
Healthcare Quarterly
The South West Local Health Integration Network Behavioural Supports Ontario Experience
Iris Gutmanis, Jennifer Speziale, Lisa Van Bussel, Julie Girard, Loretta Hillier and Kelly Simpson
Abstract
Creating a seamless system of care with improved system and patient outcomes is imperative to the estimated 35,000 older adults living with mental health problems and addictions in the South West Local Health Integration Network. Building on existing investments and those offered through the Behavioural Supports Ontario program, strategies to improve system coordination were put in place, cross-sectoral partnerships were fostered, interdisciplinary teams from across the care continuum were linked, and educational opportunities were promoted. This evolving, co-created system has resulted in a decrease in alternate level of care cases among those with behavioural specialized needs and improved client/family perceptions of care. Also, in fiscal year 2014/15, it provided more than 7,000 care providers with learning opportunities.
Background
Increasing numbers of older adults are living with behavioural and psychological symptoms associated with cognitive impairment due to mental health problems, dementia, addictions and other neurological conditions (Brookmeyer et al. 2007; Mathillas et al. 2011; Smetanin et al. 2009). Referred to as responsive behaviours, behavioural and psychological symptoms can include aggression, disruptive behaviours, disinhibition, apathy, depression, anxiety and agitation (Cerejeira et al. 2012; Patterson et al. 1999; Savva et al. 2009). These behaviours are a means of communication and reflect a response to something in the person's environment (Cohen-Mansfield 2000; Kunik et al. 2010). Responsive behaviours can threaten the safety and well-being of the people experiencing them as well as their care providers (Rodney 2000) and others within the care environment (Rosen et al. 2008). Responsive behaviours are associated with increased care costs (Beeri et al. 2002; Herrmann et al. 2006), increased risk for hospitalization (Toot et al. 2013), early institutionalization (Chan et al. 2003), and mortality (Russ et al. 2012). In response to this growing problem, in 2010, the Ontario government created the Behavioural Supports Ontario (BSO) program, a pan-provincial, regionally implemented quality improvement (QI) initiative that utilizes evidence-informed change strategies and knowledge translation best practices aimed at improving the system of care of older persons experiencing responsive behaviours (Gutmanis et al. 2015).
An estimated 16,904 people in the South West Local Health Integration Network (LHIN) are living with dementia (Hopkins 2010). As well, an estimated 26,077 to 46,019 older adults are living with a mental health problem that could lead to responsive behaviours, dependent on the specific diagnoses (based on prevalence estimates of 17%–30%; Ontario Seniors' Secretariat 2009). To meet service needs, multi-sectoral health service providers came together to co-create a system of care for those living with responsive behaviours. Planning accounted for many factors, including the broad geography of the South West LHIN (size: 21,639 square kilometres), current and future population need and the multiple service provider agencies involved.
This paper outlines the change strategies, executed in stages, that were implemented in the South West LHIN and that led to system redesign. It also describes the impact of those changes both on health system transformation and on those living with responsive behaviours and their family members. Funding was provided by the South West LHIN.
Methods
Health system partners focused on co-creating a system of care that was person-centred, would maximize the skills of staff in a variety of healthcare settings and would provide equitable access to services. St. Joseph's Health Care London was identified as the organization responsible for LHIN-wide BSO coordination. In 2010, a South West LHIN BSO steering committee was struck, comprised of members from many agencies/services to ensure that multi-sectoral, diverse perspectives were at the table. Described below and organized by the three BSO pillars ((1) system coordination and management, (2) intersectoral and interdisciplinary service delivery and (3) knowledgeable care teams and capacity development (Gutmanis et al. 2015); operational and clinical structures were developed, implemented and evaluated to support the BSO system of care.
System Coordination and Management
Many agencies/services were tasked with improving the coordination of services offered across the care continuum, including six Schedule 1 hospitals (i.e., psychiatric facilities designated under the Mental Health Act), 79 long-term care (LTC) homes, six Alzheimer Societies, 10 adult day programs (ADPs) offering overnight respite, St. Joseph's Health Care London (a tertiary-care hospital that offers both specialized geriatric mental health services and specialized geriatric services) and the South West Community Care Access Centre. The development of a common agenda and regional QI plans was facilitated by the BSO operational team (including a project, evaluation and QI lead) and at LHIN and local levels through Kaizen events (Graban and Swartz 2012) that frequently included value stream mapping (Martin and Osterling 2013). Findings informed the South West LHIN BSO action plan (South West Local Health Integration Network 2012). These events assisted with the articulation of a BSO client value statement, vision, mission and values (Table 1).
| Table 1. BSO Vision, Mission and Values |
| BSO Client Value Statement: "I am a unique individual who wants to live my life with dignity." |
| BSO Vision: Enabling older adults to achieve positive emotional and behavioural health and to live with dignity, value and meaning |
| BSO Mission: Through partnership, collaboration, innovation and evidence-informed practice, to build a quality-driven, sustainable behavioural support system of person/family-centred care for older adults living with or at risk of developing responsive behaviours |
BSO Values:
|
To ensure coordinated, system-wide change at a local level, Geriatric Cooperatives were created in five sub-LHIN areas. Co-led by a local hospital director and a community agency lead, representatives from regional mental health services were asked to identify system gaps and develop local work plans that leveraged existing capacity. In addition, Cooperatives were mandated to coordinate, leverage and improve linkages among agencies/services.
In the summer of 2012 and 2015, Geriatric Cooperative members completed the Partnership Self-Assessment Tool (PSAT; https://www.lmgforhealth.org), a standardized tool that identifies effectiveness related to synergy, leadership, efficiency and sufficiency of resources (Lasker et al. 2001; Wiess et al. 2002). In addition, experience-based design (EBD) (Bate and Robert 2006) methodology was used to gather personal stories from individuals with responsive behaviours, their caregivers and staff that described the emotional touch points associated with healthcare journeys. This information was used to identify QI opportunities.
Intersectoral and Interdisciplinary Service Delivery
Multiple strategies were used to ensure interdisciplinary service delivery. One such strategy was the creation and/or enhancement of Geriatric Mental Health Outreach Teams (GMHOTs). Based out of local Schedule 1 hospitals, GMHOT members provide assessment, consultation and short-term follow-up, as well as timely education and support to staff working in LTC homes, hospitals and community organizations, in addition to families and other care partners. GMHOT members come from many disciplines, including recreation therapy, social work and occupational therapy. Teams are led by enhanced psychogeriatric resource consultants (EPRCs), who provide "in the moment," case-based training opportunities, link team members with local services and specialized geriatric psychiatry expertise when more intensive services are needed, and act as a liaison between the EPRC Network and the Geriatric Cooperatives. EPRCs can be from multiple professional backgrounds, including social work and nursing.
Further service enhancements included embedded BSO LTC home staff. Registered nurses, registered practical nurses, and/or personal support workers collaborate with all LTC home staff to improve the care experience of residents and their families and offer staff education regarding responsive behaviours. They are the point of contact within the LTC home for other community-based services and specialized geriatric psychiatry resources. As well, additional social work/social support staff were added to local Alzheimer Societies, and more spaces were funded for ADPs offering overnight respite.
Knowledgeable Care Teams and Capacity Development
Existing provincial resources were leveraged to support the development of LTC home and community service provider QI skills, including the Health Quality Ontario Residents First Initiative (https://www.hqontario.ca/quality-improvement/long-term-care), which provided QI training and coaching within LTC homes. The BETSI tool (Behavioural Supports Ontario 2012a), a framework that helps organizations identify staff readiness and need for education as well as appropriate programs to meet these needs, was administered across all sectors involved with BSO in the South West LHIN. Subsequently, in collaboration with local, regional and provincial experts, the local EPRCs and the BSO operational team coordinated education delivery, providing both in-kind informal coaching and formal teaching. As well, the Capacity Building Roadmap (Behavioural Supports Ontario 2012b), a tool that describes the core competencies required to manage responsive behaviours, was used to develop job descriptions.
The EPRC Network continues to coordinate education initiatives across the LHIN. As well, technology (e.g., Ontario Telemedicine Network, OTN) is used to support clinical and educational activities. HealthChat, an online forum for health professionals to share information, communicate and collaborate (www.healthchat.ca), is used as a central repository for BSO-related information and tools (e.g., assessment and QI tools, protocols, data collection tools) as well as a communication venue for educational opportunities.
Results
System Coordination and Management
EBD (Bate and Robert 2006) data showed that consumers felt that they were "assessed to death," were not sure what was happening with pending referrals to services, were confused by medical jargon, lacked knowledge of available services and supports and how to access them and needed greater access to crisis-oriented services. Communication strategies were implemented that minimized assessment duplication and let clients know when referrals were received and what crisis services were available. These strategies continue to be tweaked using QI methods. As well, plans are in place to train EBD champions across the region.
In 2012, 54 Geriatric Cooperative members (a 64% response rate), and the PSAT findings indicated that the Cooperatives were functioning fairly well in all areas (Gutmanis and Hillier 2012). However, mean scores were in the "work zone" for all dimensions, suggesting that more effort was needed to maximize the partnership's collaborative potential (Table 2). Subsequently, strengths-based Cooperative work plans were generated in an effort to maximize local partnerships.
| TABLE 2. Geriatric Cooperative Evaluation: Partnership Self-Assessment Tool (PSAT) Results by Year | ||
| Dimension | 2012 (N = 54) Mean (range) | 2015 (N = 43) Mean (range) |
| Synergy | 3.5 (3.2–3.7) | 3.4 (3.1–3.7) |
| Leadership | 3.4 (3.0–3.9) | 3.4 (3.3–3.6) |
| Partnership Efficiency | 3.3 (3.1–3.8) | 3.6 (3.5–3.7) |
| Administration and Management Effectiveness | 3.2 (2.7–3.7) | 3.2 (3.1–3.4) |
| Sufficiency of Non-Financial Resources | 3.7 (3.3–3.9) | 3.7 (3.7–3.8) |
| Sufficiency of Financial and Other Capital Resources | 3.8 (3.4–4.0) | 3.7 (3.6–3.9) |
| Benefits Exceeding Drawbacks (% Positive) | 74.1% (69.3%–100%) | 74.5% (55.5%–87.5%) |
| Note: Scores from 1.0 to 2.9 are in the Danger Zone, which means that this area needs a lot of improvement. Scores from 3.0 to 3.9 are in the Work Zone, which means that more effort is needed in this area to maximize the partnership's collaborative potential. Scores from 4.0 to 4.5 are in the Headway Zone, which means that although the partnership is doing pretty well in this area, it has the potential to progress even further. Scores from 4.6 to 5.0 are in the Target Zone, which means that the partnership currently excels in this area and needs to focus attention on maintaining its high score. | ||
When the tool was re-administered in 2015 (Gutmanis and Hillier 2015), only 43 members (a 38% response rate) completed the survey. However, similar results were obtained. Across both administrations, the majority of respondents (>74%) reported that the benefits of Cooperative partnership "exceeded" the drawbacks. The majority of respondents provided ratings of "mostly" or "completely" satisfied (ranging from 63% to 74%) with the way people/organizations worked together, their role in the partnership, plans for achieving goals and the way the partnership implemented its plans (Gutmanis and Hillier 2012; Gutmanis and Hillier 2015). Administration and management effectiveness (e.g., coordinating communication among people/organizations outside of the partnership, providing orientation to new partners) remains an area that needs further work. When asked to identify barriers, respondents indicated that time constraints, high membership turnover and maintaining/improving partner engagement posed challenges.
Qualitative data (i.e., patient and caregiver stories) demonstrate some of the impacts of improved system coordination. One caregiver whose spouse used the overnight respite program on an ongoing basis wrote, "You certainly have relieved a lot of pressure off me, because being the caregiver 24/7 was extremely hard on me."
Client impacts were also observed. For example, one LTC home was struggling to find the best approach with a resident who was refusing to take his medications and was experiencing suicidal ideation. In collaboration with the local Community Stroke Rehabilitation team, the GMHOT was able to gain a better understanding of the resident's personal situation and adapt the approach to care used by the LTC home staff. One of the LTC home staff said,
One month after we started this initiative, we saw a completely different individual!…While it may take a lot of effort on our part, our home has learned to really listen to what the resident is trying to tell you.
Intersectoral and Interdisciplinary Service Delivery
As predicted, need continues to increase. The number of clients served by the BSO program has increased from 2,294 in the third quarter of 2013/14 to almost 3,560 in the fourth quarter of 2014/15. More than 6% of the population aged 65 or older are now being seen through BSO.
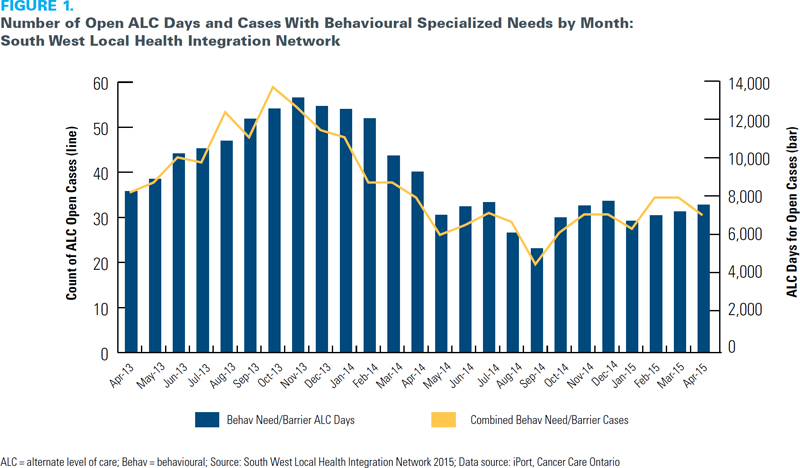
Both system and individual-level impacts have been noted. Between October 2013 and April 2015 there were fewer open alternate level of care (ALC) cases among those with behavioural specialized needs in the South West LHIN, as well as fewer ALC days (South West Local Health Integration Network 2015). As seen in Figure 1, the number of open ALC cases among those with behavioural specialized needs has varied from a high of 58 in October 2013 to a low of 24 in September 2014. From November 2013 to April 2014, the number fell from 55 cases to 36 cases (average: 49.8 cases). Over the same six-month period in 2014/15, the mean number of open ALC cases was 36% lower (mean: 31.8 cases). A similar decrease in the number of ALC days for open cases is observed between November 2013 and April 2014, with a similar levelling off between November 2014 and April 2015.
Qualitative data further demonstrate the impact of interdisciplinary care on clients and their families. A LTC home resident who had exhibited inappropriate behaviour toward other residents was referred to a local hospital for assessment and recommendations. As reported by the LTC home;
The BSO staff, inpatient mental health team, hospital psychiatrist, LTC home Director of Care and Alzheimer Society met together with [Resident]'s family to review his history, challenges and possible treatment approaches. [Resident] was successfully returned to his LTC home within a week of admission to the hospital … Other residents' safety has increased. No incident reports have been recorded since the client's return to the facility and no responsive behaviours have been exhibited….There was no one individual more responsible for [Resident]'s care than another. The team was truly interdisciplinary in its approach to client-centred care.
Knowledgeable Care Teams and Capacity Development
Opportunities for capacity development have increased. In 2012/2013, at the onset of the BSO initiative, 34 education events/presentations related to the care of those with responsive behaviours were scheduled. This increased to 325 in 2013/2014, and then to 410 in 2014/2015. In 2013/14, more than 1,100 people attended these events. This number increased dramatically in 2014/15, to 7,025 people.
Demonstrating effective outcomes, one caregiver wrote to the then Ontario Minister of Health and Long-Term Care, Deb Matthews, and related the story of her husband who had frontotemporal dementia. Amongst several comments about the high quality of care he received, she wrote of the LTC home in which her husband was living, "All of the services are provided by well trained, caring and cheerful professionals, who make every possible effort to ensure those under their care feel secure, comfortable and content."
Discussion
With the implementation of BSO, system coordination has improved and cross-sectoral communication has been enhanced. Partnerships facilitated by the Geriatric Cooperatives have changed the way agencies/services collaborate. As evidenced by client and family stories, interdisciplinary service delivery has improved client perceptions of care and increased the time clients spend in the right place, accessing the right services. The observed reduction in ALC days, though likely attributable to the combined efforts of several LHIN-wide initiatives, suggests improved client flow. And, when services are provided by well trained, qualified staff, clients feel safe.
Lessons Learned
Broad system change is not without its challenges and risks.
- Developing a common language proved more difficult and confusing than expected (e.g., some mobile teams were called behavioural response teams while others were called BSO outreach teams, confusing some referral sources).
- Sustainability has been challenging, particularly in regard to staff recruitment and retention, ensuring capacity development in light of staff turnover and maintaining partner engagement, as recently evidenced by some flagging engagement in the Geriatric Cooperatives. Static funding can potentially result in staffing erosion, as hospitals, LTC homes and community services will not be able to compensate for the anticipated rise in program and salary costs.
- Measuring BSO impacts/outcomes has been challenging, as there is currently no valid method of accessing BSO-specific data from existing large databases. Process and QI measures continue to be collected and used to understand system evolution.
Although these factors may be considered barriers, they also serve as opportunities for creative problem-solving; these issues are frequent agenda items at BSO meetings at provincial, regional and local levels.
Although in place for several years, this new way of working together requires nurturing, and, as evidenced by the PSAT results, more effort is needed to maximize collaborative efforts. Moving forward, with stable, appropriate, and consistent membership, the Cooperatives will likely be in a better position to excel in all areas of their partnership.
BSO has been a catalyst for change. It builds on existing local and system resources and strengths and provides an approach to capacity and care model development that has the potential for replication in other jurisdictions seeking sustainable system change. A renewed culture of QI and a fully developed healthcare force that keeps asking, "How can we make this better?" will result in a system of care that can adapt and rectify future service gaps.
Next Steps
As BSO evolves, ongoing local and system change will focus on continuing support to primary care, the establishment of behavioural support units and alignment with existing provincial and local addictions, dementia, and HealthLink strategies (https://www.health.gov.on.ca/en/pro/programs/transformation/com_healthlinks.aspx). Additional investments to build on OTN technology and other mobile devices and electronic patient systems across the South West LHIN will further support clinical and educational initiatives.
Recently, a provincial operations team and BSO secretariat were created with the aim of linking BSO initiatives across Ontario to promote best practices in assessment, capacity development and measurement. The "Ontario Best Practice Exchange & Beyond" event was held on September 25, 2015. In his concluding remarks, Dr. Ken LeClair (Queen's University, Professor and Chair, Division of Geriatric Psychiatry) supported the philosophy of moving forward together for better health and healthcare for older persons with responsive behaviours, mental health and addictions, dementia, and families and caregivers. By honouring people, honouring partners and honouring possibilities, person- and family-centred care is and will continue to be the foundation on which we build a better system of care for those living with responsive behaviours.
About the Author(s)
Iris Gutmanis, PhD is an associate scientist with the Lawson Health Research Institute; an Assistant Professor with the Department of Epidemiology and Biostatistics, Schulich School of Medicine and Dentistry, Western University; and Director of Research and Evaluation, Specialized Geriatric Services, St. Joseph's Health Care London, in London, Ontario.
Jennifer Speziale, RN, MPH, is the director of Mental Health Specialty Programs, St. Joseph's Health Care London, in London, Ontario. For more information, please contact Ms. Speziale by email at: Jennifer.Speziale@sjhc.london.on.ca.
Lisa Van Bussel, BSc. MD, FRCPC, is a geriatric psychiatrist in the Regional Psychogeriatric Program and Physician Leader for the Geriatric Psychiatry Program, St. Joseph's Health Care London, and an Associate Professor in the Department of Psychiatry, Schulich School of Medicine and Dentistry, Western University, in London, Ontario.
Julie Girard, BA, MA, is the team lead for System Design and Integration, South West Local Health Integration Network, in London, Ontario.
Loretta Hillier, MA, is a research associate with Specialized Geriatric Services, St. Joseph's Health Care London, in London, Ontario.
Kelly Simpson, MA, was the project lead for Behavioural Supports Ontario, St. Joseph's Health Care London, in London, Ontario.
Acknowledgment
The authors wish to thank the South West Local Health Integration Network and the Ontario Ministry of Health and Long-Term Care for their ongoing support for Behavioural Supports Ontario, individuals and committees that have provided leadership support for this initiative, and people (healthcare providers, front-line workers, leaders, managers) across health sectors and services, all of whose dedication to Behavioural Supports Ontario reflects their ongoing commitment to improve the quality of life of persons with responsive behaviours and their care partners. As well, we thank individuals with responsive behaviours and their care partners who have shared their lived experiences, allowing front-line workers and care providers to identify gaps in services and test opportunities for improving the quality of care in this region.
References
Bate, P. and G. Robert. 2006. "Experience-Based Design: From Redesigning the System Around the Patient to Co-designing Services with the Patient." Quality and Safety in Health Care 15: 307–10. doi:10.1136/qshc.2005.016527
Beeri, M.S., P. Werner, M. Davidson and S. Noy. 2002. "The Cost of Behavioral and Psychological Symptoms of Dementia (BPSD) in Community Dwelling Alzheimer's Disease Patients." International Journal of Geriatric Psychiatry 17(5): 403–08. doi:10.1002/gps.490
Behavioural Supports Ontario. 2012a. "Behavioural Education and Training Supports Inventory (BETSI)." Toronto, ON: Author. Retrieved July 8, 2015. <http://brainxchange.ca/Public/Resource-Centre-Topics-A-to-Z/Behavioural-Education-and-Training-Supports-Invent.aspx>.
Behavioural Supports Ontario. 2012b. Capacity Building Roadmap. Toronto, ON: Author. Retrieved July 8, 2015. <http://brainxchange.ca/Public/Files/BSO-Resources/BSO-capacity-building-roadmap.aspx>.
Brookmeyer, R., E. Johnson, K. Ziegler-Graham and H.M. Arrighi. 2007. "Forecasting the Global Burden of Alzheimer's Disease." Alzheimer's and Dementia 3: 186–91. doi:10.1016/j.jalz.2007.04.381
Cerejeira, J., L. Lagarto and E.B. Mukaetova-Ladinska. 2012. "Behavioural and Psychological Symptoms of Dementia." Frontiers in Neurology 3: 73. doi:10.3389/fneur.2012.00073
Chan, D.C., J.D. Kasper, B.S. Black and P.V. Rabins. 2003. "Presence of Behavioral and Psychological Symptoms Predicts Nursing Home Placement in Community-Dwelling Elders With Cognitive Impairment in Univariate but Not Multivariate Analysis." Journal of Gerontology Series A, Biological Sciences and Medical Sciences 58(6): 548–54.
Cohen-Mansfield, J. 2000. "Theoretical Frameworks for Behavioral Problems in Dementia." Alzheimer's Care Quarterly 1: 8–21.
Graban, M. and J. Swartz. 2012. Healthcare Kaizen: Engaging Front-line Staff in Sustainable Continuous Improvement. New York, NY: Productivity Press.
Gutmanis, I. and L.M. Hillier. 2012. "Behavioral Support System for Older Persons With Behavioral Challenges: Evaluation of Geriatric Cooperatives in Southwestern Ontario." London, ON: South West Local Health Integration Network.
Gutmanis, I., and L.M. Hillier.2015. "Behavioural Supports Ontario – South West: Elevation of Geriatric Cooperatives in Southwestern Ontario: 2015." London, ON: St. Joesph's Health Care London.
Gutmanis, I., M. Snyder, D. Harvey, L.M. Hillier and J.K. LeClair. 2015. "Health Care Redesign for Responsive Behaviours – the Behavioural Supports Ontario Experience: Lessons Learned and Keys to Success." Canadian Journal of Community Mental Health 34: 45–63. doi:10.7870/cjcmh-2015-001
Herrmann, N., K.L. Lanctot, R. Sambrook, N. Lesnikova, R. Hebert, P. McCracken, A. Robillard and E. Nguyen. 2006. "The Contribution of Neuropsychiatric Symptoms to the Cost of Dementia Care." International Journal of Geriatric Psychiatry 21(10): 972–76. doi:10.1002/gps.1594
Hopkins, R.W. 2010. "Dementia Projections for the Counties, Regional Municipalities and Census Divisions of Ontario. Kingston, ON, PCCC Mental Health Services." Geriatric Psychiatry Program Clinical/Research Bulletin Number 16. 7-7-2015.
Kunik, M.E., A.L. Snow, J.A. Davila, A.B. Steele, V. Balasubramanyam, R.S. Doody, P.E. Schulz, J.S. Kalavar and R.O. Morgan. 2010. "Causes of Aggressive Behavior in Patients With Dementia." Journal of Clinical Psychiatry 71: 1145–52. doi:10.4088/JCP.08m04703oli
Lasker, R.D., E.S. Wiess and R. Miller. 2001. "Partnership Synergy: A Practical Framework for Studying and Strengthening the Collaborative Advantage." Milbank Quarterly 79: 179–205.
Martin, K. and M. Osterling. 2013. Value Stream Mapping: How to Visualize Work and Align Leadership for Organizational Transformation. New York, NY: McGraw Hill.
Mathillas, J., H. Lovheim and Y. Gustafson. 2011. "Increasing Prevalence of Dementia Among Very Old People." Age and Ageing 40: 243–49. doi:10.1093/ageing/afq173
Ontario Seniors' Secretariat. June 3, 2009. Presentation to the Select Commmittee on Mental Health and Addictions.
Patterson, C.J., S. Gauthier, H. Bergman, C.A. Cohen, J.W. Feightner, H. Feldman and D.B. Hogan. 1999. "The Recognition, Assessment, and Management of Dementing Disorders: Conclusions From the Canadian Consensus Conference on Dementia." Canadian Medical Association Journal 160: S1–S15.
Rodney, V. 2000. "Nurse Stress Associated With Aggression in People With Dementia: Its Relationship to Hardiness, Cognitive Appraisal and Coping." Journal of Advanced Nursing 31(1): 172–80.
Rosen, T., K. Pillemer and M. Lachs. 2008. "Resident-to-Resident Aggression in Long-Term Care Facilities: An Understudied Problem." Aggression and Violent Behavior 13: 77–87. doi:10.1016/j.avb2007.12.001
Russ, T.C., G.D. Batty and J.M. Starr. 2012. "Cognitive and Behavioural Predictors of Survival in Alzheimer Disease: Results From a Sample of Treated Patients in a Tertiary-Referral Memory Clinic." International Journal of Geriatric Psychiatry 27(8): 844–53. doi:10.1002/gps.2795
Savva, G.M., J. Zaccai, F.E. Matthews, J.E. Davidson, I. McKeith and C. Brayne. 2009. "Prevalence, Correlates and Course of Behavioural and Psychological Symptoms of Dementia in the Population." British Journal of Psychiatry 194(3): 212–19. doi:10.1192/bjp.bp.108.049619
Smetanin, P., P. Kobak, C. Briante, D. Stiff, G. Sherman and S. Ahmad. 2009. "Rising Tide: The Impact of Dementia in Canada in 2008 to 2038." Toronto, ON, Risk Analytica.
South West Local Health Integration Network. 2012. "Developing a Behavioural Support System for Older Persons With Responsive Behaviours in the South West LHIN Action Plan: Part A." Retreived July 7, 2015. <www.southwestlhin.on.ca/.../SW_ActionPlan%20A%205Apr12%20Final>.
South West Local Health Integration Network. 2015. "South West LHIN Seniors Portfolio Internal Dashboard." London, ON: South West Local Health Integration Network.
Toot, S., M. Devine, A. Akporobaro and M. Orrell. 2013. "Causes of Hospital Admission for People With Dementia: A Systematic Review and Meta-Analysis." Journal of the American Medical Directors Association 14(7): 463–70. doi:10.1016/j.jamda.2013.01.011
Wiess, E.S., R. Miller Anderson and R.D. Lasker. 2002. "Making the Most of Collaboration: Exploring the Relationship Between Partnership Synergy and Partnership Functioning." Health Education and Behavior 29: 683–98. doi:10.1177/109019802237938
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed