
Healthcare Quarterly
Advancing Healthcare Equity Monitoring and Progress: A Framework to Assess Measures for Sensitivity to Inequities
Abstract
Equitable healthcare is needed to improve population health outcomes. However, a lack of comprehensive analytical tools and data impedes efforts to monitor and improve equity in care. Measures often do not include stratified statistics, providing insufficient information about variations in access, quality or outcomes across population subgroups. Measures that are equity-sensitive leverage disaggregated data to detect differences in care among population groups and across institutions, serving as one mechanism toward identifying and tracking healthcare inequities across the care continuum. This report presents a framework to assess measures for equity sensitivity that may be used across diverse settings.
Why Assess Measures for Sensitivity to Inequities?
Improving population health and providing quality and equitable healthcare – whether defined along socio-economic, demographic or geographic lines – are goals for Canada's health systems (Health Quality Ontario n.d.; Ministry of Health 2025; Prime Minister of Canada 2023). However, a lack of comprehensive analytical tools and data remains a major obstacle to improving equity in health services. Reported healthcare measures often focus on “overall” statistics that are not stratified, providing insufficient information about variations in access, quality or outcomes across population subgroups. Many data sources also fail to adequately represent certain marginalized populations, such as racialized minorities and non-binary individuals, further limiting efforts to identify healthcare inequities. Where data permits, disaggregating findings may facilitate the assessment of potentially avoidable differences in healthcare between populations that are more and less advantaged socially.
We refer to any measure that can be disaggregated toward assessing inequities across distinct pre-specified equity-deprived groups as equity-sensitive measures. The term “measure” is used throughout this paper to refer more broadly to any type of quantitative summary of information, including but not limited to metrics and indicators. The identification and development of such measures may facilitate the identification of inequities along the care continuum as they detect differences in care quality among population groups and across institutions, while also providing evidence of action to redress observed disparities. As equity-sensitive measures may help to monitor and reduce inequities, they should be prioritized. This report thus presents a framework for assessing measures for equity sensitivity toward addressing variations in quality along the continuum of healthcare. Related concepts are defined in Box 1 (CIHI 2022).
| BOX 1. Definitions |
| Equity stratifier: A demographic, social, economic or geographic characteristic that can identify population subgroups for the purpose of measuring differences in health and healthcare that may be considered unfair and avoidable. |
| Health inequality: Any measured difference in health and healthcare access, quality or health outcomes between population subgroups. Health inequalities may be due to unavoidable biological and natural factors. |
| Health inequity: A difference in health and healthcare access, quality or outcomes between population subgroups that is unfair and avoidable. |
| Equity-sensitive measure: Any measure that can be disaggregated toward assessing inequities across distinct population groups. A measure may be equity-sensitive for some population groups and not for others if data pertaining to a particular group were captured by a measure and if evidence points to related disparities or inequities and actions to redress observed disparities or inequities. |
Background of the Framework
Prior work aimed at assessing disparity-sensitive measures conducted by the US National Quality Forum (NQF) and the Core Quality Measures Collaborative (CQMC) was reviewed to inform the approach taken for this project. Two reports (CQMC 2022; NQF 2012) released by the NQF and CQMC were particularly consulted to adapt the equity-sensitive measures screening framework discussed in this paper. An additional high-level scan of the academic and grey literature was also conducted to identify additional relevant resources.
The framework outlined below addresses limitations that were identified in the NQF and CQMC reports, such as the use of an arbitrary threshold for the NQF's quality gap measure and the CQMC's limited list of conditions necessary to satisfy its criteria to indicate a measure as inequity sensitive. Key consideration was given to balancing comprehensiveness and simplicity to facilitate use by stakeholders, including those with limited capacity and resources.
The Equity-Sensitive Measures Framework
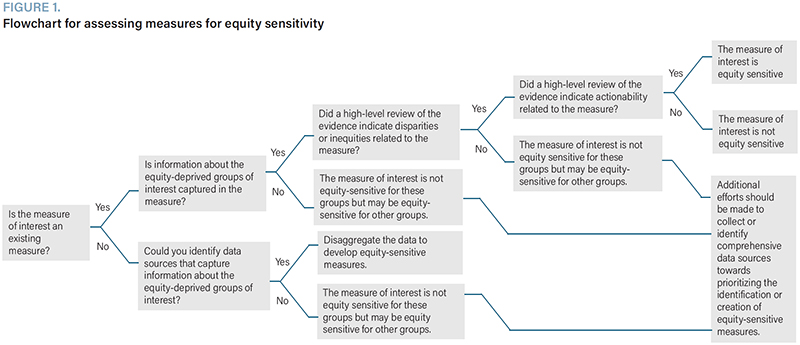
The framework for assessing measures for equity sensitivity (described in Figure 1 and further illustrated in Figure 2) may be used to determine whether healthcare measures are equity sensitive.
{kind=link}
{kind=link}


This approach first considers whether data on pre-specified equity-deprived groups were captured in the measure during its development – an important step toward verifying that inequities may be calculated where present (Figure 1). Particular measures and equity-deprived groups may be selected for evaluation based on existing organizational priorities, preliminary reviews of the literature or consultations with health equity scholars, practitioners and/or advocates.
Next, a high-level scan of available evidence must be conducted to determine whether the measure is associated with disparities or inequities, with additional consideration given to the location of the measure along the care continuum and whether disparities or inequities may potentially exist at other locations further upstream or downstream (Figure 2). For example, if a health outcome measure has been selected and disparities are observed, then consideration should be given to whether these disparities potentially arose due to upstream disparities in social, structural or medical determinants of health, as well as the long-term consequences of such disparities. It is important to note that a lack of disparities or inequities identified in the literature does not denote conclusive evidence that disparities or inequities related to the measure are completely absent. As reported measures often represent cross-sectional summaries of data, it is possible for the information captured to differ before or after its collection, as might occur following the implementation or de-implementation of an intervention. It is also possible for certain population groups that are particularly susceptible to health inequities to be under-investigated due to challenges or biases in data collection due to their relatively smaller population size or reduced likelihood of participation in survey-based research.
Intersectionality (Crenshaw 1989, 1991) – which considers the complex ways in which individuals' unique social positions (like race, sex, gender and disability) interconnect with one another and with related systems of power (like racism, sexism and ableism) to shape opportunity, experiences and outcomes – should also be considered when reviewing the evidence and evaluating nuances in healthcare experiences and related measures. Evaluating such complexities would further support equitable care practice and policy development by highlighting population groups that are at particular risk of care inequities, and who should potentially be prioritized.
The strength of the evidence resulting from the high-level literature scan should also be noted as it relates not only to the volume of evidence but also to the effects reported and related implications. It is important to note that considering the sheer volume of evidence is not sufficient in determining its strength, as a paucity of evidence might indicate under-investigated topics or population groups, and not necessarily a true lack of evidence, as mentioned earlier. Examples of guiding questions to consider when evaluating the strength of evidence include the following: In addition to the volume of the evidence, are reported effect size estimates clinically/practically meaningful? What would be the possible consequences (e.g., clinically, socially or economically) if the measure persisted as is? As this step is more subjective and requires a level of value judgement, a team-based approach with at least two literature reviewers may be preferable. Also, as this is a high-level scan, focus should be placed on reviewing abstracts, with full-text reviews completed only when necessary. Important information about the articles found in this literature review should finally be extracted to allow for the identification of trends across published studies.
If the first two criteria are satisfied (i.e., the measure captures information about the pre-specified equity-deprived group(s), and there is evidence of disparities or inequities associated with the measure topic), then the actionability of the measure should be evaluated through a second high-level evidence review to determine whether reducing observed disparities is feasible. Measures that are amenable to action should be prioritized for monitoring and reporting toward actively reducing observed inequities.
If all three criteria are met, then the measure should be classified as equity sensitive and should be prioritized for equity-informed analysis and reporting. If the first criterion is not satisfied, then the evidence searches may still be conducted to determine whether a particular equity-sensitive measure should be prioritized for future development. A case example of the application of this framework is presented in Table 1.
| TABLE 1. Example of the framework's application using the Canadian Institute for Health Information's ambulatory care-sensitive condition hospitalization indicator | |
| Step in the framework | Case example |
| Select a measure and determine its location along the framework's continuum | The ambulatory care-sensitive condition (ACSC) hospitalization measure was selected. It is located at the “Subsequent Engagement(s) with Health Services” point in the framework. |
| Select equity stratifiers |
|
| Determine whether information on the equity-deprived groups was captured in the measure | Information on sex, gender and rurality was captured in the measure. Information on race, ethnicity and income was not captured in the measure. The indicator is therefore not currently sensitive to ethnoracial and income inequities. The remainder of the assessment included all equity stratifiers to determine whether the ACSC hospitalization measure is equity-sensitive for sex, gender and rurality in its current form, and whether a future version of the measure may be developed to monitor inequities in race, ethnicity and income. |
| Select an academic database for the literature reviews | Several databases exist and may be used to conduct the high-level evidence scan. PubMed was used for this assessment. |
| Develop a search strategy | A search strategy was iteratively developed, resulting in the following: ((“ambulatory care sensitive condition*”[Title/Abstract] OR “ACSC”[Title/Abstract]) AND (“inequit*”[Title/Abstract] OR “equit*”[Title/Abstract] OR “disparit*”[Title/Abstract] OR “equal*”[Title/Abstract] OR “inequal*”[Title/Abstract]) AND (“hospitalization*”[Title/Abstract] OR “hospitalisation*”[Title/Abstract])) AND (fha[Filter]) |
| Conduct the literature search | The advanced search option on the PubMed homepage was used to conduct the search. The abstracts of the resulting studies were extracted from PubMed. |
| Extract equity-specific information | A matrix was created in Excel to extract relevant information from each abstract (e.g., authors, title, journal, year of publication, objective, jurisdiction, specific equity group stratifier, equity results). A new sheet was created for each equity-deprived group within this Excel file and the extracted data was reviewed to identify whether there were ACSC hospitalization inequities relating to sex, gender, rurality, race, ethnicity and/or income. |
| Interpret the results | We identified abundant evidence of ACSC hospitalization disparities/inequities relating to race and ethnicity, rurality and income. As the selected measure is located at the “Subsequent Engagement(s) with Health Services” point in the framework, interpretations should consider how observed disparities or inequities might have been influenced by disparities or inequities in earlier care experiences or through other determinants of health. Less evidence of disparities/inequities relating to sex and gender were found in the evidence search, possibly due to a lack of empirical investigation regarding these groups. |
| Repeat the previous steps to identify whether interventions associated with the measure have been reported and interpret the results | A large body of evidence demonstrates that community- and health centre-based interventions may reduce inequities relating to ACSC hospitalizations. |
| Form conclusions | The ACSC hospitalization indicator is sensitive to inequities relating to rurality and may be further developed to be sensitive to ethnoracial and income inequities, if the necessary data are made available. |
Conclusion
Health equity is a cross-cutting theme and a key component of quality healthcare. This work is thus relevant to all aspects of care provision, including access, quality and outcomes of primary care, acute care and long-term care, among others. The result of this project may be used to identify equity-sensitive measures from an existing suite of measures or to develop novel measures that are equity sensitive, toward facilitating efforts to monitor and address healthcare inequities.
About the Author(s)
Khandideh K.A. Williams, Phd(c), is a fellow at the Canadian Institute for Health Information (CIHI) in Montreal, QC. She can be reached by e-mail at khandideh.williams@mail.mcgill.ca
Josh Fagbemi, MSc, is a program manager at CIHI in Toronto, ON. He can be reached by e-mail at jfagbemi@cihi.ca.
Acknowledgment
We thank members of the Canadian Institute for Health Information's Health Equity and Analytical Information Governance team for their feedback on this paper. Khandideh K. A. Williams was supported by a Health System Impact Fellowship, co-funded by the Canadian Institutes of Health Research (CIHR) and the Canadian Institute for Health Information (CIHI).
References
Canadian Institute for Health Information (CIHI). 2022. Measuring Health Inequalities: A Toolkit – Glossary of Terms. Retrieved August 18, 2025. <https://www.cihi.ca/sites/default/files/document/measuring-health-inequalities-toolkit-glossary-of-terms-en.pdf>.
Core Quality Measures Collaborative (CQMC). 2022, November 14. CQMC Health Equity Final Report. Retrieved August 18, 2025. <https://p4qm.org/sites/default/files/CQMC-Resources/cqmc-health-equity-final-report-2022.pdf>.
Crenshaw, K. 1989. Demarginalizing the Intersection of Race and Sex: A Black Feminist Critique of Antidiscrimination Doctrine, Feminist Theory and Antiracist Politics. University of Chicago Legal Forum 1989: 139–67.
Crenshaw, K. 1991. Mapping the Margins: Intersectionality, Identity Politics, and Violence Against Women of Color. Stanford Law Review 43(6): 1241–99, doi: 10.2307/1229039.
Health Quality Ontario. n.d. Health Quality Ontario's Health Equity Plan. Retrieved 14 July 2025. <https://www.hqontario.ca/Portals/0/documents/health-quality/Health_Equity_Plan_Report_En.pdf>.
Ministry of Health. 2025, January. Closing the Gap: A Measurement Primer to Reduce Population Health Inequities in British Columbia. Retrieved August 18, 2025. <https://www2.gov.bc.ca/assets/gov/health/about-bc-s-health-care-system/public-health/pph-framework/bc_population_and_public_health_closing_the_gap_primer_jan_2025.pdf>.
National Quality Forum. 2012, November 15. Healthcare Disparities and Cultural Competency Consensus Standards: Disparities-Sensitive Measure Assessment. Retrieved July 14, 2025. <https://www.oregon.gov/oha/HPA/ANALYTICS/MeetingDocuments/2018-12-18-NQF-DisparitiesMeasure-Assessment-Final-Report-2012.pdf>.
Prime Minister of Canada. 2023. Working Together to Improve Health Care for Canadians. Retrieved July 14, 2025. <https://www.pm.gc.ca/en/news/news-releases/2023/02/07/working-together-improve-health-care-canadians>.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed