indicate directions in which instantaneous state-to-state transitions are possible. Multistate models are particularly useful for describing the complexities of a disease process, including changes in a patient's health condition over time (Cook et al. 2006). The Markov multistate approach allows one to (1) estimate the probability of transition from one state to another within a specific time period, (2) estimate the average period of a single stay in a state (mean sojourn time) and (3) evaluate factors associated with the rate of each transition.
For the entire cohort under the Markov multistate analysis, a patient in the transitional state has a 24.1% chance of being deceased at the end of one month, whereas a patient in the end-of-life state has a 73.5% chance (Sutradhar et al. 2011). A patient in the end-of-life state has a 20.7% chance of remaining in that state at the end of one month and a 5.7% chance of improvement (implying moving to either the stable state or the transitional state). In general, transitional probabilities are similar between patients with breast or genitourinary cancers and patients with lung or gastrointestinal cancers, and are more favourable for the former than the latter (Sutradhar et al. 2013).
Table 1 provides the estimated mean sojourn time in each state for the entire cohort and for patients diagnosed with lung, breast, gastrointestinal or genitourinary cancer (Sutradhar et al. 2013). For the entire cohort, the average number of months a patient spent in the transitional state before moving to another state was 1.88 months (95% confidence interval [CI]: 1.83–1.94), whereas the average number of months a patient spent in the end-of-life state before moving into another state was 0.63 months (95% CI: 0.56–0.69) or less than three weeks. More drastically, patients with lung or gastrointestinal cancer spent less than two weeks in the end-of-life state. The rate of transition from the end-of-life state to death was 1.79 times higher (95% CI: 1.35–2.32) for males than females, and patients in the highest income quintile were not significantly different from patients in the lower quintiles with respect to the rate of deterioration in performance status (Sutradhar et al. 2013).
| TABLE 1. Estimated mean sojourn time based on PPS scores among patients with cancer in the PPS cohort study, Ontario, Canada, 2007–2009 | ||||||
| Estimated mean sojourn time | ||||||
| Cancer type | Stablea | Transitionalb | End of lifec | |||
| Estimated mean | 95% CI | Estimated mean | 95% CI | Estimated mean | 95% CI | |
| All | 16.74 | 16.35–17.14 | 1.88 | 1.83–1.94 | 0.63 | 0.56–0.69 |
| Lung | 8.74 | 8.42–9.07 | 1.64 | 1.56–1.71 | 0.38 | 0.32–0.45 |
| Breast | 81.46 | 72.84–91.09 | 2.23 | 1.93–2.57 | 1.22 | 0.64–2.34 |
| Gastrointestinal | 15.53 | 14.84–16.25 | 1.65 | 1.56–1.75 | 0.38 | 0.31–0.46 |
| Genitourinary | 25.21 | 22.92–27.72 | 2.05 | 1.81–2.31 | 1.88 | 1.28–2.75 |
| PPS = Palliative Performance Scale. | ||||||
| a = PPS score of 70–100 | ||||||
| b = PPS score of 40–60. | ||||||
| c = PPS score of 10–30. | ||||||
| CI = Confidence interval | ||||||
Implications
The PPS can serve as a tool to guide the timing of palliative care referral. Understanding the probability and direction of change in performance status can contribute to the physician's ability to determine a patient's future needs. Our results indicate that waiting until a patient reaches the end-of-life state may be too late for discussing hospice and/or palliative care options. If ambulatory patients with cancer wait until they reach the end-of-life state to initiate palliative care services, most would not receive palliative care until days before death (Sutradhar et al. 2013). Entry into the transitional state – that is, as soon as a patient receives a PPS score of 60 – may be a more appropriate time to review options for hospice and end-of-life care, as patients with cancer spend sufficient time in this state before experiencing a change in their condition. These implications are in line with results from prior descriptive analyses (Seow et al. 2011).
Because PPS assessments are conducted at clinic visits that occur intermittently throughout a patient's cancer trajectory, the exact time at which a patient reaches the transitional state is not known, making it difficult for clinicians to advise patients in a timely manner. This should motivate providers to decrease the gap between assessments. By doing so, the window of time during which a patient enters the transitional state is narrowed. Assessing performance status with the PPS in a systematic way would allow for prompt identification of a decline in status and the earlier integration of supportive services, which may increase survival and quality of life (Seow et al. 2011). The cohort included in these studies was an ambulatory cancer population, which is representative of what most oncologists encounter in daily clinical practice; this makes our implications generalizable to outpatient cancer centres.
Next Steps
This paper illustrates how longitudinal information on transitions in performance status among cancer outpatients can be used to guide the integration of palliative care services. Our results support the need for recording systematic PPS scores so that progression in performance status can be captured. Providers adhering to this practice can identify patients who have moved into the transitional state, signalling a time for discussion of hospice and palliative care options.
About the Author(s)
Rinku Sutradhar, PhD, is a senior scientist and biostatistician at ICES, and a faculty member in the Department of Biostatistics at the Dalla Lana School of Public Health at the University of Toronto. She may be contacted at rinku.sutradhar@ices.on.ca
References
Cook, R.J. and P. Major. 2006. "Multistate Analysis of Skeletal Events in Patients with Bone Metastases." Clinical Cancer Research 12(20 Pt 2): 6264s–69s.
Ho, F., F. Lau, M.G. Downing and M. Lesperance. 2008. "A Reliability and Validity Study of the Palliative Performance Scale." BMC Palliative Care 7: 10.
Lau, F., M. Downing, M. Lesperance, N. Karlson, C. Kuziemsky and J. Yang. 2009. "Using the Palliative Performance Scale to Provide Meaningful Survival Estimates." Journal of Pain and Symptom Management 38(1): 134–44.
Lau, F., G.M. Downing, M. Lesperance, J. Shaw and C. Kuziemsky. 2006. "Using the Palliative Performance Scale in End-of-Life Prognostication." Journal of Palliative Medicine 9(5): 1066–75.
Seow, H., L. Barbera, R. Sutradhar, D. Howell, D. Dudgeon, C. Atzema et al. 2011. "Trajectory of Performance Status and Symptom Scores for Patients with Cancer during the Last Six Months of Life." Journal of Clinical Oncology 29(9): 1151–58.
Sutradhar, R. and L. Barbera. 2014. "A Markov Multistate Analysis of the Relationship between Performance Status and Death among an Ambulatory Population of Cancer Patients." Palliative Medicine 28(2): 184–90.
Sutradhar, R., L. Barbera, H. Seow, D. Howell, A. Husain and D. Dudgeon. 2011. "Multistate Analysis of Interval-Censored Longitudinal Data: Application to a Cohort Study on Performance Status among Patients Diagnosed with Cancer." American Journal of Epidemiology 173(4): 468–75.
Sutradhar, R., H. Seow, C. Earle, D. Dudgeon, C. Atzema, A. Hussain et al. 2013. "Modeling the Longitudinal Transitions of Performance Status in Cancer Outpatients: Time to Discuss Palliative Care." Journal of Pain and Symptom Management 45(4): 726–34.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed