
Healthcare Quarterly
Using Data to Drive Policy Action: An Urgent Call for Funding Interdisciplinary Team-Based Rheumatology Care
Abstract
Canadian healthcare systems face mounting pressures from rising chronic disease prevalence, persistent specialist shortages and escalating healthcare expenditures. Rheumatology exemplifies these challenges, with growing patient demand and a persistently limited rheumatologist workforce caring for patients requiring intensive ongoing specialist care. Population-level data on rheumatology patients demonstrate increasing rheumatic disease prevalence, emergency department utilization, disability and medication expenditures, underscoring the unsustainability of physician-centric care models. Across Canada, there is a broad policy consensus that team-based care is essential to improving access, reducing system pressures and enhancing outcomes for patients with chronic disease. However, team-based models have not been systematically extended to specialty care across jurisdictions. Team-based models of rheumatology care that integrate allied health practitioners in rheumatology practices are essential to improving access, enhancing care quality and optimizing workforce capacity. Leveraging existing interprofessional team funding mechanisms to rheumatology settings represents a pragmatic, evidence-informed policy pathway to modernize specialist care delivery and improve the sustainability of the healthcare system.
Aligning Rheumatology Care With Canada's Health System Priorities
Canadian healthcare systems face immense pressure to reduce emergency department (ED) overcrowding, improve wait times, strengthen health workforce capacity, enhance care coordination and contain rising expenditures in the face of growing populations and rising prevalence of chronic disease. Yet, for many chronic diseases, system performance remains stubbornly stagnant. Rheumatology is a stark example of this challenge. Individuals with rheumatoid arthritis (RA) and other rheumatic and musculoskeletal diseases (RMDs) are among the most intensive consumers of primary, specialty and acute care and medication spending (Barber et al. 2023). Despite this, the rheumatology workforce remains persistently limited, with only 500 clinically active rheumatologists nationally (300 in Ontario) serving a growing, increasingly complex patient population.
From Numbers to Action: Using Data to Drive Change
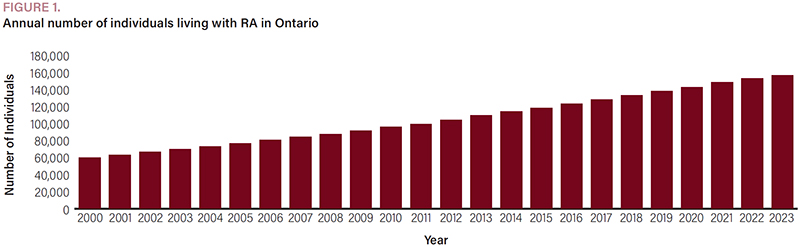
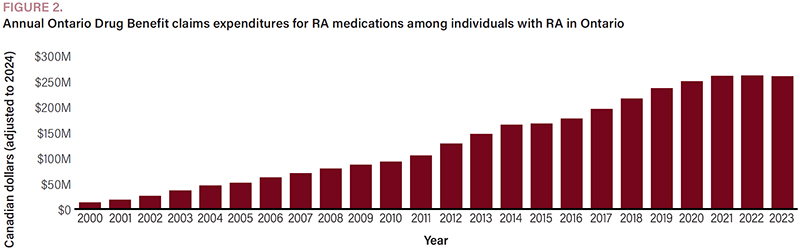
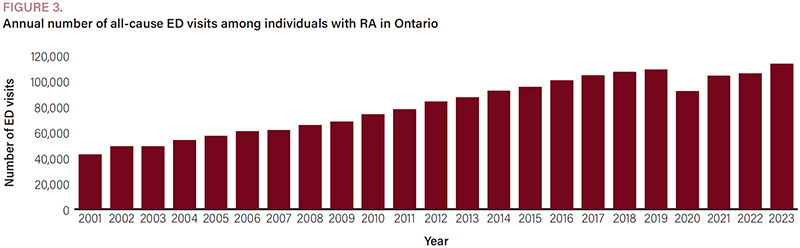
Recent ICES data illustrate the scale of the challenge in Ontario, with RA presented here as a representative example of the impacts imposed by RMDs on Ontario's healthcare system. The number of individuals living with RA in Ontario has more than doubled over two decades (>162,000 as of 2023) (Figure 1). At the same time, RA medication expenditures have surged from $12.6 million (2000) to over $260 million (2023) for public drug funding programs (Figure 2). Furthermore, ED visits among RA patients continue to rise, exceeding 113,000 ED visits in 2023 (Figure 3), reflecting gaps in outpatient care. In addition, nearly one in 11 working-age RA individuals (under 65) are recipients of disability benefits (Widdifield et al. [in press]). These indicators collectively underscore a sobering reality: the current model of rheumatology service delivery (largely based on solo independent rheumatologist practices) is no longer sustainable and does not lead to optimal patient and system-wide outcomes. ICES data have also enhanced our understanding of the rising demand for rheumatology care in the population (Widdifield et al. 2020, 2021). Only 300 practicing rheumatologists (at 140 practice locations) serve approximately 350,000 total patients (>800,000 visits) annually across Ontario (Widdifield et al. 2020, 2025). Without new care models that expand service capacity and more effectively support complex chronic disease management, Canada will remain unable to meet policy targets for reducing avoidable acute care use, improving patient outcomes and containing healthcare costs.
{kind=link}
{kind=link}
{kind=link}



Why Rheumatology Needs a Team-Based Model
RMDs are among the leading causes of pain, disability and reduced employment and quality of life (Hassen et al. 2025; Kirkeskov and Bray 2023). They impose significant economic burdens on individuals and society, driven by high medication costs, productivity losses and increased hospital and ED utilization (Barber et al. 2023). Timely access to rheumatologists is critical: early diagnosis and treatment dramatically improve long-term outcomes, prevent irreversible joint and organ damage and reduce downstream costs (Davtyan et al. 2023; Monti et al. 2015; Widdifield et al. 2016). Yet, timely access to rheumatology care is increasingly unattainable (Widdifield et al. 2017).
Rheumatologists face mounting pressures: escalating caseloads, growing clinical complexity, expanding administrative workload and rising expectations for high-quality care amid increasing multi-morbidity and social determinants of health that require attention. Expanding visit durations is rarely feasible given prolonged waitlists, forcing rheumatologists to make difficult trade-offs balancing comprehensive consultations and preserving access. Burnout among rheumatologists is rising (Kulhawy-Wibe et al. 2022), workforce growth has not kept pace with population growth and rheumatologists cannot increase clinical capacity without sacrificing quality.
Meanwhile, prolonged wait times delay initiation of disease-modifying therapies during the early stages of inflammatory disease, when treatment is most effective in preventing irreversible damage. In the absence of timely specialist care, patients seek interim management in primary care or the ED, where management tends toward short-term symptom control rather than disease modification. Delayed treatment accelerates progression and impairs treatment response, driving further system expenditures. Indeed, diagnostic and treatment delay is the most important modifiable factor negatively impacting outcomes across most RMDs (Nagy et al. 2025). These realities reflect a persistent mismatch between patient needs and system capacity, underscoring the urgency of more effective specialist care models.
Interdisciplinary Team-Based Models of Rheumatology Care: A High-Value, High-Impact Solution
Interdisciplinary team-based models of rheumatology care offer a pragmatic, evidence-informed solution (Bodmer et al. 2026). By integrating interdisciplinary healthcare professionals (IHPs) – extended scope practitioners, physiotherapists, occupational therapists, nurses, pharmacists and other allied health practitioners – into rheumatology clinics, these models extend the reach and efficiency of rheumatology services while enhancing the comprehensiveness of care (King et al. 2026; Sraka et al. 2026).
Such models directly advance Canada's health policy priorities by:
- increasing capacity and shortening wait times, enabling earlier diagnosis and treatment;
- enhancing medication stewardship through therapy optimization, adherence support and monitoring;
- reducing avoidable acute care use through proactive outpatient management;
- improving patient experience and functional outcomes through education, rehabilitation and self-management support;
- advancing health equity for underserved populations;
- enhancing specialist well-being by redistributing care responsibilities; and
- strengthening primary care–specialist integration and care continuity.
These benefits align with provincial commitments to reduce ED pressures, improve chronic disease management and optimize health human resources.
In a 2025 survey, most Ontario rheumatologists agreed that team-based care would be superior to their current practice model, and 91% were motivated to integrate IHPs into their practice – if funding supported the costs of the IHPs (Widdifield et al. 2025).
Key Implementation Barriers: Lack of Sustainable Funding and Capacity Development for Team-Based Care
Despite clear benefits, the primary implementation barrier is the absence of dedicated and sustainable funding for team-based specialty care (Kwok et al. 2025; Widdifield et al. 2025). Rheumatologists lack mechanisms to financially support the integration of IHPs into routine practice. In part, this is because the fee-for-service physician-centric funding model only permits reimbursement for services that physicians perform. Moreover, the infrastructure required to operationalize team-based care, including training and organizational supports needed to support effective team functioning, remains underdeveloped.
The current policy environment presents challenges, as governments across Canada are exercising fiscal restraint and carefully scrutinizing proposals for new investment. Yet, recent commitments to expanding interprofessional primary care teams demonstrate a growing recognition of the value of collaborative care models. This presents a timely and strategic opportunity: positioning rheumatology as a natural extension of primary care modernization.
Leveraging Existing Team Funding Models for Specialty Care
Rheumatology practices share many core features of outpatient primary care, including longitudinal patient relationships, recurring follow-up visits and the need for coordinated management across multiple healthcare professionals. These similarities position rheumatology well for the adaptation of team-based primary care funding approaches that support the integration of IHPs alongside physicians. Rather than replicating comprehensive primary care team funding models in full, a streamlined, specialty-appropriate approach that involves scaled-down elements of Ontario's Family Health Team funding model or, alternatively, alternative payment plans that mirror multidisciplinary clinics of the Ontario Renal Network, for example, could be implemented. Both options offer a feasible and scalable pathway for funding IHPs in outpatient specialty care, without requiring changes to physician reimbursement. By strengthening specialty team capacity, this approach also reduces strains on primary care and strengthens the effectiveness of existing primary care investments.
Team-based rheumatology clinics could:
- shorten time from primary care referral to rheumatology assessment;
- provide rapid access for urgent inflammatory disease assessments;
- offer longitudinal support for patients with chronic, complex diseases;
- reduce primary care and ED visits for uncontrolled pain, disease flares or other complications;
- improve medication optimization and disease monitoring; and
- provide more equitable care tailored to patient needs and address social, functional and psychological needs that drive poor outcomes.
Under the Canadian Institutes of Health Research's Transforming Health with Integrated Care initiative, efforts to guide implementation, spread and scale of interdisciplinary models of rheumatology care across Ontario are underway. This includes developing implementation supports to help rheumatologists transition their practice to a team-based model and ensuring that new funding is used effectively. Without dedicated and stable funding to support the integration of IHPs into rheumatology practices, these models cannot achieve long-term viability.
Conclusion: A Pragmatic Policy Path for High-Impact Reform
ICES data have been instrumental in generating the evidence needed to drive policy change by demonstrating that rheumatology patients account for disproportionately high healthcare utilization and costs – costs that will continue to rise without structural change. Interdisciplinary team-based rheumatology care offers a scalable, high-value workforce solution aligned with current policy priorities. The required investment is modest: rheumatology services represent only a small fraction of overall expenditures incurred by these patients, while therapies alone exceed $10,000 per patient annually. Comprehensive team-based care can optimize therapy use, reduce downstream costs and improve patient and provider well-being.
Expansion of interprofessional teams across Canada presents a timely opportunity. Positioning rheumatology care teams as a natural extension of primary care transformation aligns with a modernization agenda that decision-makers already support. Decision-makers already recognize the value of collaborative, team-based models in improving access, reducing system pressures and improving patient outcomes. Extending this approach to rheumatology represents a politically feasible and economically sound pathway to strengthen specialist care capacity and improve chronic disease management. Without reform, wait times and access pressures will worsen as the burden of RMD grows. Team-based rheumatology care is not simply common-sense reform; it is essential to modernizing care, improving outcomes and ensuring long-term system sustainability.
About the Author(s)
Jessica Widdifield, Phd is a Senior Scientist at ICES, Sunnybrook Research Institute, and Associate Professor at University of Toronto Institute of Health Policy, Management and Evaluation. Jessica can be reached by e-mail at jessica.widdifield@utoronto.ca.
Lauren K. King, MD Phd is an assistant professor in the Division of Rheumatology, Department of Medicine, University of Toronto, and a scientist at Li Ka Shing Research Institute, St. Michael's Hospital.
Celia V. Laur, Phd is a scientist at Women's College Hospital, Office of Spread and Scale, and assistant professor at University of Toronto Institute of Health Policy, Management and Evaluation.
Timothy S.H. Kwok, MD MSc is an assistant professor in the Division of Rheumatology, Department of Medicine, University of Toronto, and associate scientist at Sunnybrook Research Institute.
Jane Purvis, MD FRCPC, is an adjunct professor at Queens University Department of Family Practice.
Philip Baer, MD FRCPC, is Chair of the Ontario Medical Association Section on Rheumatology.
J. Carter Thorne, MD FRCPC, Centre of Arthritis Excellence and The Arthritis Program Research Group Inc, in Newmarket, Canada.
Bindee Kuriya, MD, SM, FRCPC is an assistant professor in the Department of Medicine, University of Toronto; Division of Rheumatology, Sinai Health System and University Health Network.
Vandana Ahluwalia, MD FRCPC, William Osler Health System.
Laura Passalent, PT, BScPT, MHSc, ACPAC, is an assistant professor in the Department of Physical Therapy, Temerty Faculty of Medicine, University of Toronto; and a clinician investigator at Schroeder Arthritis Institute, Krembil Research Institute, University Health Network.
Catherine Hofstetter, Patient Research Partner.
Joanna Yang, MSc, is an analyst at ICES, Toronto, ON.
C. Thomas Appleton MD FRCPC Phd is an associate professor, Department of Medicine, University of Western Ontario.
Acknowledgment
This research was supported by the Canadian Institutes of Health Research (Transforming Health with Integrated Care initiative, IT6-188079), the Institute of Musculoskeletal Health and Arthritis and the Strategy for Patient-Oriented Research. Jessica Widdifield is supported by the Holland Chair in Musculoskeletal Research. Lauren K. King is supported by Arthritis Society Canada. The authors thank the Ontario Rheumatology Association for support and input.
References
Barber, C.E.H., D. Lacaille, R. Croxford, C. Barnabe, D.A. Marshall, M. Abrahamowicz et al. 2023. Investigating Associations Between Access to Rheumatology Care, Treatment, Continuous Care, and Healthcare Utilization and Costs Among Older Individuals With Rheumatoid Arthritis. Journal of Rheumatology 50(5): 617–24. doi:10.3899/jrheum.220729.
Bodmer, N.S., C.V. Laur, J.C. Wong, L.K. King, M.J. Gomes, G.A. Hawker et al. 2026. Team-Based Outpatient Rheumatology Care: A Scoping Review of Terminology, Team Composition, and Impact on Advancing the Quintuple Aim. Journal of Rheumatology 53(4): doi:10.3899/jrheum.2025-0989.
Davtyan, A., J.J.Y. Lee, L. Eder, G.A. Hawker, J. Luo, C.E.H. Barber et al. 2023. The Effects of Continuity of Rheumatology Care on Emergency Department Utilization and Hospitalizations for Individuals With Early Rheumatoid Arthritis: A Population-Based Study. Journal of Rheumatology 50(6): 748–53. doi:10.3899/jrheum.220996.
Hassen, N., K. Moolooghy, J. Kopec, H. Xie, K.M. Khan and D. Lacaille. 2025. Determinants of Health-Related Quality of Life in Adults Living With Rheumatoid Arthritis: A Systematic Review. Seminars in Arthritis and Rheumatism 73: 152717. doi:10.1016/j.semarthrit.2025.152717.
King, L.K., D. To, Z. Ladak, L. Oliva, C. Barnes, C. Hofstetter et al. 2026. Constructing the Program Theory: An Implementation Science Approach to Understanding a Successful Interdisciplinary Team-Based Model of Rheumatology Care. Implementation Science Communications 7: 45. doi:10.1186/s43058-026-00870-w.
Kirkeskov, L. and K. Bray. 2023. Employment of Patients With Rheumatoid Arthritis – A Systematic Review and Meta-Analysis. BMC Rheumatology 7: 41. doi:10.1186/s41927-023-00365-4.
Kulhawy-Wibe, S.C., J. Widdifield, J.J.Y. Lee, J.C. Thorne, E.A. Yacyshyn, M. Batthish et al. 2022. Results From the 2020 Canadian Rheumatology Association's Workforce and Wellness Survey. Journal of Rheumatology 49(6): 635–43. doi:10.3899/jrheum.210990.
Kwok, T.S.H., S. Lake, C.E.H. Barber, S. Katz, C.A. Hitchon, K. Jilkine et al. 2025. Inequities in Fee-for-Service Remuneration Affecting Rheumatologists and Patient-Centered Care Across Canada: An Environmental Scan. Journal of Rheumatology 52(7): 713–20. doi:10.3899/jrheum.2024-1170.
Monti, S., C. Montecucco, S. Bugatti and R. Caporali. 2015. Rheumatoid Arthritis Treatment: The Earlier the Better to Prevent Joint Damage. RMD Open 1: e000057. doi:10.1136/rmdopen-2015-000057.
Nagy, G., L. Gunkl-Toth, A.M. Dorgo and I.B. McInnes. 2025. The Concept of Difficult-to-Treat Disease in Rheumatology: Where Next? Lancet Rheumatology 7(4): e274–89. doi:10.1016/S2665-9913(24)00340-0.
Sraka, G., Z. Ladak, C. Laur, D. To, L. Oliva, C. Barnes et al. 2026. “It's Like a One-Stop-Shop”: A Qualitative Study Exploring Patient Experiences With Interdisciplinary Team-Based Rheumatology Care. Journal of Rheumatology 53(2): 206–12. doi:10.3899/jrheum.2025-0768.
Widdifield, J., B. Kuriya, L.K. King, J. Yang, P. Baer, J. Purvis et al. (in press). Using a Novel Approach to Evaluate the Population-Level Burden of Disability Among Working-Age Individuals With Rheumatoid Arthritis. Journal of Rheumatology.
Widdifield, J., C. Laur, T.S.H. Kwok, L. Oliva, C.T. Appleton, V. Ahluwalia et al. 2025. Evaluating Implementation Context to Prepare for Scaling-Up the Integration of Interdisciplinary Healthcare Providers in Rheumatology Practices: A Rheumatology Workforce Survey. Journal of Rheumatology 53(4): 1–23. doi:10.3899/jrheum.2025-0683.
Widdifield, J., C.S. Moura, Y. Wang, M. Abrahamowicz, J.M. Paterson, A. Huang et al. 2016. The Longterm Effect of Early Intensive Treatment of Seniors With Rheumatoid Arthritis: A Comparison of 2 Population-Based Cohort Studies on Time to Joint Replacement Surgery. Journal of Rheumatology 43(5): 861–68. doi:10.3899/jrheum.151156.
Widdifield, J., K. Tu, J.C. Thorne, C. Bombardier, J.M. Paterson, R.L. Jaakkimainen et al. 2017. Patterns of Care Among Patients Referred to Rheumatologists in Ontario, Canada. Arthritis Care and Research 69(1): 104–14. doi:10.1002/acr.22910.
Widdifield, J., S. Bernatsky, J.E. Pope, B. Kuriya, C.E.H. Barber, L. Eder et al. 2021. Evaluation of Rheumatology Workforce Supply Changes in Ontario, Canada, From 2000 to 2030. Healthcare Policy 16(3): 119–34. doi:10.12927/hcpol.2021.26428.
Widdifield, J., S. Bernatsky, J.E. Pope, V. Ahluwalia, C.E.H. Barber, L. Eder et al. 2020. Encounters With Rheumatologists in a Publicly Funded Canadian Healthcare System: A Population-Based Study. Journal of Rheumatology 47(3):468–76. doi:10.3899/jrheum.190034.
Comments
Be the first to comment on this!
Personal Subscriber? Sign In
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed