
Healthcare Quarterly
Expanding Access to Team-Based Care: Insights from British Columbia’s Nursing Initiatives for Primary Care Program
Abstract
Nurses possess distinct competencies that align with primary care initiatives – yet their integration remains inconsistent. British Columbia's Nursing Initiatives for Primary Care (NIPC) program addresses this gap. Developed in partnership with the British Columbia Ministry of Health and Nurses and Nurse Practitioners of British Columbia, NIPC supports the integration of registered nurses and licensed practical nurses employed by family practices. By providing a structured professional practice framework that includes clinical consultation, education, mentorship and a facilitated online community, NIPC ensures that nurses are well-supported to work to their full scope and demonstrates how policy alignment and targeted professional supports can unlock the full value of nurses.
Introduction
Chronic disease management accounts for up to 70% of healthcare expenditures in Canada, with the majority of these demands being placed on primary care initiatives (Lukewich et al. 2014). Globally, attention has been given to the need to transform health systems to better serve the growing needs of populations, communities and individuals by establishing team-based care models within primary care settings (Swanson et al. 2020). These initiatives are vital as primary care is often the first point of contact within the healthcare system. Despite this emphasis, Canadian health systems have been slow to fully integrate all nursing designations into primary care practice settings. While nurse practitioners (NPs) play a central role in primary care initiatives, the integration of registered nurses (RNs) and licensed practical nurses (LPNs) remains a challenge, leading to missed opportunities to enhance population health. A collaboration between the British Columbia Ministry of Health and the Association for Nurses and Nurse Practitioners of British Columbia (NNPBC) led to the development of the Nursing Initiatives for Primary Care (NIPC) program, a strategic initiative that aims to address this gap. Developed in collaboration with the British Columbia Ministry of Health and NNPBC, NIPC supports the integration of RNs and LPNs into primary care settings.
Background
Historically, RNs and LPNs have played vital roles in primary care, providing essential services such as patient education, chronic disease management, health promotion and preventive care. Before the emergence of modern nursing, nurses primarily worked in the private sector within communities, with private registries dating back to the early 1900s (Whelan 2012). The historical evolution of nurses' roles in primary care reflects health system transformations and medical advancements. As medicine advanced and care provision shifted to hospital settings, nursing largely shifted to these institutions (Whelan 2012). Consequently, the presence of RNs and LPNs in community-based primary care declined. Although NPs have maintained a critical presence in primary care since the 1960s (Klemmer-Lamoureux n.d.), the extent of RN and LPN integration has remained limited. As health systems continue to adapt to the changing needs of individuals, communities and populations, there is renewed recognition of the importance of primary care services and the need to move toward patient-centred, comprehensive care that goes beyond episodic treatment. Reintegrating RNs and LPNs into primary care is crucial for improving access, bettering health outcomes and supporting coordinated, comprehensive interdisciplinary care. This is especially true given nurses' expertise in health promotion, preventative screening, chronic and infectious disease management and acute episodic care (Lukewich et al. 2014; Swanson et al. 2020). Yet, despite ongoing efforts to promote team-based care, integrating RNs and LPNs into these settings remains challenging.
The delay in fully integrating the range of nursing designations into primary care can be attributed to three key factors. First, there is a general lack of understanding of nurses' roles, scope and functions within primary care. For example, research indicates that without clear job descriptions, up to 40% of RNs experience role confusion, with many practising outside their scope of practice (Norful et al. 2017). Similarly, in the absence of adequate administrative staff, RNs can spend as much as 55% of their time on clerical tasks such as billing, filing, booking appointments, answering phones and restocking supplies (Norful et al. 2017). Second, successful role integration depends on the level of trust among other primary care providers, which affects how effectively nurses' roles and scope are maximized in primary care settings (Oelke et al. 2014; Todd et al. 2007). Third, structural barriers also impede the adoption of nursing roles in primary care (Oelke et al. 2014; Swanson et al. 2020). Funding models such as fee-for-service act as barriers, as remuneration often depends on primary care providers seeing the patient directly, which can limit referrals to nursing services (Fraher 2020; Oelke et al. 2014).
Historically, in British Columbia, physicians and NPs operating within fee-for-service or blended payment models were required to cover the full cost of employing RNs and LPNs. Nursing services are not independently billable under a fee-for-service structure, so clinics were required to absorb nursing salaries directly, creating a financial disincentive to nurse integration despite demonstrated benefits to access, continuity and chronic disease management. Recent policy changes, including the Nurse in Practice Program (Government of BC 2025), have addressed this barrier by enabling RNs and LPNs to be hired directly by clinics through government-funded positions. This shift separates nursing employment from physician billings, allowing nurses to function as fully integrated team members rather than cost centres borne by individual practices. While this model has reduced a key structural barrier in British Columbia, jurisdictions that rely exclusively on fee-for-service funding continue to face challenges in sustaining nursing roles without dedicated public funding mechanisms.
Although a welcome change, successful implementation requires additional infrastructure to ensure RNs and LPNs are supported in these settings. While nurses employed by larger health employers have access to various practice support programs and peer networks to facilitate their work, nurses working independently within the Primary Care Networks (PCNs) lack access to similar resources. To address this gap and mitigate other significant barriers to successful RN and LPN integration, NNPBC, the provincial professional nursing association of British Columbia, partnered with the Ministry of Health to launch the NIPC program. This professional practice program provides wraparound supports to RNs and LPNs hired into PCNs as part of the Nurse in Practice Program (Government of BC 2025).
Program Development and Implementation
As a provincial mechanism supporting the BC Nurse in Practice Program (Government of BC 2025), the NIPC program establishes the infrastructure and professional supports necessary to transition and support nurses within primary care teams. By translating policy into practice, the program is facilitating RNs and LPNs to contribute fully to patient care, advancing the province's vision for team-based, longitudinal models of care.
The NIPC program's leadership structure includes a director, a clinical nurse specialist with expertise in primary care and two program managers. This leadership team is augmented by a regional network of practice success consultants (PSCs), who are experienced RNs or LPNs, and serve as dedicated mentors for both nurses and clinic teams.
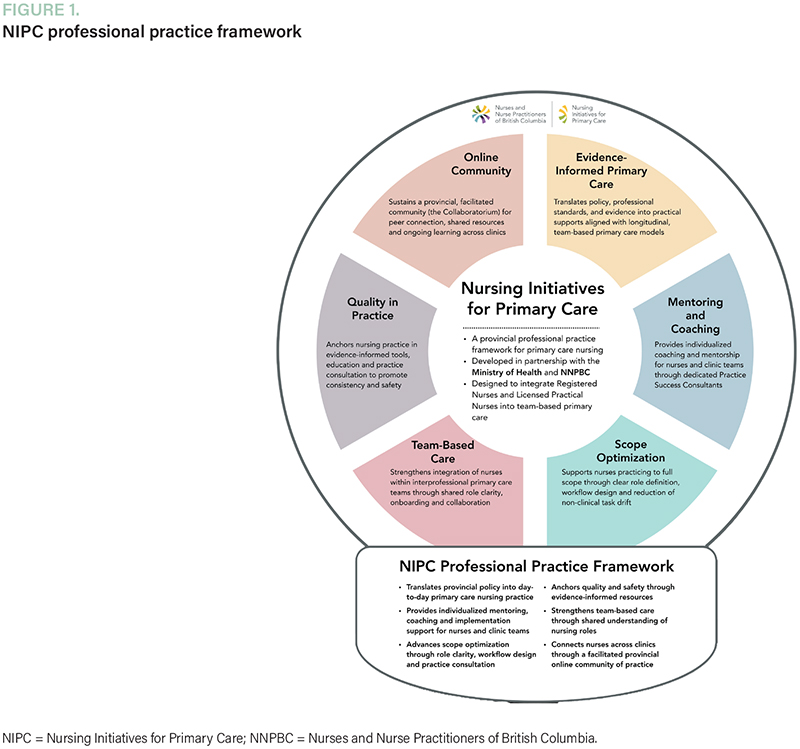
The NIPC program delivers the following two primary types of services (Figure 1):
{kind=link}
- Individualized practice support: PSCs provide one-on-one coaching and mentoring for nurses and clinic leaders. This includes guidance on workflow redesign, scope optimization, care planning and strategies to align nursing roles with clinic objectives. Support may occur through regular virtual check-ins, phone calls or scheduled in-person visits.
- Resource and learning infrastructure: The Collaboratorium, NIPC's online platform, serves as the program's digital backbone. It houses clinical tools, workflow templates, onboarding guides and professional development modules and hosts an interactive nurse-to-nurse community. Through this space, nurses can access on-demand resources, engage in continuous learning and share best practices across regions.

These supports are effectively addressing a longstanding gap for nurses employed directly within private clinics and patient medical homes, practice environments that have historically lacked structural and professional supports for nurses. The Individual Practice Support initiative has had considerable uptake. Four PSCs have been assigned to approximately 81 clinics and 127 nurses, providing tailored, wraparound supports to RNs and LPNs working in these settings. Consultants provide practice support on the scope of practice, workload and workflow, encounter coding, electronic medical record use, onboarding, role clarity, education and professional development. In addition, the clinical nurse specialist hosts monthly community-of-practice meetings with all PSCs to promote information sharing and collaboration among team members. Examples of resources and learning infrastructure include a partnership with Minerva, through which RNs and LPNs can access education on “Advocating for Yourself.” Other collaborations for education include Pain Care British Columbia, Resources for Interdisciplinary Pediatric Practice Learning Child Health and Wound Care with Connecting Learners with Knowledge Team. Another example of learning infrastructure is a recently released encounter coding toolkit (NNPBC n.d.). This initiative included videos and resource documents to support RNs and LPNs in implementing the new recently released encounter codes. Collectively, the two initiatives embedded in NIPC have developed a highly responsive, provincial-level, professional practice support program. Through the NIPC model, nurses now have access to a consistent point of contact, specialized guidance and a province-wide community of practice, fostering professional confidence, strengthening role identity and enhancing capacity for sustained engagement within interprofessional teams.
Evaluation Summary
The NIPC program evaluation aims to understand how the program functions and its impact on nurses' confidence, competence and integration into team-based primary care. Using a mixed-methods approach grounded in the RE-AIM Framework (Reach, Effectiveness, Adoption, Implementation and Maintenance), the evaluation examines who the program reaches, how it is used and the short-term effects on practice. Over the initial three-year period (2024–2027), it will track participation, satisfaction and engagement across all program components, including one-on-one consultations with PSCs, the Collaboratorium online community and the resource library access and impact.
Quantitative data will be drawn from analytics within NNPBC's online platform and digital tracking systems, alongside participant surveys administered at enrolment, three months and annually. These surveys capture participant demographics, satisfaction, relevance and perceived competence. Complementary qualitative methods, including interviews, focus consultations with nursing PSCs and team debriefs, will provide the contextual understanding required to interpret patterns in participation and implementation. Together, these methods will illustrate how nurses are integrating into primary care teams, what supports are most effective and what barriers remain.
The evaluation's structure emphasizes continuous learning. Findings are reviewed annually to identify implementation challenges, highlight facilitators of success and refine subsequent program cycles. This iterative, utilization-focused design ensures that the evaluation is not simply a retrospective report, but an active tool for improvement, supporting evidence-informed adaptation of NIPC as it matures and scales within British Columbia's evolving team-based primary care system.
While it remains early in the program's implementation, with the comprehensive Year 1 evaluation underway, preliminary feedback indicates promising results. Early outcomes, largely self-reported by participating nurses, clinic leaders and PSCs, suggest that the NIPC program is effectively contributing to improvements in role clarity, confidence and collaboration, alongside perceived gains in job satisfaction and care quality. Although these findings are preliminary, they point to the program's potential to strengthen the overall capacity and resilience to advance the province's broader vision for comprehensive, team-based and patient-centred models of care. Beyond this, the program holds potential to meaningfully contribute to retention during a time of considerable workforce challenge.
Discussion
Evidence of impact
Since the program's launch in 2024, over 100 eligible primary care RNs and LPNs from across British Columbia have joined the program, many of whom are the first nurses ever hired at their clinics. New clinics regularly seek advice on role design, onboarding and mentoring. Program analytics indicate a high level of user engagement on the Collaboratorium platform. Hundreds of practice tools and orientation templates have been downloaded by nurses and clinic leaders over the past year, with a steady flow of traffic to discussion boards and learning modules. The materials most frequently downloaded by teams focus on workflow development, chronic disease management and role definition and clarification. The resource library currently offers 40+ practice resources, ranging from clinical decision-making tools and health promotion templates to onboarding checklists and scope-of-practice optimization frameworks. In addition, the team's PSCs offer individualized coaching and mentorship to nurses, both through the online community and in person. These supports contribute to the successful integration of the nurses into their respective clinics while providing a community that would otherwise not exist. Nurses highlight enhanced role clarity and confidence, while physicians experience improved collaboration and follow-up consistency. Early signs point to a model that is both scalable and sustainable as part of British Columbia's primary care transformation.
Implications for system leaders
For system leaders, the NIPC program reinforces that robust primary care can be developed adjacent to acute care systems when the two sectors are viewed as complementary, not competitive. Patients inevitably move between hospital and community settings; however, the design of primary care must reflect its distinct context and patterns of care delivery. The program has shown that when nurses are supported within team-based care environments, through intentional onboarding, clear role definition and access to expert guidance, their role shifts to an essential connector between prevention, treatment and follow-up.
Equally important is recognizing that team-based care depends on professional practice infrastructure. Simply placing nurses in multidisciplinary teams does not guarantee collaboration or quality. Teams function best when every profession is equipped with role clarity, shared language and access to mentorship. NIPC's PSCs and the Collaboratorium provide that structure for nurses, ensuring that they are confident contributors rather than underused generalists.
The partnership model behind NIPC also highlights the value of professional associations. The program alignment with NNPBC provides for deep expertise in nursing practice, education and regulation, complementing the system leadership of government and the practice-based expertise of family physicians and NPs in the primary care environment. This collaborative model shows how association-led practice supports can strengthen team-based care by keeping professional standards and patient needs at the centre of system change.
Systems leaders must realize that the optimization of scope of practice is fundamental to advancing effective primary care. This work includes removing structural and cultural barriers that limit nursing scope while educating other professionals about the full contributions RNs and LPNs can make within primary care. Through policy alignment, association partnership and professional practice supports, NIPC is demonstrating how role clarity can strengthen collaboration and system efficiency across primary care teams.
Lessons learned
Early implementation of NIPC has revealed several areas that are critical for success and sustainability. The first is role clarity and workflow design. Clinics introducing nursing roles must define team-based care principles and role clarity during onboarding. Without this structure, nurses are at risk of being pulled into administrative work, such as booking appointments, ordering supplies and managing day-to-day logistics, rather than providing clinical care. Investing in role definition and workflow planning from the outset is one of the most effective strategies for building clinic capacity.
A second priority is individualized implementation support. Each clinic functions differently, with unique patient populations, systems and team dynamics. NIPC's regional PSCs have proven invaluable as mentors, mediators and guides during onboarding. Their combination of practical coaching and relationship-building helps teams move from uncertainty to confidence. Clinics consistently report that this individualized support made integration smoother and more sustainable.
Peer networks are a third priority. Many clinic-employed nurses work outside the traditional health system structure and can feel professionally isolated. The Collaboratorium, NIPC's online learning and networking platform, provides a vital connection point where nurses share orientation tools, scope optimization guides and problem-solving strategies. Access to this collective expertise fosters consistency, confidence and belonging across dispersed teams.
And finally, a fourth priority is strategic partnerships. Aligning the program with the province's Doctors of British Columbia consultants established early legitimacy and enabled collaboration. This partnership, along with connections to several Divisions of Family Practice and Primary Care Network teams, has demonstrated that sustained progress will rely heavily on strategic partnerships that link policy direction with professional practice expertise, creating a bridge between system priorities and front-line implementation.
Conclusions
Nurses in primary care have an impact. The NNPBC NIPC program offers a scalable framework to facilitate widespread integration of RNs and LPNs into primary care settings. NIPC provides wraparound supports to ensure that nurses can work to the full breadth of their scope. Beyond this, the program ensures that primary care providers understand who nurses are and what nurses do. By facilitating role clarity and workflow design, prioritizing an individualized approach to each setting, creating communities of practice and working in collaboration with key partners, NIPC ensures that clients and communities have access to timely, comprehensive care.
Disclosure Statement
The Nursing Initiatives for Primary Care is funded by the Ministry of Health. Nurses and Nurse Practitioners of British Columbia is the home organization that delivers the program. This manuscript did not receive any external funding. The authors declare no conflicts of interest. All authors meet the criteria of the International Committee of Medical Journal Editors. Artificial intelligence was not used in the development of the manuscript, and this manuscript has not been previously published or is not being considered for publication elsewhere. No authors are members of the Healthcare Quarterly Editorial Board.
About the Author(s)
Patti Telford, RN, BScN, MHS, is a provincial director at Nursing Initiative for Primary Care (NIPC) and Nurses and Nurse Practitioners of British Columbia (NNPBC), Vancouver, BC. Patti is an accomplished nurse leader with extensive experience across a range of clinical areas, with a recent focus on primary care. Her work centres on nursing leadership, program development and health system innovation, with a particular emphasis on advancing nursing roles within interdisciplinary teams and strengthening models of care.
Patti Telford can be reached by e-mail at ptelford@nnpbc.com.
Angela Wignall, RN, BSN, BA, MA, Phd(c), is the chief executive officer at NNPBC, Vancouver, BC. Angela is a nursing leader with experience across all domains of practice. She holds expertise in policy and governance, with a particular emphasis on policy competencies for nursing leaders and clinical governance.
Carly Mann, RN, BScN, MAL, is a provincial manager at Nursing Practice Success and NNPBC, Vancouver, BC. Carly is a values-led nurse leader and systems innovator with 18 years of experience across public, community and Indigenous health. Her work focuses on advancing nursing leadership, program development and evidence-informed, person-centred practice. She is passionate about collaboration, equity and translating strategy into meaningful change that strengthens health systems and supports healthier communities.
Alayna Payne, RN, MN, Phd, is the director of Practice Excellence, Policy & Knowledge at NNPBC, Vancouver, BC. Alayna is a nurse leader and researcher. Her area of scholarship focuses on understanding how nurses construct a professional nursing identity, and the relationship identity shares with job satisfaction and retention.
References
Fraher, E.P. 2020. Primary Care Teams: Past, Present and Future. Journal of the American Board of Family Medicine 33(4): 495–98. doi:10.3122/jabfm.2020.04.200260.
Government of BC. 2025, May 1. Nurse in Practice Program. Retrieved January 2, 2026. <https://www2.gov.bc.ca/gov/content/health/nurse-in-practice-program>.
Klemmer-Lamoureux, D. n.d. History of Nurse Practitioners in Canada. Retrieved October 20, 2025. <https://albertanps.com/history-of-nurse-practitioners-in-canada/>.
Lukewich, J., D.S. Edge, E. Vandenkerkhof and J. Tranmer. 2014. Nursing Contributions to Chronic Disease Management in Primary Care. Journal of Nursing Administration 44(2): 103–10. doi:10.1097/NNA.0000000000000033.
Norful, A., G. Martsolf, K. de Jacq and L. Poghosyan. 2017. Utilization of Registered Nurses in Primary Care Teams: A Systematic Review. International Journal of Nursing Studies 74: 15–23. doi:10.1016/j.ijnurstu.2017.05.013.
Nurses and Nurse Practitioners of British Columbia (NNPBC). n.d. New Encounter Codes for Primary Care Nurses. Retrieved December 5, 2025. <https://codeyourcare.ca/>.
Oelke, N.D., J. Besner and R. Carter. 2014. The Evolving Role of Nurses in Primary Care Medical Settings. International Journal of Nursing Practice 20(6): 629–35. doi:10.1111/ijn.12219.
Swanson, M., S.T. Wong, R. Martin-Misener and A.J. Browne. 2020. The Role of Registered Nurses in Primary Care and Public Health Collaboration: A Scoping Review. Nursing Open 7(4): 1197–207. doi:10.1002/nop2.496.
Todd, C., M. Howlett, M. MacKay and B. Lawson. 2007. Family Practice/Primary Health Care Nurses in Nova Scotia. Canadian Nurse 103(6): 23–27.
Whelan, J. 2012. When the Business of Nursing Was the Nursing Business: The Private Duty Registry System, 1900–1940. The Online Journal of Issues in Nursing 17(2): 6.
Comments
Be the first to comment on this!
This article is for subscribers only. To view the entire article
Related Articles

Note: Please enter a display name. Your email address will not be publically displayed